Cystic lymphangioma is a benign tumor of the lym- phatic system which usually occurs in the skin and sub- cutaneous region of the head and axilla. However, a small portion of cystic lymphangiomas have been re- ported in various regions of the abdomen including the stomach, jejunum, colon, pancreas, and the mesentery (1-3). Among them, cystic lymphangiomas of the stom- ach are considered very rare. In effect, fewer than 50 cases have been reported in the English literature (4).
The majority of these reports were related with endo- scopic and surgical findings (1-4). To our knowledge, no report describes the findings of cystic lymphangioma of the stomach demonstrated by multidetector-row computed tomography (MDCT) using multiplanar refor- mation. Here, we report the MDCT findings of a patient diagnosed with cystic lymphangioma of the stomach.
Case Report
A 46-year-old man was admitted with abnormal gas- tric endoscopy findings. At the time of screening, the pa- tient had no symptoms or any previous remarkable medical history, including gastritis or peptic ulcer dis- ease. Also, a physical and routine laboratory examina- tion, including a complete blood count and chemistry profile, was unremarkable. The gastric endoscopy ex- amination showed a well-defined lobulated mass with normal covering mucosa. The size was of the mass was about 3.5 cm in diameter and was located in the greater curvature side of the gastric antrum (Fig. 1A). The lesion was soft enough to be compressed with biopsy forceps.
Hence, the examining gastroenterologist concluded that the most probable diagnosis of this lesion would be a be- nign submucosal tumor (e.g. gastrointestinal stromal tu- mor or cystic lesion).
After admission, an enodoscopic ultrasonography (EUS) was performed for further characterization of the lesion. The EUS was performed using the EUM-30 en- doscope (Olympus, Japan). The results of the EUS
J Korean Radiol Soc 2008;59:261-264
─ 261 ─
Multidetector-Row CT Findings of Gastric Cystic Lymphangioma: A Case Report1
Tae Wook Kang, M.D., Soon Jin Lee, M.D., Hye Jong Song, M.D.2
1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea
2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea
Received July 11, 2008 ; Accepted August 18, 2008
Address reprint requests to : Soon Jin Lee, M.D., Department of Radiology, Samsung Medical Center, School of Medicine, Sungkyunkwan University, 50 Ilwon-dong, Kangnam-gu, Seoul 135-710, Korea Tel. 82-2-3410- 3864 Fax. 82-2-3410-2559 E-mail: [email protected]
Cystic lymphangioma is a rare benign submucosal tumor of the stomach thought to originate from sequestered lymphatic tissue that fails to communicate with the normal lymphatic system. The most commonly used method of evaluation for cystic lym- phangioma of the stomach is an endoscopic ultrasonography. We report the multide- tector-row computed tomography findings of a cystic lymphangioma of the stomach in a 46-year-old man along with a literature review.
Index words :Lymphangioma, cystic Stomach
Tomography, X-Ray Computed
demonstrated that the lesion had a homogeneous ane- choic cystic mass confined to the submucosal layer. In addition, no septation or solid component was identified within the lesion (Fig. 1B). Next, a MDCT was per- formed to assess the extent of the lesion as well as the associated findings in the abdomen. The CT scan was performed using a MDCT scanner (Lightspeed VCT, GE Healthcare, Milwaukee, WI, U.S.A.) with 64 detectors.
MDCT scans were obtained using the following para- meters: 290 mA, 120 kVp, a section thickness of 5 mm, a reconstruction interval of 5 mm, and a pitch of 0.984:1. The direct multiplanar reformation function
was used to generate coronal and sagittal reformations using a section thickness of 3 mm as well as a recon- struction interval of 3 mm. For the axial image, a 3.5 cm low density mass was demonstrated in the anterior wall of the gastric antrum (Fig. 1C). In addition, the sagittal reformation showed the mass with a smooth surface and a broad base on greater curvature side of the gastric antrum. Moreover, it had a thin enhancing wall cover- ing representing the normal mucosal layer and was con- fined to the stomach (Fig. 1D). We could clarify an exact extent and location of the lesion using a multiplanar re- formation of the MDCT. The mean Hounsfield unit
Tae Wook Kang, et al: Multidetector-Row CT Findings of Gastric Cystic Lymphangioma
─ 262 ─
A B
C D
Fig. 1. A. The gastric endoscopy examination indicates a well-defined lobulated mass with normal covering mucosa in the greater curvature side of the gastric antrum (arrow).
