J. Exp. Biomed. Sci. 2013, 19(1): 70~78 pISSN : 1738-3226
The Effects of Beta-blocker and Aerobic Exercise on Heart Rate Recovery and Exercise Capacity after Maximal Exercise in
Acute Coronary Syndrome Patients
Kyung-Hwa Cha1, Jae-Keun Oh1 and Young-Joo Kim2,†
1Department of Health and Exercise Science, Korea National Sport University, Seoul 138-763, Korea
2Department of Rehabilitation Medicine, Sanggye-Paik Hospital, Seoul 139-707, Korea
This study was conducted to identify the effects of intake of beta-blocker and aerobic exercise on heart rate recovery (HRR) and exercise capacity after maximal exercise in acute coronary syndrome patients (ACS). Subjects were divided into 4 groups; Beta-blocker-Exercise group (n=10), Beta-blocker group (n=10), Exercise group (n=10), Control group (n=10). Symptom-limited grade exercise test were conducted on subjects pre- and post- 6 week study, to measure maximal heart rate, heart rate at 1 minute and 2 minutes at the recovery stage, maximal oxygen uptake and maximal exercise time. Study resulted in significant improvements in heart rate recovery for BB-Ex group (17.40 ± 5.58 bpm to 26.10 ± 6.66 bpm), maximal oxygen uptake for BB-Ex group (30.46 ± 8.63 to 36.33 ± 8.10) and Ex group (29.04
± 4.93 to 34.31 ± 5.19), and total exercise time for BB-Ex group (906.30 ± 158.57 to 1018.50 ± 151.21), BB group (805.70 ± 182.94 to 897.50 ± 160.16) and Ex group (870.00 ± 145.63 to 961.90 ± 107.29). Therefore it showed the biggest improvement for heart rate recovery and exercise capacity in acute coronary syndrome patients when both Beta-blocker and aerobic exercise were in effect.
Key Words: Beta-blocker, Aerobic exercise, Heart rate recovery, Acute coronary syndrome, Percutaneous transluminal coronary angioplasty, Maximal oxygen uptake, Maximal exercise time
서 론
급성관상동맥증후군 (acute coronary syndrome, ACS)은 죽상경화반의 파열 및 변화된 관상동맥, 염증반응, 혈소 판의 응집과 혈전현상에 의해 임상적으로 불안정 협심증, 비 ST 분절 상승 심근경색이나 ST 분절 상승 심근경색으 로 발현되는 것 (Shah, 1997)을 말한다. 최근 성공적인 관 상동맥 중재술 후에도 재협착 (restenosis)을 포함한 심장 질환 재발이 시술받은 환자의 약 30~50%에서 발생되고 있다. 생명에 치명적인 심근경색증의 경우, 처음 발생했 을 때는 사망률이 20~30%에 불과하지만, 치료 후 다시
재발하는 경우에는 68~85%로 사망률이 훨씬 증가하게 됨 (Black & Matassarin-Jacobs, 1997)을 고려해 볼 때, 관상 동맥질환에 대한 일차예방뿐만 아니라 재발방지를 위한 근본적인 대책마련이 시급하다. 운동이 중심이 되는 심장 재활 (cardiac rehabilitation) 프로그램은 관상동맥질환자에 있어 사망률과 재발률을 낮추는 것으로 잘 알려져 있으 며 (Thompson et al., 2003) 환자의 삶의 질을 개선하는 프 로그램이다 (Lavie, 1993; Blair, 1989). 운동 트레이닝은 심 장병 환자들의 최대산소섭취량 (VO
2max)과 운동 능력을 향상시킬 뿐만 아니라, 자율 신경계 기능, 혈류량, 골격 근 기능 등을 향상시키며 (Jette et al., 1991; Giannuzzi et al., 1993) 환자들의 회복과 생존률을 높여 준다 (Keteyian et al., 1997). 운동 수행 능력의 장애 정도는 심장이식과 사 망률 및 회복의 중요한 예측인자로 활용되고 있으며 (Yeo et al., 2001) 운동 후 심박수의 회복은 심질환의 예 후를 예측하는데 유용한 지표가 된다 (Kim et al., 2004).
