149 서 론
생체 간이식은 뇌사자로부터의 공여 간의 부족으로 시작
되었지만, 1990년대에 이미 말기 간질환의 확립된 치료법 의 하나로 자리를 잡았다. 처음 생체 간이식은, 뇌사자 대기 시간이 긴 소아에게 어머니로부터 좌외구역을 이식하는 데 에서 시작했다.(1,2) 소아 생체 간이식의 경험이 축적되면서 차츰 그 영역이 확대되어, 1990년대 중반 이후에는 대사 요 구량이 큰 성인 수혜자에 우간 이식을 시작하였고, 이식 성 적은 뇌사자 간이식과 견줄 수 있게 되었다.(3-5) 이러한 생 체 간이식의 눈부신 발전은 공여자와 수혜자 모두에서 간 의 해부학 및 수술 중 혈액학적 변화에 대한 이해, 수술 술 기 및 수술 전후 관리의 발전에 의하였다. 본고에서 저자들 은, 지난 15년간의 생체 간이식 술기의 다양한 변화와 발전 에 초점을 맞추어 기술하고자 한다.
공여자 수술
1) 간의 해부학
생체 간 공여자의 수술은 수혜자에게 적절한 용적의 이
Technical Evolution in Living Donor Liver Transplantation
Nam-Joon Yi, M.D. and Kyung-Suk Suh, M.D.
Department of Surgery, Seoul National University College of Medicine, Seoul, Korea
During the last 15 years, much progress has been made in the technical aspect of living donor liver transplantation (LDLT). In fact, LDLT has contributed to understanding of the detailed anatomy of the liver and performing more precise hepatectomy. Recently, more complex cases which were relative contraindications for liver transplantation such as Budd-Chiari syndrome and portal vein thrombosis have been challenged in LDLT area. This review focuses on donor hepatectomy and hanging maneuver in the donor, and hilar dissection and venous reconstruction in the recipient. In addition, recent technical advances in complex cases were also introduced. Biliary complication has been the most common, intractable complication to disturb the quality of life of the long-term survivors. Reduction of its complication rate is a pending question of the transplant surgeon. In LDLT, donor safety is paramount. Technical innovations should be balanced with any unexpected harm to the donors. (J Korean Soc Transplant 2006;20:149-159)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Living donor liver transplantation, Donor hepa-
tectomy, Hanging maneuver, Outflow recon- struction, Portal vein thrombosis
중심 단어: 생체 간이식, 공여자 간절제술, 간 현수법, 간정맥 재건, 문맥 혈전
생체 간이식 술기의 변화와 발전
서울대학교 의과대학 외과학교실 이 남 준․서 경 석
책임저자:서경석, 서울시 종로구 연건동 28 서울대학교 의과대학 외과학교실, 110-744 Tel: 02-2072-3789, Fax: 02-766-3975 E-mail: [email protected]
Fig. 1. The inflow of the portal vein and hepatic artery does not parallel the outflow of the hepatic vein. The inflow structure enters the center of each segment but the outflow of the hepatic vein usually lies between segments (Ref. 7, Fig. 1).
RHV = right hepatic vein; MHV = middle hepatic vein; ISV
= scissural vein; LHV = left hepatic vein; RP = right posterior section; RA = right anterior section; Sg4 = segment 4; LL = left lateral section; PV = portal vein.
RP RA
Sg4
LL
Left PV
RA-PV
RP-PV
150 대한이식학회지:제 20 권 제 2 호 2006
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 식편을 제공하면서 동시에 공여자의 안전을 저해하지 않아
야 하기 때문에, 외과의에게 가장 까다로운 수술 중의 하나 이다. 일반적으로 간세포암 등으로 간을 절제하는 경우, 절 제되어 나가는 부분에 대해서는 유입되는 혈류와 유출되는 혈류의 균형을 생각할 필요가 없다. 그러나 생체 간이식에 서는, 이식편과 공여자의 잔존 간 모두에서 혈류 유입과 유 출의 균형을 유지하여야 하는 어려움이 있다.(6) 간문맥과 간동맥혈은 간의 각 구역 중앙으로 유입되지만 간정맥은 각 구역 사이로 유출된다(Fig. 1).(7) 즉 우간문맥과 동맥은 우전구역과 우후구역으로, 좌간문맥과 동맥은 좌내구역과 좌외구역으로 유입되지만, 우간정맥은 우후구역과 우전구 역 일부를, 중간간정맥은 우전구역 일부와 좌내구역 일부 를, 그리고 좌간정맥은 좌외구역과 좌내구역 일부를 유출 시킨다. 중간간정맥이 공여자의 좌간에 남게 되는 고전적 인 우간이식편에서는, 이식편의 우전구역 유출로가 없어지 기 때문에 우전구역 울혈이 발생하게 된다(Fig. 2C). 때로는 이로 인하여 이식편 부전으로 수혜자의 생명을 위협하기도 한다.(8)
2) 이식편의 종류 및 적절한 이식편의 용적
공여자 간절제술은, 이러한 간 해부학의 아이러니 때문 에 고난도의 술기를 요하며 일반적인 간절제술의 명명법과 조금 다른 개념이 필요하다. 지금까지 알려진 공여자 간절 제술의 종류는, 2번 또는 3번 분절을 이용하는 단분절절제 술(monosegmentectomy, segment 2 or 3), 좌외구역절제술(left lateral sectionectomy), 확대좌외구역절제술(extended left late-
ral sectionectomy), 좌간절제술(left hepatectomy), 확대좌간절 제술(extended left hepatectomy), 우간절제술(right hepatecto- my), 변형우간절제술(modified right hepatectomy), 변형확대 우간절제술(modified extended right hepatectomy), 확대우간 절제술(extended right hepatectomy), 우후구역절제술(right posterior sectionectomy)이 있다.
공여자 간절제술의 기술은, 브리즈번 2000 용어집에(9) 소개된 용어 체계를 사용하여, 간실질 구역과 이식편 내에 어떤 간정맥이 포함되는지에 따라 달라진다. 좌외구역은 최초의 생체 간이식에서 소아에게 수혜된 이식편이다.(1,2) 좌외구역절제술과 연관된 공여자의 안전성은 확립되어 있 으며, 소아 수혜자에게 적절한 용적의 이식편이다. 좌외구 역이식편은 좌간문맥과 동맥 및 좌간정맥이 포함되므로 이 식편 내에서는 허혈이나 울혈의 문제가 발행하지 않지만, 공여자에게 잔존하는 좌내구역과 미상엽에 허혈이 발생하 며 이는 수술 후 공여자의 간효소 증가와 연관되어 있다 (Fig. 2A).(10) 체구가 큰 소아 수혜자에서는 확대좌외구역 혹은 좌간절제술을 시행할 수 있고, 확대좌외구역절제술은 좌외구역과 좌내구역 일부를 포함하는 수술이며, 좌간절제 술은 온전한 좌간절제술이며, 이 두 수술은 중간간정맥을 이식편에 포함하지 않기 때문에 이식편 좌내구역에 울혈을 유발할 수 있다.