B. The endoscopic ultrasonography revealed a homogeneous anechoic cystic mass confined to the submucosal layer (arrow). No in- ternal septation or solid component was present within the lesion.
C. The MDCT axial image shows a small low density mass (arrows) in the anterior wall of the gastric antrum, which has a thin en- hancing wall covering representing the normal mucosal layer.
D. The sagittal reformation image shows the mass (arrow) with a smooth surface and a broad base on the greater curvature side of the gastric antrum, which is confined to the stomach.
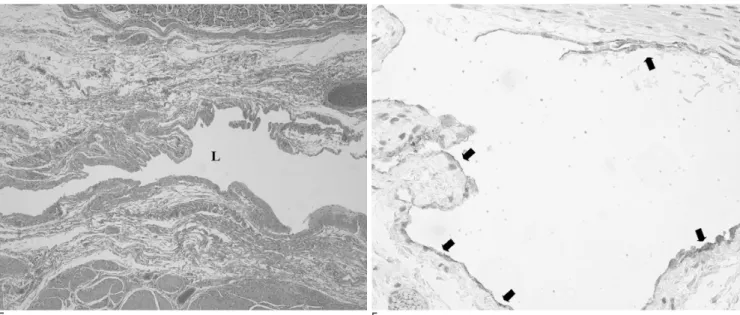
(HU) of the low density portion of the mass was about 20 HU. This measurement represented the cystic mass, which was slightly higher than gastric fluid. Moreover, there was no perigastic fat infiltration around the mass and regional lymph node enlargement. Considering these imaging findings, we considered a duplication cyst, ectopic pancreas with cystic change, cystic lym- phangioma, and other benign tumors with cystic change as part of the suite of differential diagnosis. The patient underwent a wedge resection of the stomach. Upon light microscopic examination, unusual dilated lymphat- ic channels were identified in the submucosal area (Fig.
1E). The overlying endothelial cells of the lymphatic channels were positive for D2-40, which represented a lymphatic endothelial immunohistochemical marker (Fig. 1F). These findings were consistent with cystic lymphangioma. After surgery, the patient was dis- charged without any complications.
Discussion
Cystic lymphangioma is a benign malformation of the lymphatic system. The vast majority (-95%) of lym- phangiomas are found in the neck and axilla regions.
Other locations include the mediastinum, omentum, mesentery, retoroperitooneum and bone (5). Cystic lym- phangioma of the stomach and duodenum is very rare.
Histologically, this lesion consists of irregularly dilated lymphatic channels lined with benign-appearing en- dothelial cells. Cystic lymphangioma are thought to be
developmental malformations arising from sequestered lymphatic tissue (6). Furthermore, these lesions often have a cystic appearance because of the progressive ac- cumulation of fluid.
Clinically, most cases of cystic lymphangiomas are asymptomatic and are detected incidentally. On occa- sion, they are large enough to cause obstruction or intus- susception, depending on the size and location of the mass (7). A cystic lymphangioma can be demonstrated as a submucosal tumor with overlying normal musoca by a gastric endoscopy. However, it is difficult to differ- entiate cystic lymphangioma from other submucosal tu- mors such as leiomyoma, lipoma, carcinoid tumor, soli- tary submucosal varix, as well as others (8). As a result, the EUS has become a standard tool in assessing gastric submucosal tumors since it can provide an assessment of the internal components of submucosal tumors in the stomach (4). Tsai et al. (9) reported that the characteristic EUS findings of cystic lymphangiomas were anechoic cystic lesions located in the submucosal layer with mul- tiple inner septations. As a result, the conventional CT could not delineate the inner septations due to poor im- age resolution compared with EUS. In effect, cystic lym- phangioma may appear as a non-enhancing submucosal mass with an internal homogeneous low density which renders it difficult to differentiate from other cystic le- sions of the stomach (e.g., enteric duplication, resolving hematoma, necrotic tumor, and cystic change of the het- erotopic pancreas) (10).