운동 강도의 증가에 따른 심박수의 증가는 부교감신경
*Received: December 31, 2012 / Revised: March 19, 2013 Accepted: March 21, 2013
†Corresponding author: Young-Joo Kim. Department of Rehabilitation Medicine, Sanggye-Paik Hospital, Seoul 139-707, Korea.
Tel: +82-2-950-1114, e-mail: [email protected]
○CThe Korean Society for Biomedical Laboratory Sciences. All rights reserved.
Original Article
활성도 감소와 교감신경의 활성화에 의하여 일어나며, 운 동직후에 심박수의 감소는 부교감신경계의 재활성화 작 용에 의한 것으로 알려져 있다 (Arai et al., 1989; Imai et al., 1994). 따라서 심박수 회복률의 감소는 부교감신경계 의 이상을 의미한다 (Yamamoto et al., 1991). 특히 회복기 1분의 심박수 변화량과 변화율은 부교감신경의 재활성도 를 잘 반영하는 것으로 알려져 있다 (Ju et al., 2004). 심근 경색증 환자에서 교감-부교감신경 균형은 교감신경 우위 로 이동하고, 부교감신경의 활성도는 감소한다 (Casolo et al., 1992). 심장질환 환자들에서는 이러한 부교감신경의 활성이 감소되어 있기 때문에 (Imai et al., 1994; Iellamo et al., 2000) 운동 중지 후 심박수의 감소 정도는 심장질환 의 예후와 관련이 있을 가능성이 있다 (Kim et al., 2004).
Cole 등 (1999)은 운동부하검사에서 최고 운동 시와 운동 종료 후 1분대 심박수의 차이를 회복기 심박수 (heart rate recovery, HRR)로 정의하였다. 운동 부족과 심폐 기능은 회복기 심박수와 밀접한 관계가 있다 (Goldsmith et al., 1997; Lauer, 2001). 심폐 기능 및 지구력이 우수한 사람일 수록 운동 중 심박수는 강도에 따라 서서히 증가하고 운 동 후에는 훈련되지 않은 사람에 비해 빠른 심박수 회복 을 보이는 것이 일반적인 현상이다 (Tuttle & Horvath, 1957). 규칙적인 운동은 자율 신경계의 활성도를 호전시 키며 특히 미주 신경계 활성도의 증가가 두드러지게 보 인다는 연구 보고가 많으나 이러한 결과의 기전에 대해 서는 아직 확실하지 않다 (Rosenwinkel et al., 2001; Billman, 2002).
심장재활 프로그램의 운동효과에 영향을 미치는 여러 가지 요소 중 논란이 있는 것이 베타차단제이다. 관상동 맥질환 환자에서 베타차단제 투여는 비 투여에 비해 운 동 능력 향상에 영향을 미치지 않는다는 보고와 함께 베 타차단제 투여가 운동 능력의 증가율을 감소시킨다는 보 고가 있었다 (Pollock et al., 1991; Wilmore et al., 1990). 또 다른 연구들에서는 심장질환 환자를 대상으로 한 연구에 서 베타차단제 투여군이 비 투여군 보다 운동 능력이 호 전되거나 동등한 최대 산소소모량의 증가를 관찰할 수 있다는 보고 (Fletcher et al., 1985; O'Connor et al., 1989)가 있었다 . 이 외에도 심근경색증 환자에서 낮은 심박변동과 운동 후 비정상적인 심박 감소는 사망률의 증가와 밀접 한 관련이 있다는 연구결과들 (Bigger et al., 1992; Cole et al., 1999; Cole et al., 2000)을 토대로 심근경색증 후 심박 변동 및 운동 후 심박수 회복에 영향을 주는 운동, 베타 차단제, 경피적 관상동맥 중재술 (percutaneous coronary
intervention, PCI) 등과 같은 여러 요소들에 대한 연구가 이루어져 왔다 (Bonnemeier et al., 2000; Larsen et al., 2004;
Malfatto et al., 1998).