생체 간이식을 포함한 부분 간이식에서 적절한 이식편의 무게는, 수혜자 몸무게 대비(graft versus recipient weight ratio, GRWR) 0.8∼1% 이상이 되어야 안전하다.(11,12) 성인 의 간은 대략 몸무게의 2% 정도이고 우간이 전체 간용적의
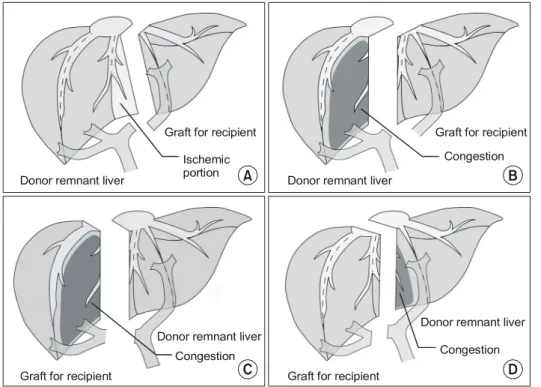
Fig. 2. Various types of donor he- patectomy (Ref. 7, Fig. 2).
(A) Left lateral sectionect- omy. There is usually no is- chemia and congestion in the graft, but the left medial section and a part of cau- date lobe become ischemic in the remnant liver of the donor. (B) Extended left he- patectomy. This graft has a good inflow and outflow, but the right anterior sec- tion becomes congested in the remnant liver of the do- nor. (C) Right hepatectomy.
The right anterior section wi- thout the middle hepatic vein becomes congested when the graft is reperfused. (D) Ext- ended right hepatectomy.
A B
D C
Donor remnant liver
Ischemic portion Graft for recipient
Donor remnant liver
Graft for recipient Congestion
Graft for recipient
Congestion Donor remnant liver
Graft for recipient
Congestion Donor remnant liver
60∼70%를 차지하며, 좌외구역이 17% 정도를 차지한 다.(13) 대개의 건강한 성인 공여자의 좌외구역은 소아 수 혜자에게, 그리고 좌간 이하의 이식편은 작은 체구의 성인 수혜자에게 적절한 이식편 용적을 제공하므로 임상적인 문 제를 일으키지 않는다. 소아에서는 오히려 GRWR이 4% 이 상이 되면, 상대적으로 큰 이식편에 적절한 혈류 공급이 되 지 않거나 복강 내 공간이 협소하여 폐복이 어렵고 이식편 이 압박되기 때문에, 신생아 혹은 6 kg 이하의 영아에서는 단분절이식편을 사용하기도 한다.(14,15) 그러나 체구가 큰 성인 수혜자에서 좌간은 대사 요구량을 만족시키기 어렵 다. 성인 수혜자에서 이식편 용적의 부족을 해결하기 위해 서, 초기에는 확대좌간절제술에 미상엽을 합병절제하기도 하였다.(16) 확대좌간이식편은(Fig. 2B) 중간간정맥 및 우전 구역 일부와 미상엽을 포함하게 되므로, 기능적 용적은 고 전적인 좌간이식편에 비해서 크다. 그러나 체구가 큰 성인 수혜자에서는 여전히 이식편 용적이 부족한 경우가 많다.
고전적인 우간절제술은(Fig. 2C) 중간간정맥을 구득하지 않 기 때문에, 우전구역 울혈과 관련하여 기능적인 이식편 용 적이 작아지고 이식편 부전의 문제들을 야기할 수 있다.
HongKong group에서 제시한 확대우간절제술은,(5) 좌내구 역 일부를 포함하여 중간간정맥을 구득하기 때문에 이식편 의 허혈이나 울혈의 문제가 없고 충분한 이식편 용적을 확 보할 수 있어서 성인 수혜자에게 있어서 가장 이상적인 이 식편이라고 할 수 있다(Fig. 2D). 그러나 생체 간이식에서 가장 우선시 되어야 하는 공여자 안전 확보라는 관점에서 문제점이 지적된다.(17) 이러한 문제를 해결하기 위해 저자 들은, 좌내구역을 온전히 공여자측에 보존하여 잔존 간 용 적을 최대한 확보하면서 중간간정맥을 구득하는 변형확대 우간절제술(modified extended right hepatectomy)을 보고하
였다(Fig. 3).(6) 그러나 잔존 간의 좌내구역 울혈로 인한 공 여자의 초기 잔존 간 재생이 원활하지 못하다는 문제점을 극복하지 못했다.
아직 논란의 여지가 있지만, 공여자의 안전을 보장하기 위한 최소한의 잔존 간 용적은 적어도 전체 간 용적의 30%
이상이어야 하고,(18,19) 울혈이나 허혈의 문제가 없어야 한 다. Lee 등(8,20)은, 공여자의 기능성 잔존 간을 최대한 보장 하면서 동시에 성인 수혜자에게도 충분한 이식편을 제공할 수 있는 방법으로 변형우간절제술을 제시하였다. 공여자의 간절제술은 고전적인 우간절제술과 동일하지만, 중간간정 맥으로 유입되는 5 mm 이상의 5분절과 8분절 간정맥을 보 존하여 벤치에서 간치혈관을 문합하게 된다. 간치혈관으로 는 수혜자의 자가 정맥(복재 정맥, 하장간막정맥, 문맥 등), 공여자의 정맥(복재 정맥, 난소 정맥 등), 뇌사자로부터 구 득한 냉동보존혈관(장골 동맥 혹은 정맥 등)을 사용할 수 있다.(21-25)
공여자의 좌간이 전체 간용적의 30% 이하이고 우후구역 의 용적이 좌간보다 커서 수혜자의 표준 간용적의 40% 이 상을 보이는 경우, 드물지만 우후구역을 이식편으로 쓸 수 있다.(26) 그러나 우후구역절제는 술기가 까다롭고, 수술 후 수혜자에서 담즙 누출 등의 합병증이 빈발하며, 실제로 측 정하는 이식편의 무게는 수술 전 추정한 용적보다 작은 경 우가 있다.(7,27,28) 또한 우후구역절제는 우후구역으로 유 입되는 혈관과 담도의 해부학적 접근 용이성을 담보하여야 하므로 적응 범위가 넓지 않다.(26-29) Fig. 4에서와 같이, 우전구역의 문맥지는 좌간 문맥에서 기시하고 우후구역 문 맥지는 따로 우측에서 기시하며(Fig. 4A), 담도와 간동맥에 비슷한 변형이 있는 경우(Fig. 4B), 우후구역절제술의 적응 증이 될 수 있다.