Recently, the introduction of MDCT enables the accu-
J Korean Radiol Soc 2008;59:261-264
─ 263 ─
E F
Fig. 1. E, F. The light microscopic examination reveals a large lymphatic channel (L) with flat endothelial cells (E) (H & E stain, × 40) which are positive for D2-40 (F) (arrows) (× 200).
rate evaluation of the type of stomach tumor. A MDCT also provides improved spatial resolution, which in turn provides good quality multiplanar reformation com- pared to the single detector CT. In our case, a MDCT properly demonstrated the extent and location of cystic lymphangioma and its internal component; however, no internal septation was seen in the cystic mass on MDCT findings. This was consistent with our EUS and patho- logic findings. The treatment of gastric cystic lymphan- gioma depends on the size, location, and complications associated with the tumor. In the case of a large lesion, surgical resection is usually the modality of choice.
However, observation or endoscopic manipulation is al- so considered as possible treatment modalities in the case of small cystic lesions (8).
In this case report, we describe the MDCT findings of cystic lymphangioma in the stomach using a multipla- nar reformation. Although cases of gastric cystic lym- phangioma are highly unusual, it should be considered in the differential diagnosis of the various types of cystic lesions of the stomach. Cystic lymphangioma is present- ed as a well-defined low density cystic lesion with an in- tact overlying thin normal mucosa with or without in- ternal septations on MDCT.
References
1. de Perrot M, Rostan O, Morel P, Le Coultre C. Abdominal lym- phangioma in adults and children. Br J Surg 1998;85:395-397 2. Drago JR, DeMuth WE Jr. Lymphangioma of the stomach in a
child. Am J Surg 1976;131:605-606
3. Gockel I, Muller H, Kilic M, Eitelbach F, Gaedertz C, Peters H.
Giant cystic lymphangioma of the stomach. Eur J Surg 2001;167:
927-930
4. Ishikawa N, Fuchigami T, Kikuchi Y, Kobayashi H, Sakai Y, Nakanishi M, et al. EUS for gastric lymphangioma. Gastrointest Endosc 2000;52:798-800
5. Singh S, Baboo ML, Pathak IC. Cystic lymphangioma in children:
report of 32 cases including lesions atrrare sites. Surgery 1971;69:947-951
6. Davis M, Fenoglio-Preiser C, Haque AK. Cavernous lymphan- gioma of the duodenum: case report and review of the literature.
Gastrointest Radiol 1987;12:10-12
7. Ramsay GS. Enterogenous cyst of the stomach simulating hyper- trophic pyloric stenosis. Br J Surg 1957;44:632-633
8. Kim HS, Lee SY, Lee YD, Kim DH, Kwon JG, Tak WY, et al.
Gastric lymphangioma. J Korean Med Sci 2001;16:229-232 9. Tsai CY, Wang HP, Yu SC, Shun CT, Wang TH, Lin JT.
Endoscopic ultrasonographic diagnosis of gastric lymphangioma. J Clin Ultrasound 1997;25:333-335
10. Park SH, Han JK, Kim TK, Lee JW, Kim SH, Kim YI, et al.
Unusual gastric tumors: radiologic-pathologic correlation.
Radiographics 1999;19:1435-1446
Tae Wook Kang, et al: Multidetector-Row CT Findings of Gastric Cystic Lymphangioma
─ 264 ─
대한영상의학회지 2008;59:261-264
위에 생긴 낭성 림프관종의 MDCT 소견: 증례 보고1
1삼성서울병원 영상의학과, 2삼성서울병원 병리과
강태욱・이순진・송혜정2
낭성 림프관종은 위에 생기는 드문 점막하 종양으로 정상적인 림프계와의 연결이 되지 않은 격리된 림프 조직들 에서 발생한다. 이제까지 내시경을 통한 초음파를 이용하여 낭성 림프관종에 대한 평가가 주로 보고되었다. 이에 저 자들은 46세 남자 환자에서 생긴 낭성 림프관종의 MDCT 소견에 대해 기술하고 관련된 문헌에 대해 고찰하고자 한다.