위와 같이 지금까지의 연구들에서는 심장질환자들에 게 있어 베타차단제 약물 복용과 운동이 회복기 심박수 (HRR)의 개선과 운동 능력에 미치는 영향에 대해 상반된 연구결과를 보였으며, 그 기전 또한 명확하게 규명되지 않았다. 또한 운동과 베타차단제 약물 복용의 효과를 비 교한 연구가 국내외적으로 미미한 실정이다. 따라서 본 연구는 급성관상동맥증후군 환자에서 베타차단제 약물 복용과 유산소 운동 참여가 최대 운동 후 회복기 심박수 (HRR)와 운동 능력에 미치는 영향에 대해 알아보고자 한다 .
재료 및 방법
연구대상
2008년 9월부터 2010년 11월까지 급성관상동맥증후 군 (불안정 협심증, 급성심근경색증)으로 서울 소재 P 병원 심장내과에 입원하여 경피적 관상동맥 성형술 (percutaneous transluminal coronary angioplasty, PTCA) 및 약물치료를 받은 남자 환자를 대상으로 베타차단제 약물 복용과 유산소 운동을 함께 시행한 복합군, 베타차단제를 복용한 약물군, 6주 간의 유산소 운동을 시행한 운동군 그리고 통제군으로 총 4집단으로 구성하였다.
베타차단제 투여군의 약물은 Bisoprolol (Concor)을 복 용하는 환자로 제한하였으며, 6주 간의 사전 · 사후 검사 기간 동안 약물의 변화가 없었던 환자들을 대상으로 하 였다. 베타차단제 외에 심박수에 영향을 주지 않는 약물 들은 허용하였다.
이들 중 조절되지 않는 불안정 협심증, 심각한 부정맥, 좌심실 박출률 (ejection fraction)이 50% 미만인 경우, 운 동부하검사를 받기 어려운 만성 폐쇄성 폐질환과 근 · 골 격계 질환, 운동부하검사 도중 심혈관계 이상 반응으로 검사를 중단한 경우, 실험 기간 중 흡연이나 다른 요인으 로 약물을 중단한 경우, 중간에 약물처방이 환자의 상태 에 따라 바뀐 경우, 운동프로그램을 중도 포기한 경우는 연구대상에서 제외하였다. 본 연구는 인제대학교 생명윤 리위원회에 승인을 받았으며 환자의 정보와 실험에 대 한 동의를 얻어 연구되어졌다. 피험자의 신체적 특징은
<Table 1>과 같다.
측정 및 분석방법
신체계측 및 체성분 측정:
신장은 STDK-AD (Shintokyo Desshikizai Co., Japan)를 이용하였으며, 체중은 Autobody Weight (YK-150N, Korea) 기기를 이용하여 계측하였다.
체지방량 및 제지방량을 포함한 신체조성은 체성분 분석 기 (InBody 72 Biospace Co., Korea)를 이용하여 실험 개시 및 6주 후에 계측하였다.
운동부하검사 및 최대 운동 후 심박수 회복반응:
운동부하 검사는 4집단 모두에서 사전 검사와 6주 후 사후 검사를 시행하였다 . 베타차단제 약물을 복용하는 집단에서는 입 원 직후부터 약물을 복용하여 약 일주일간 약물 복용을 하고 있는 상태에서 사전 검사를 시행하였고, 유산소 운 동을 시행하는 집단에서는 운동 참여 전에 사전 검사를 시행한 후 사후 검사를 시행하였다. 유산소 운동은 운동 에 기초한 2단계 심장재활 프로그램으로 6주 간의 기간 동안 시행하였다. 검사 전 · 후로 Modified bruce protocol 을 이용하여 점진적 증상 제한 (symptom-limited) 운동부
하검사를 시행하였다.
검사는 12채널 실시간 운동부하검사용 심전도 검사기 Q4500 및 호흡가스 분석기 QMC (Quinton, U.S.A), 자동 혈압 및 맥박 측정기 (Model 412, U.S.A) 그리고 운동부하 검사용 트레드밀 (Medtrack ST 55, Quinton, U.S.A)을 사용 하였다.
운동부하검사를 시행하여 안정 시 및 최대 운동 시, 회 복기 시의 심박수, 혈압, 최대산소섭취량 (VO
2max), 총 운동 시간 (maximal exercise time, MT)을 측정하였다. 가 스 분석은 Quinton metabolic cart (QMCTM, U.S.A)를 이용 하여 mixing chamber mode로 15초 간격으로 측정하였다.