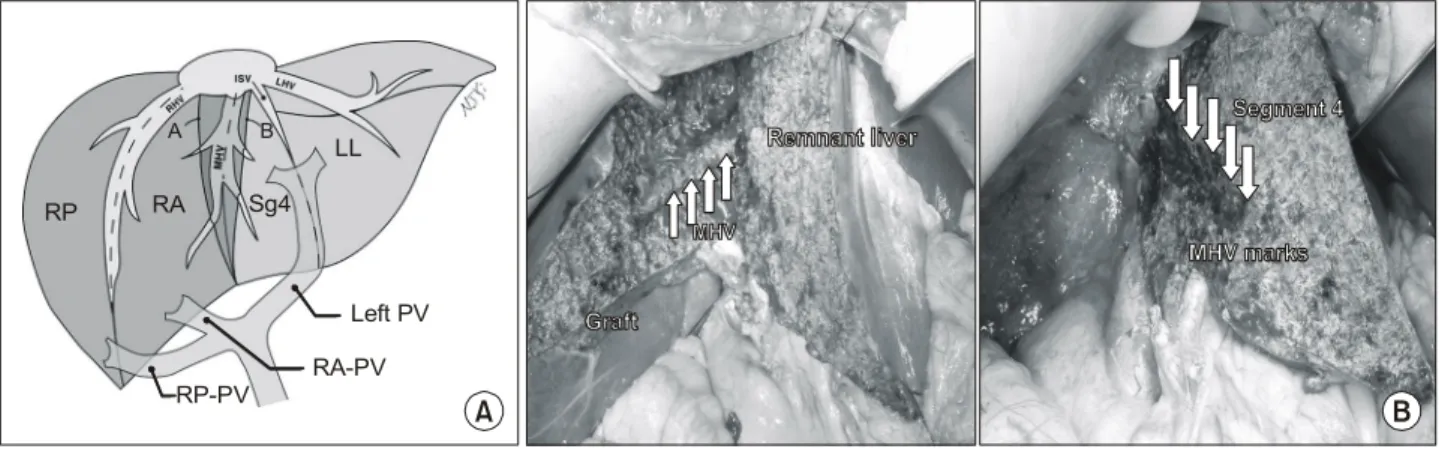
Fig. 3. Modified extended right hepatectomy (MERH)(Ref. 3, Fig. 3). (A) Line (A) represents the transection line for MERH, which is the same as that use in right hepatectomy, whereas line (B) is used for extended right hepatectomy. (B) Harvest of the middle hepatic vein (MHV) in MERH. The MHV was excavated leaving all of segment 4 on the donor side. RHV = right hepatic vein;
MHV = middle hepatic vein; ISV = scissural vein; LHV = left hepatic vein; RP = right posterior section; RA = right anterior section; Sg4 = segment 4; LL = left lateral section; PV = portal vein.
A B
RP RA Sg4
LL
Left PV RA-PV RP-PV
A B
152 대한이식학회지:제 20 권 제 2 호 2006
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
3) 간 현수기법(Hanging maneuver)
안전한 간절제를 위해서는 간의 구동화가 가장 기본적인 기술이다. 그러나 종양이 횡격막을 침윤했거나 우간에 거 대한 종양이 있을 경우 간의 구동화는 쉽지 않다. 또한 간의 구동화 과정에서, 병소가 압박되어 종양의 파종 위험이 증 대되고 반대측 간을 압박하는 단점이 있다. HongKong group에서는(30,31) 이러한 환자에서 복측에서 하대 정맥을 향하여 간을 절리하는 전방절제술(anterior approach)을 이용 하여 간의 구동 없이 우간절제술을 시행하였다. 그러나, 전 방절제술에서 심부 간절리는 용이하지 않다. Belghiti 등(32) 은 전방절제술의 단점을 보완하기 위하여 현수기법를 도입
하였다. 현수기법은, 하대 정맥의 전방과 간 후방 사이에 테 이프를 걸어 간을 하대정맥으로부터 들어 올리는 것이다.
이를 통해 전방절제 시 정확한 간의 절리면을 유도하고, 심 부에서의 절리와 지혈을 용이하게 한다. 현수기법은 안전 을 최우선으로 하는 공여자 간절제술에서도 매우 유용한 기법으로, 최근 생체 간이식 공여자 이식편 구득에도 도입 되었다.(33,34)
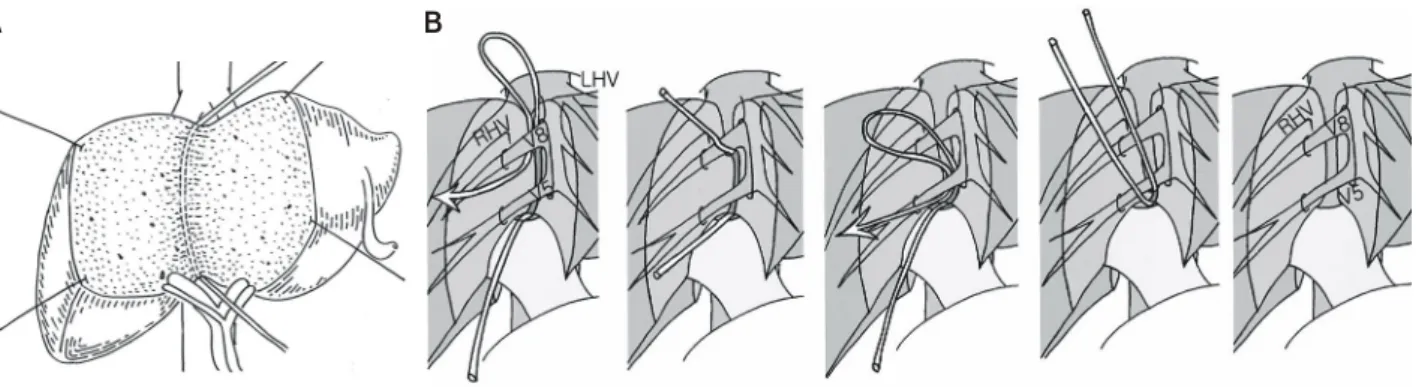
공여자 우간절제술을 할 때에는 우간을 구동하여 우간정 맥과 하대정맥을 완전히 노출한 후 현수테이프를 건다. 현 수테이프는 우간정맥과 중간간정맥의 사이를 통과하여 간 후방과 하대정맥 전방의 공간에 놓이게 되고, 최종적으로 우간문부의 전방을 통과한다. 미상엽이 절리된 후 현수테
Fig. 5. Hanging maneuver in donor right hepatectomy (Ref. 7, Fig. 5). (A) Insertion of the tape into the anterior surface of the inferior vena cava from between the right hepatic vein and the middle hepatic vein down to the inferior edge of caudate lobe under direct vision after fully mobilizing the right liver. After the caudate lobe inferior to hilum is transected, the tape is pulling out above from the hilar plate. (B) A gradual tape-repositioning of the tape behind the major tributaries of the middle hepatic vein. RHV
= right hepatic vein; V5 = the segment V hepatic vein; V8 = the segment VIII hepatic vein; LHV = left hepatic vein.
A B
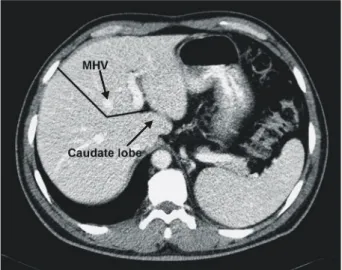
Fig. 4. Preoperative imaging study in living donor liver transplantation using the right posterior section (Ref. 7, Fig. 4). (A) Preoperative computerized tomography. The black arrow indicates the right anterior portal vein that originates from the umbilical portion of the left portal vein. The white arrow indicates the right posterior portal vein. (B) Intraoperative cholangiography. The arrowhead shows the right posterior hepatic duct, which was separated in the extra-hepatic area.
A B
이프를 복측으로 당기고 양측간의 사방을 견인하면 우간의 심부 절리면이 유도된다(Fig. 5A). Kokudo 등(33)은 단계적 현수법을 소개하였는데, 중간간정맥의 분지를 보존하는 변 형우간절제술에 적용할 수 있다(Fig. 5B).
공여자 확대좌간절제술은 미상엽은 절제하지 않고 중간 간정맥을 포함하여 절리해야 하기 때문에, 심부 절리면은 미상엽 전방에서 급격하게 방향을 바꾸게 된다(Fig. 6). 이 때 정확한 심부 절리면을 찾기 위해서 현수기법을 이용하 면 보다 안전하고 용이하게 간절제를 할 수 있다.(34) 좌간 정맥 외측에서 중간간정맥과 좌간정맥의 공통간을 박리하 여 현수테이프를 건 후, 현수테이프의 한쪽은 정맥인대를
따라 간의 미측으로 돌려서 좌간문부를 통과하도록 한다 (Fig. 7). 간실질은 전방에서 후방으로 수직으로 절리를 시 작하고, 미상엽 전방에 도달하면 절리면이 좌측 수평으로 방향 전환이 되므로, 이때 현수테이프를 들어 심부 절리면 을 유도한다.
수혜자 수술
1) 간적출술
생체 간이식에서 수혜자의 문맥이나 제대 정맥 등은, 문맥 이나 간정맥의 문합 시 혈관의 구경을 넓히거나 변형우간 이식편에서 중간간정맥 유출로를 재건하기 위한 patch 등으 로 이용된다. 한편 이식편의 혈관이나 담도는, 2개 이상 다 발성이거나 길이가 짧고 구경이 작은 경우가 종종 있다. 따 라서 수혜자의 간문부를 처리할 때는, 가능하면 좌우 간동 맥과 문맥을 가능한 충분히 길게 박리하고, 담도는 혈류의 손상 없이 좌우간관 개구 부위까지 유지하는 것이 필요하 다. 그러나 수혜자는 대개 문맥압 항진증이 있거나 과거에 각종 시술이나 수술을 받은 경우가 많기 때문에, 이러한 간 문부 처리는 실혈량도 많고 시간도 오래 걸린다.
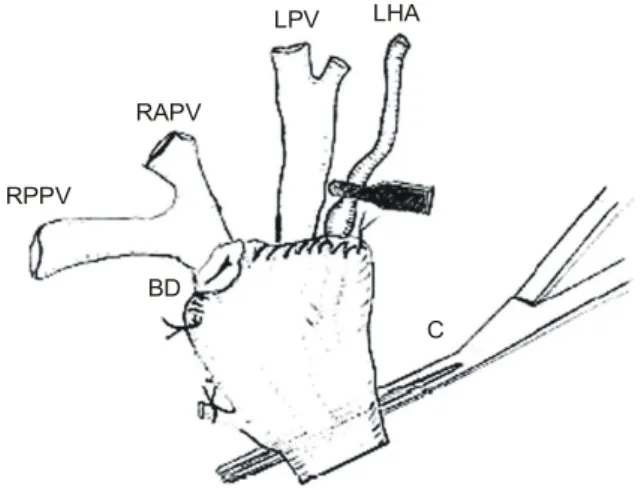
고위 간문부 박리술(high hilar dissection)은,(35) 간문부를 혈관겸자로 한 번에 차단한 후 간실질에 연하여 담도, 간동 맥, 문맥을 한꺼번에 절리한 후 말단 부위에서부터 문합이 필요한 부분만 선택적으로 박리하고 그 외의 부분은 봉합 하는 방법이다(Fig. 8). 고위 간문부 박리술은 담도 주위 조 직을 보존하여 담도-담도 문합술 시 담도 합병증을 줄이는 목적으로 고안되었는데, 실제로 간문부 박리 시 실혈량을 줄이고 적절한 크기와 수의 혈관 문합부를 얻기에 유용한 방법이다. 선택적 문맥 차단술(selective portal clamp techni- que)(36) 역시 담도 합병증을 줄이는 방법으로 고안되었는 데, 간문부의 각 구조물을 가장 말단 부위에서 결찰한 후 간동맥과 담도는 분리하지 않고 문맥만 기저부에서 혈관 겸자로 차단하는 방법이다(Fig. 9). 담도와 간동맥을 분리하 Fig. 6. A transection line for the extended left hepatectomy (Ref.
7, Fig. 6). One is a vertical plane that extends from the anterior surface of the liver down to the immediate right of the middle hepatic vein (MHV). When the parenchymal dissection approaches the superior part of caudate lobe, the plane of dissection turns sharply to the left and becomes horizontal.
Fig. 7. Hanging maneuver in the extended left hepatectomy (Ref. 7, Fig. 7). (A) The tape behind the common trunk of the MHV and LHV in order to make the horizontal plane dissection easier. (B) Easy pass of the tape behind the common trunk after division of the ligamentum venosum.
MHV = middle hepatic vein;
LHV = left hepatic vein;
IVC = inferior vena cava.
Common trunk of MHV and LHV
A B
IVC
MHV+LHV Caudate
lobe
Ligamentum venosum
154 대한이식학회지:제 20 권 제 2 호 2006
ꠏ ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
지 않기 때문에 온허혈 기간에도 수혜자의 담도에 혈류가 유지시키면서 문맥 문합이 용이한 장점이 있다.
2) 간정맥의 재건
충분한 유출로의 재건은 생체 간이식의 성공 유무를 결 정하는 중요한 과정이다. 물론 유출로의 재건 시 술기상 문
제가 없다고 하더라도, 이식편이 놓이는 위치와 이식편 재 생에 따른 혈관 비틀림 현상 등이 관여할 수 있다.