혈압 및 운동 자각도는 각 운동단계 2분에 측정하였으며, 운동 자각도는 6~20 Borg scale을 이용하였다.
운동 종료 후, 회복기에는 가볍게 걷기를 하면서 (1.3 mph) 약 5분간 회복 상태를 측정하였다. HRR은 선행연 구에서 제시한 방법으로 최대하 운동부하검사 시 도달한 최대 심박수에서 회복기 1분대 및 2분대 심박수를 뺀 값 으로 하였다 (Vivekananthan et al., 2003).
Table 1. Characteristics of research subjects
Factor BB-Ex (N=10) BB (N=10) Ex (N=10) Con (N=10) F P
Age (years) 54.90 ± 10.30 56.30 ± 10.68 55.70 ± 9.25 50.80 ± 9.31 .658 .583 Height (cm) 164.50 ± 6.36 166.50 ± 4.03 165.50 ± 6.83 167.00 ± 6.89 .325 .807 Weight (kg) 67.50 ± 6.77 70.75 ± 5.21 68.90 ± 8.38 76.10 ± 11.71 2.024 .128 BMI (kg/m2) 24.84 ± 2.83 25.52 ± 1.76 24.94 ± 2.07 27.16 ± 2.65 2.052 .124 RHR (beats) 68.50 ± 16.54 66.70 ± 13.74 76.70 ± 11.34 77.80 ± 8.05 1.937 .141 RSBP (mmHg) 118.80 ± 19.48 122.90 ± 15.04 115.60 ± 16.18 113.90 ± 15.17 .571 .638 RDBP (mmHg) 78.10 ± 10.37 81.10 ± 8.29 82.10 ± 10.54 78.40 ± 9.41 .417 .742 Diagnosis
UA 2 (20%) 5 (50%) 5 (50%) 1 (10%)
MI 8 (80%) 5 (50%) 5 (50%) 9 (90%)
Medications
Aspirin 10 (100%) 9 (90%) 9 (90%) 10 (100%)
Plavix 10 (100%) 9 (90%) 9 (90%) 8 (80%)
Statin 6 (60%) 8 (80%) 8 (80%) 8 (80%)
Vasodilator 9 (90%) 8 (80%) 6 (60%) 10 (100%)
ACEI 6 (60%) 5 (50%) 2 (20%) 4 (40%)
CCB 1 (10%) 1 (10%) 1 (10%) 3 (30%)
ATII 0 (0%) 1 (10%) 1 (10%) 0 (0%)
Diuretic 0 (0%) 2 (2%) 1 (1%) 0 (0%)
Values are mean ± SD. BB-Ex, beta-blocker and exercise complex group; BB, beta-blocker group; Ex, exercise group; Con, control group;
BMI, body mass index; RHR, rest heart rate; RSBP, rest systolic blood pressure; RDBP, rest diastolic blood pressure; UA, unstable angina;
MI, myocardial infarction; ACEI, angiotensin converting enzyme inhibitor; CCB, calcium channel blocker; ATII, angiotensin II type
운동프로그램
운동을 기초로 한 심장재활 2단계 프로그램에 참가하 는 환자들은 퇴원 후 1주 내에 심장재활 클리닉에서 감 시하 (supervised)에 운동을 시작하였다. 모든 운동 시간에 무선심전도를 부착하여 모니터로 심박수와 심장사건 (심 근허혈, 부정맥)을 감시하였다. 운동요법은 주 3회씩, 6주 동안 총 18회를 시행하였으며, 1회의 운동 시간은 준비 운동인 스트레칭 10분, 본 운동 24분, 정리 운동으로 가 볍게 3분간 걷고 난 후 스트레칭으로 마무리하였다. 본 운동은 트레드밀 (Quinton Medtrack SR 60, U.S.A)과 바이 크 (Quinton Corival 400, U.S.A)를 8분씩 교대로 시행하고 3분간 휴식기를 주면서 총 30분간 시행하였다. 운동 강도 는 운동프로그램을 시작하기 전에 시행한 운동부하검사 로 측정된 각 환자의 최대 심박수 및 안정시 심박수를 기준으로 예비 심박수 (heart rate reserve, HRR)를 계산하여 50%에서 85%까지 단계적으로 증가시켰다. 목표 심박수 는 Karvonen (1957)의 공식에 따라 산출하였다.