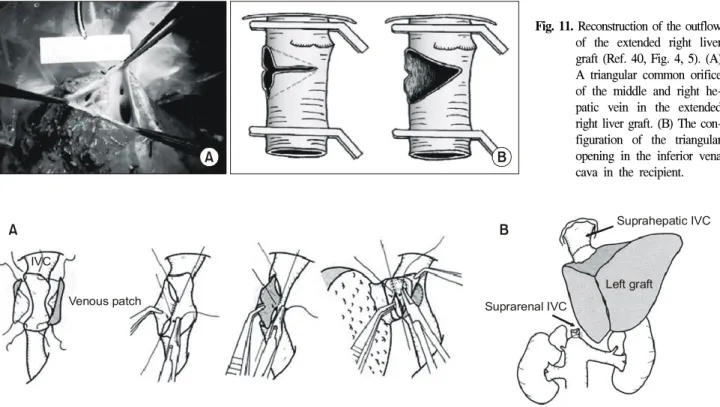
작은 소아에서 성인 공여자로부터 얻은 이식편의 좌간정 맥은 소아의 중간 및 좌간정맥 공통강의 구경보다 큰 경우 가 있다. 이런 경우, 우간정맥과 함께 열어서 구경을 넓히거 나 중간간정맥과 좌간정맥 공통강을 하대정맥 전벽으로 넓 혀서 사용할 수 있다(Fig. 10).(7,37) Makuuchi와 Sugawara (38)는 좌간이식편 경우, 이식편 자체에 의한 하대정맥의 압박과 이식편이 재생하는 동안에 우배측으로 회전하는 비 틀림 현상으로 유출 혈류에 장애를 일으킬 수 있음을 지적 하고, 충분히 넓은 유출로 재건이 필수적이라고 하였다. 우 간은 우상복부에 놓이게 되므로 좌간에 비하여 하대 정맥 압박이나 비틀림의 정도가 덜하지만 이식편의 재생과 연관 된 비틀림 현상은 우간이식편의 재생에도 적용된다.(39,40) 이러한 점에 착안하여 HongKong group에서는, 확대우간이 식편의 중간간정맥 재건을 초기에는 수혜자의 중간간정맥 에 연결하였으나, 최근에는 우간정맥과 중간간정맥을 공통 강으로 만들고 그 사이의 중격에는 v자 모양의 홈을 내어서 큰 하나의 유출로를 만든 후(Fig. 11A), 수혜자의 하대정맥 에 넓은 삼각형 구멍을 내어 연결하는 방법을 사용한다 (Fig. 11B).(40) Sugawara 등(39)과 Malago 등(41)은 중간간정 맥의 말단에 정맥 patch를 대어서 수혜자에 문합하는 유출 로를 넓게 만드는 방법을 소개하기도 하였다. 그러나 확대 우간절제술이나 변형확대우간절제술은 공여자의 안전성을 담보하기 어렵기 때문에 세계적으로 널리 이용되는 술기가 아니고 제한된 조건에서만 시행하고 있다.
변형우간이식편에서 간치혈관을 두어 중간간정맥 분지 를 재건하는 적응증에 대해서는 다양한 견해가 있지만, 5번 과 8번 분절의 중간간정맥 분지 구경이 5 mm 이상이고, 수 술 전 컴퓨터 단층촬영으로 예측한 우전구역 울혈의 정도 나 수술 중 중간간정맥 분지와 간동맥을 동시에 결찰하여 우전구역 울혈이 심각한 경우 적응증이 되며, 공여자의 나 Fig. 10. Incising the inferior vena cava lateral to the middle hepatic
vein for widening an orifice (Ref. 7, Fig. 8).
A B
Fig. 8. High hilar dissection for the recipient's hepatectomy (Ref.
35, Fig. 2). The portal vein is isolated from hepatic pedicle and clamped separately with a vascular clamp (C). Long portal vein branches are seen. Left hepatic artery is dissected and clipped with a black clamp. After selection of the proper bile duct for the duct-to-duct anastomosis, the hilar plate of remaining pedicles is sutured with continuous nonabsorbable suture. RPPV = right posterior portal vein;
RAPV = right anterior portal vein; LPV = left portal vein;
LHA = left hepatic artery; BD = bile duct.
RAPV
RPPV
BD
C
LPV LHA
Fig. 9. Selective portal clamp technique (Ref. 36, Fig. 1). The bile duct was not clamped, but selected above the bifurcation to maintain blood supply. The hepatic artery was also ligated at the top of the hilum without clamping, and the portal vein was separately clamped at the bottom with a vascular clamp. MPV = main portal vein; PHA = proper hepatic artery; CBD = common bile duct.
MPV
CBD PHA
이와 이식편의 지방변성 정도, GRWR 등을 고려하여야 하 겠다.(42-45) 최근 개발된 여러 가지 수술 기법으로 과거에 비하여 비교적 수월하게 중간간정맥 분지의 재건이 가능하 기 때문에, 기능적 이식편 용적을 최대한 확보하기 위해서 적극적으로 고려하여야 하겠다.
Budd-Chiari 증후군은 하대정맥, 간정맥 및 문맥의 해부 학적 구조의 변형 및 혈전으로 인해서 생체 간이식은 기술 적인 어려움이 따른다. 최근 Yamada 등(46)은 Budd-Chiari 증후군 환자의 생체 간이식 중 간정맥 유출로 재건 술기에 관하여 보고하였다. 섬유화로 두꺼워진 하대정맥의 전방벽 과 간정맥을 가능한 한 제거하고 수혜자의 자가 정맥 patch 등을 이용하여 하대정맥성형술을 시행하거나(Fig. 12A), 하 대정맥의 대부분이 혈전이나 섬유화가 진행되어 부대정맥 이 발달한 경우에는 하대정맥을 결찰 절리하여 이식편의 간정맥을 직접 하대정맥과 단단문합할 수 있다(Fig. 12B).
아울러 Budd-Chiari 증후군 환자의 반수 이상은 기저에 혈 액응고 기능이 항진되어 있기 때문에 이식 후에도 지속적 인 항응고치료를 요한다고 하였다.
3) 간문맥 문합
과거에는 문맥 혈전이 있거나 문맥이 없는 경우 간이식의 상대적인 금기증이었다. 특히 생체 간이식에 있어서는 이
식편의 혈관이 짧고 구경이 작으며, 대치할 수 있는 혈관이 제한되어 있기 때문에 어려움이 있다. 최근 Egawa등(47)은 문맥 혈전을 가진 수혜자에서의 생체 간이식 경험을 보고 하였다. 수혜자의 문맥을 이용하는 경우에는, 단순 문맥 혈 전 제거술 후 문맥대 문맥 문합을 하거나 문맥을 완전 절리 후 혈전을 제거하고 간치혈관을 두어 연결하였다. 수혜자 의 문맥을 결찰하는 경우에는, 하대정맥을 부분 우회하여 사용하거나, 수혜자 자가 정맥이나 냉동보존 혈관을 이용 한 jump graft를 상장간막정맥이나 좌신정맥에 연결하였다.
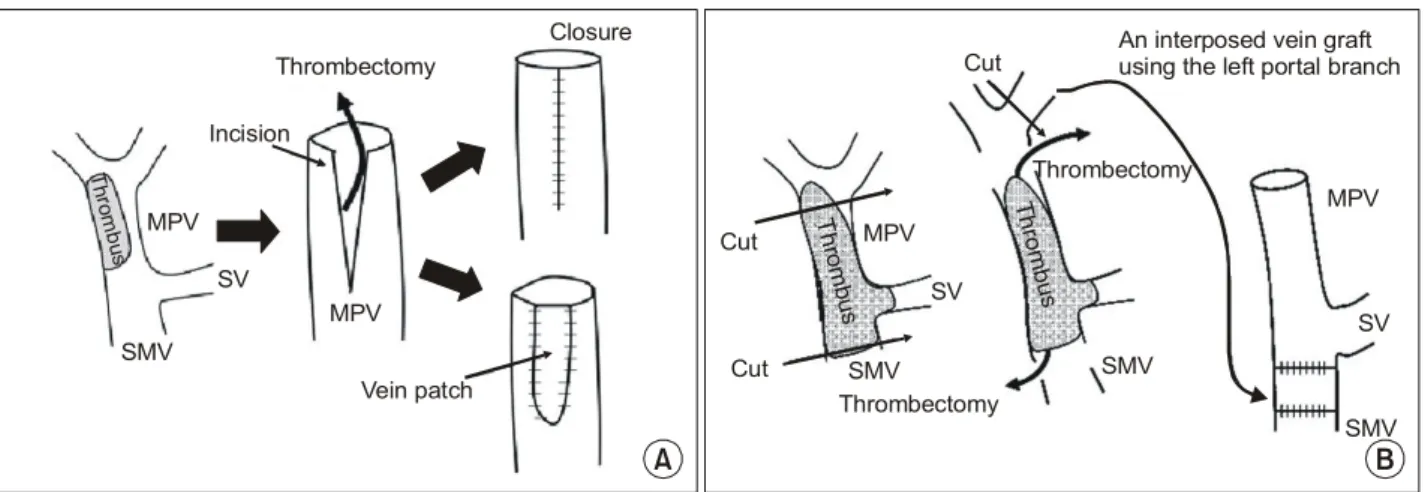
문맥혈전 제거 방법으로는 문맥을 외전시켜서 직접 제거하 는 방법과 문맥에 절개를 넣어 제거하는 방법(Fig. 13A), 혹 은 혈전이 상장간막정맥과 비장정맥까지 진행되어 있는 경 우 상장간막정맥을 열고 혈전을 밀어낸 후 직접 단단 문합 하거나 patch를 대는 방법을 제시하였다(Fig. 13B). 그러나 문맥 혈전의 진행 정도와 MELD 점수에 따라 여전히 간문 맥 혈전은 상대적인 생체 간이식 금기증임을 지적하였다.
4) 간동맥의 문합
생체 간이식에 있어서 간동맥 문합은 초기에는 간이식편 의 소실에 중대한 위험 인자였으나 미세 동맥재건술이 도 입된 이후(48)에 간동맥 합병증은 3∼5% 정도로 개선되었 다. 그러나 부분 간이식편의 간동맥은 길이가 짧고 구경이 Fig. 12. Surgical techniuqe for plasty of the occluded inferior vena cava (IVC) in Budd-Chiari syndrome (Ref. 46, Fig. 4, 6). (A) Cavoplasty of IVC and right heapatic vein reconstruction using patch plasty with vein grafts. (B) Direct anastomosis between suprahepatic intact IVC and graft hepatic vein after transection of suprarenal IVC.
Venous patch IVC
Left graft
Suprahepatic IVC
Suprarenal IVC
A B
Fig. 11. Reconstruction of the outflow of the extended right liver graft (Ref. 40, Fig. 4, 5). (A) A triangular common orifice of the middle and right he- patic vein in the extended right liver graft. (B) The con- figuration of the triangular opening in the inferior vena cava in the recipient.
A B
156 대한이식학회지:제 20 권 제 2 호 2006
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
작은 데다가 다발성인 경우가 종종 있다. 수혜자는 대개 문 맥압 항진증이 있고, 간세포암 환자에서는 여러 차례의 간 동맥 색전술을 시행하였거나, 과거 복부 혹은 간절제 수술 력이 있는 경우 등으로 인해서 간동맥의 질이 좋지 않은 경우가 많다. 수혜자의 간동맥이 좋지 않은 경우, 대치 혈관 으로 뇌사자에서 구득한 냉동 보존된 장골동맥 등은 직경 이 크고 혈관벽이 두꺼워서 생체 간이식편의 간동맥과 직 접 문합하기 어렵다. 이에 다양한 대치 혈관으로 비장동맥, S자 결장동맥, 요골동맥 등이 소개되었는데, 그 중에서 비 교적 간편하게 대치할 수 있는 혈관으로 우위대망동맥이 있다(Fig. 14).(49,50)
5) 담도 문합 술기
많은 생체 간이식 센터에서는 성인간 생체 간이식에서
기존의 담도-공장문합 대신에 여러 생리적인 이점을 지닌 담도대 담도 문합을 하고 있다. 담도대 담도 문합은 괄약근 을 가진 수혜자의 담도를 그대로 이용하는 생리적인 이점 외에도 장을 이용하는 담도-공장 문합에 비하여 문합이 간 단하고 수술 시간이 단축되기 때문에, 장기 성적이 보고되 기 이전에 이미 널리 이용되기 시작하였다.(36,51) 담도대 담도 문합의 초기 성적은 담도-공장문합에 견줄만하였으나 최근 장기 성적 보고에서 문합부 협착이 문제점으로 부상 하였다.(36,52) 문합부 협착을 줄이기 위해서 수혜자의 담도 혈류를 보존하는 고위 간문부 박리술과 선택적 문맥 결찰 술이 소개되었고, 이외에도 이식편과 반대측의 간동맥을 Fig. 13. Thrombectomy of the portal vein (Ref. 47, Fig. 2, 3). (A) Incision technique. (B) Thrombectomy by superior mesenteric vein dissection followed by reconstruction with an interposed vein graft using the left portal vein. MPV = main portal vein; SV = splenic vein; SMV = superior mesenteric vein.
Throm bus
SMV SV MPV
Incision
MPV Thrombectomy
Closure
Vein patch
An interposed vein graft using the left portal branch
Cut
Cut
MPV
SV
SMV Throm
bus
Thrombectomy
SMV Thr
ombus
Thrombectomy Cut
MPV
SV
SMV
A B
Fig. 14. Hepatic artery anastomosis using the recipient's right gast- roepipolic artery (RGEA) in the right liver graft (Ref. 50, Fig. 1).
Rt. graft
RGEA
Fig. 15. Contra-lateral arterial anastomosis in the recipient (Ref.
36, Fig. 2). To improve blood supply to the anastomosis site, the right hepatic artery is not used for the right graft and vice versa. Rt = graft, right graft; G-RHA = the right hepatic artery of the graft; R-LHA = the left hepatic artery of the recipient.
Rt.graft
G-RHA
R-LHA
박리하여 문합하는 방법 등이 소개되었다(Fig. 15).(36) 담도 를 문합하는 구체적인 술기와 문합 후 담도 배액관의 삽입 여부에 대해서도 아직은 정론이 없다.
6) 두개의 이식편을 이용한 간이식
Lee 등(53,54)은 공여자의 간우엽의 비율이 70% 이상으 로 우간을 구득할 수 없거나, 공여자의 간용적이 작아서 체 구가 큰 수혜자의 대사 요구량을 만족시키지 못하거나, 혹 은 공여자가 중등도 이상의 지방간이 있는 경우에 2명의 공여자에게서 이식편을 수혜하는 성인 생체 간이식을 보고 하였다(Fig. 16). 그러나 2개의 이식편을 이용한 생체 간이 식은, 2명의 생체 공여자를 확보하여야 하며, 공여자 각각 의 합병증을 감수하여야 하고, 술기상의 어려움이 있기 때 문에 널리 사용되고 있지 않다.(18)
결 론
생체 간이식은 지난 15년간 눈부신 발전을 거듭하여, 현 재는 뇌사 공여자를 이용한 간이식과 함께 모든 말기 간질 환 환자의 치료법으로 자리 잡았다. 특히 이식 외과의의 노 력으로 이루어진 술기의 개발과 발전은 이러한 발전에 중 심에 있었고, 앞으로도 계속되리라고 기대한다. 다만, 생체 간이식의 발전을 도모함에 있어서 인류애에 기초한 공여자 의 안전이 제일 부동의 원칙으로 지켜져야 할 것이다.
REFERENCES
1) Raia S, Nery JR, Mies S. Liver transplantation from live donors. Lancet 1989;2:497.
2) Strong RW, Lynch SV, Ong TH, Matsunami H, Koido Y,
Balderson GA. Successful liver transplantation from a living donor to her son. N Eng J Med 1990;322:1505-7.
3) Hashikura Y, Makuuchi M, Kawasaki S, Matsunami H, Ikeg- ami T, Nakazawa Y, Kiyosawa K, Ichida T. Successful living- related partial liver transplantation to an adult patient. Lancet 1994;343:1233-4.
4) Yamaoka Y, Washida M, Honda K, Tanaka K, Mori K, Shi- mahara Y, Okamoto S, Ueda M, Hayashi M, Tanaka A. Liver transplantation using a right lobe graft from a living related donor. Transplantation 1994;57:1127-30.
5) Lo CM, Fan ST, Liu CL, Wei WI, Lo RJ, Lai CL, Chan JK, Nq IO, Fung A, Wong J. Adult-to-adult living donor liver transplantation using extended right lobe grafts. Ann Surg 1997;226:261-9.
6) Suh KS, Yi NJ, Cho JY, Kwon CH, Minn KW, Lee KU.
Technical refinement preserving segment 4 to donor in extend- ed right hepatectomy. Hepatogastroenterology 2006;53:253-7.
7) Suh KS. Technical variations in living donor liver transplan- tation. Curr Opin Orang Transpl 2004;9:90-8.
8) Lee S, Park G, Hwang S, Lee Y, Choi D, Kim K, Koh K, Han S, Choi K, Hwang K, Makuuchi M, Sugawara Y, Min P. Congestion of right liver graft in living donor liver trans- plantation. Transplantation 2001;71:812-4.
9) Belghiti J, Clavien PA, Gadzijev E, Garden JO, Lau WY, Ma- kuuchi M, Storng RW. The Brisbane 2000 terminology of liver anatomy and resections. HPB 2000;2:333-9.
10) Suh KS, Kim SH, Kim SB, Lee HJ, Lee KU. Safety of right lobectomy in living donor liver transplantation. Liver Transpl 2002;8:910-5.
11) Kiuchi T, Kasahara M, Uryuhara K, Inomata Y, Uemoto S, Asonuma K, Egawa H, Fujita S, Hayashi M, Tanaka K. Impact of graft size mismatching on graft prognosis in liver transplan- tation from living donors. Transplantation 1999;67:321-7.
12) Sugawara Y, Makuuchi M, Takayama T, Imamura H, Dowaki S, Mizuta K, Kawarasaki H, Hashizume K. Small-for-size grafts in living-related liver transplantation. J Am Coll Surg 2001;192:510-3.
13) Leelaudomlipi S, Sugawara Y, Kaneko J, Matsui Y, Ohkubo T, Makuuchi M. Volumetric analysis of liver segments in 155 living donors. Liver Transpl 2002;8:612-4.
14) Kasahara M, Kaihara S, Oike F, Ito T, Fujimoto Y, Ogura Y, Ogawa K, Ueda M, Rela M, D Heaton N, Tanaka K. Living donor liver transplantation with monosegments. Transplanta- tion 2003;76:694-6.
15) Shirouzu Y, Kasahara M, Morioka D, Sakamoto S, Taira K, Uryuhara K, Ogawa K, Takada Y, Egawa H, Tanaka K.
Vascular reconstruction and complications in living donor liver transplantation in infants weighing less than 6 kilograms: the Koyto experience. Liver Transpl 2006;12:1224-32.
16) Miyagawa S, Hashikura Y, Miwa S, Ikegami T, Urata K, Terada M, Kubota T, Nakata T, Kawasaki S. Concomitant cau- date lobe resection as an option for donor hepatectomy in adult Fig. 16. Dual graft living donor liver transplantation using two left
lobes (Ref. 54, Fig. 5). (A) The orthotopical left liver graft. (B) The heterotopical left liver graft. HV = hepatic vein; PV = portal vein; BD = bile duct; HA = hepatic artery; H-J stomy = hepaticojejunostomy.
Duct-duct anastomosis
Vein graft
HV
B A
Hepatic duct for HJstomy Tissue
expander
BD HA
PV
158 대한이식학회지:제 20 권 제 2 호 2006
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ living related liver transplantation. Transplantation 1998;66:
661-3.
17) Fan ST, Lo CM, Liu CL, Wang WX, Wong J. Safety and necessity of including the middle hepatic vein in the right lobe graft in adult-to-adult live donor liver transplantation. Ann Surg 2003;238:137-48.
18) Cho JY, Suh KS, Kwon CH, Yi NJ, Lee HH, Park JW, Lee KW, Joh JW, Lee SK, Lee KU. Outcome of donors with a remnant liver volume of less than 35% after right hepatectomy.
Liver Transpl 2006;12:201-6.
19) Lee SG. Asian contribution to living donor liver transplan- tation. J Gastroenterol Hepatol 2006;21:572-4.
20) Lee S, Park K, Hwang S, Kim K, Ahn C, Moon D, Joo J, Cho S, Oh K, Ha T, Yang H, Choi K, Hwang K, Lee E, Lee Y, Lee H, Chung Y, Kim M, Lee S, Suh D, Sung K. Anterior segment congestion of a right liver lobe graft in living donor liver transplantation and strategy to prevent congestion. J Hepatobiliary Pancreat Surg 2003;10:16-25.
21) Cattral MS, Greig PD, Muradali D, Grant D. Reconstruction of middle hepatic vein of a living-donor right lobe liver graft with recipient left portal vein. Transplantation 2001;71:1864-6.
22) Lee KW, Lee DS, Lee HH, Joh JW, Choi SH, Heo JS, Lee SK, Kim SJ. Interposition vein graft in living donor liver transplantation. Transplant Proc 2004;36:2261-2.
23) Dong G, Sankary HN, Malago M, Oberholzer J, Panaro F, Knight PS, Jarzembowski TM, Benedetti E, Testa G. Cada- veric iliac vein outflow reconstruction in living donor right lobe liver transplantation. J Am Coll Surg 2004;199:504-7.
24) Sugawara Y, Makuuchi M, Akamatsu N, Kishi Y, Niiya T, Kaneko J, Imamura H, Kokudo N. Refinement of venous re- construction using cryopreserved veins in right liver grafts.
Liver Transpl 2004;10:541-7.
25) Hwang S, Lee SG, Ahn CS, Park KM, Kim KH, Moon DB, Ha TY. Cryopreserved iliac artery is indispensable interpo- sition graft material for middle hepatic vein reconstruction of right liver graft. Liver Transpl 2005;11:644-9.
26) Sugawara Y, Makuuchi M, Takayama T, Imajura H, Kaneko J. Right lateral sector graft in adult living-related liver trans- plantation. Transplantation 2002;73:111-4.
27) Kim SH, Suh KS, Kim SB, Lee HJ, Lee KU. Adult living donor liver transplantation using right posterior segment. Tran- spl Int 2003;16:689-91.
28) Hwang S, Lee SG, Lee YJ, Park KM, Kim KH, Ahn CS, Sung KB, Moon DB, Ha TY, Kim KK, Kim YD. Donor selection for procurement of right posterior segment graft in living do- nor liver transplantation. Liver Transpl 2004;10:1150-5.
29) Cheng YF, Huang TL, Lee TY, Chen TY, Chen CL. Variation of the intrahepatic portal vein; angiographic demonstration and application in living-related hepatic transplantation. Transplant Proc 1996;28:1667-8.
30) Lai EC, Fan ST, Lo CM, Chu KM, Liu CL. Anterior approach for difficult major right hepatectomy. World J Surg 1996;20:
14-7.
31) Liu CL, Fan ST, Lo CM, Poon RTP, Wong J. Anterior ap- proach for major right hepatic resection for large hepatocel- lular carcinoma. Ann Surg 2000;232:25-31.
32) Belghiti J, Guevara OA, Noun R, Saldinger PF, Kianmanesh R. Liver hanging maneuver: a safe approach to right hepatec- tomy without liver mobilization. J Am Coll Surg 2001;193:
109-11.
33) Kokudo N, Sugawara Y, Imamura H, Sano K, Makuuchi M.
Sling suspension of the liver in donor operation: a gradual tape-repositioning technique. Transplantation 2003;76:803-7.
34) Suh KS, Lee HJ, Kim SH, Kim SB, Lee KU. Hanging man- euver in left hepatectomy. Hepatogastroenterology 2004;51:
1464-6.
35) Lee KW, Joh JW, Kim SJ, Choi SH, Heo JS, Lee HH, Park JW, Lee SK. High hilar dissection: new technique to reduce biliary complication in living donor liver transplantation. Liver Transpl 2004;10:1158-62.
36) Yi NJ, Suh KS, Cho JY, Kwon CH, Lee KU. In adult-to-adult living donor liver transplantation hepaticojejunostomy shows a better long-term outcome than duct-to-duct anastomosis. Tran- spl Int 2005;18:1240-7.
37) Sato Y, Yamamoto S, Takeishi T, Nakatsuka H, Kokai H, Ha- takeyama K. New hepatic vein reconstruction by double ex- pansion of outflow capacity of left-sided liver graft in living- donor liver transplantation. Transplantation 2003;76:882-4.
38) Makuuchi M, Sugawara Y. Living-donor liver transplantation using the left liver, with special reference to vein reconstru- ction. Transplantation 2003;75:S23-4.
39) Sugawara Y, Makuuchi M, Sano K, Imamura H, Kaneko J, Ohkubo T, Matsui Y, Kokudo N. Vein reconstruction in modi- fied right liver graft for living donor liver transplantation. Ann Surg 2003;237:180-5.
40) Liu CL, Zhao Y, Lo CM, Fan ST. Hepatic venoplasty in right lobe live donor liver transplantation. Liver Transpl 2003;9:
1265-72.
41) Malago M, Molmenti EP, Paul A, Nadalin S, Lang H, Radtke A, Liu C, Frilling A, Biglamia R, Broelsch CE. Hepatic ven- ous outflow reconstruction in right live donor liver transplan- tation. Liver Transpl 2005;11:364-5.
42) Hwang S, Lee SG, Park KM, Kim KH, Ahn CS, Lee YJ, Sung KB, Moon DB, Ha TY, Cho SH, Oh KB, Han JM, Kim MH.
Hepatic venous congestion in living donor liver transplan- tation: preoperative quantitative prediction and follow-up using computed tomography. Liver Transpl 2004;10:763-70.
43) Akamatsu N, Sugawara Y, Kaneko J, Sano K, Imamura H, Kokudo N, Makuuchi M. Effects of middle hepatic vein recon- struction on right liver graft regeneration. Transplantation 2003;
76:832-7.
44) de Villa VH, Chen CL, Chen YS, Wang CC, Lin CC, Cheng YF, Huang TL, Jawan B, Eng HL. Right lobe living donor liver transplantation-addressing the middle hepatic vein contro-
versy. Ann Surg 2003;238:275-82.
45) Maetani Y, Itoh K, Egawa H, Shibata T, Ametani F, Kubo T, Kiuchi T, Tanaka K, Konishi J. Factors influencing liver regeneration following living-donor liver transplantation of the right hepatic lobe. Transplantation 2003;75:97-102.
46) Yamada T, Tanaka K ,Ogura Y, Ko S, Nakajima Y, Takada Y, Uemoto S. Surgical technique and long-term outcomes of living donor liver transplantation for Budd-Chiari syndrome.
Am J Transpl 2006;6:2463-9.
47) Egawa H, Tanaka K, Kasahara M, Takada Y, Oike F, Ogawa K, Sakamoto S, Kozaki T, Taira K, Ito T. Single center ex- perience of 39 patients with preoperative portal vein throm- bosis among 404 adult living donor liver transplantations.
Liver Transpl 2006;12:1512-8.
48) Mori K, Nagata I, Yamagata S, Sasaki H, Nishizawa F, Takada Y, Moriyasu F, Tanaka K, Yamaoka Y, Kumada K. The introduction of microvascular surgery to hepatic artery recons- truction in living donor liver transplantation-its surgical advan- tages compared with conventional procedures. Transplantation 1992;54:263-8.
49) Ikegami T, Kawasaki S, Hashikura Y, Miwa S, Kubota T, Mita
A, Iijima S, Terada M, Miyagawa S, Furuta S. An alternative method of arterial reconstruction after hepatic artery throm- bosis following liver transplantation. Transplantation 2000;69:
1953-5.
50) 이승은, 이남준, 서경석, 권준혁, 민경원, 이건욱. 생체 부분 간 이식에서 수여자의 우 위대망동맥을 이용한 간동맥 문합. 한 국간담췌외과학회지 2005;9:102-5.
51) Ishiko T, Egawa H, Kasahara M, Nakamura T, Oike F, Kaihara S, Kiuchi T, Uemoto S, Inomata Y, Tanaka K. Duct-to-duct biliary reconstruction in living donor liver transplantation uti- lizing right lobe graft. Ann Surg 2002;236:235-40.
52) Hwang S, Lee SG, Sung KB, Park KM, Kim KH, Ahn CS, Lee YJ, Lee SK, Hwang GS, Moon DB, Ha TY, Kim DS, Jung JP, Song GW. Long-term incidence, risk factors, and management of biliary complications after adult living donor liver transplantation. Liver Transpl 2006;12:831-8.
53) Lee S, Hwang S, Park K, Lee Y, Choi D, Ahn C, Nah Y, Koh K, Han S, Park S, Min P. An adult-to-adult liver transplantation using dual left lobe grafts. Surgery 2001;129:647-50.
54) 이승규. 생체 부분 간이식. In: 박용현, 김선회, 이건욱, 서경석 편집. 간담췌외과학. 제2판. 서울, 의학문화사; 2006. p.582.