운동시작 첫째 주에는 운동부하검사에서 확인된 최대 목표 심박수의 50%, 둘째 주 60%, 셋째 주 70%, 넷째 주에서 여섯째 주 까지 85%로 운동 강도를 점진적으로 증가시켰다 .
자료처리방법
연구결과 얻어진 자료는 윈도우용 SPSS/PC+version 12.0 통계프로그램을 이용하여 기술 통계치 (mean ± SD)
를 산출하였다. 최대 심박수에서 1분대 심박수와 2분대 심박수의 전후 비교는 paired-t test로 검증하였으며 집단 간 회복기 1분 및 2분 심박수 (HRR1, HRR2), 최대산소 섭취량 (VO
2max) 그리고 총 운동 시간 (maximal exercise time, MT)의 전 · 후 차이 값의 차이 검증을 위해 일원변 량분석 (one-way ANOVA)을 실시하였으며 사후 검증을 위해 Bonferroni를 적용하였다. 통계적 유의 수준은 P<.05 로 설정하였다.
결 과
운동부하검사 후 회복기 심박수의 변화
집단 내 최대 심박수와 회복기 1분대 및 2분대 심박수 의 전 · 후 변화 값은 <Table 2>와 같이 최대 심박수는 BB-Ex에서 유의하게 증가하였다 (P=.033).
집단 내 회복기 1분 심박수 (HRR1)의 전 · 후 변화 값 은 BB-Ex에서 17.40 ± 5.58 bpm에서 26.10 ± 6.66 bpm 으로 유의하게 증가하였다 (P<.001). 집단 내 회복기 2분 심박수 (HRR2)의 전 · 후 변화 값은 BB-Ex에서 29.20 ± 8.84 bpm에서 39.50 ± 7.91 bpm으로 (P=.001), Ex에서 36.20 ± 10.11 bpm에서 43.30 ± 13.63 bpm으로 유의하게 증가하였다 (P=.016).
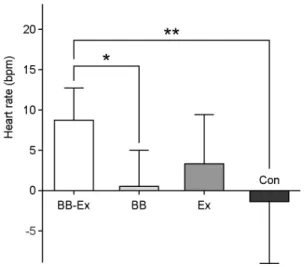
집단 간 최대 심박수에서 회복기 1분 심박수를 뺀 HRR1의 전 · 후 차이 값은 집단 간 유의한 차이가 있는 것으로 나타났다 (P=.002). 사후검증 결과 <Fig. 1>에서 보듯이 BB-Ex (8.70 ± 3.83 bpm)가 BB (0.40 ± 4.47 bpm)
Table 2. Change of maximal heart rate, 1 min and 2 min recovery heart rate in pre and post 6 weeksHR Pre (bpm) Post (bpm) t P
Max 134.70 ± 24.94 146.50 ± 21.88 -2.515 .033*
1 min 117.30 ± 21.10 120.40 ± 18.06 -0.706 .498
BB-Ex
2 min 105.50 ± 21.79 107.00 ± 18.48 -0.321 .755
Max 129.20 ± 17.70 134.90 ± 18.62 -1.339 .214
1 min 106.80 ± 17.19 112.10 ± 17.36 -1.256 .241
BB
2 min 96.00 ± 15.67 97.70 ± 11.55 -0.474 .647
Max 147.60 ± 18.75 153.60 ± 13.71 -1.843 .098
1 min 127.40 ± 15.95 130.20 ± 24 -0.642 .537
Ex
2 min 111.40 ± 10.38 110.30 ± 12.01 0.237 .818
Max 143.90 ± 21.70 146.20 ± 21.57 -0.453 .661
1 min 125.30 ± 21.54 128.90 ± 19.53 -0.757 .468
Con
2 min 110.00 ± 19.15 110.40 ± 17.52 -0.081 .937
Values are mean ± SD. BB-Ex, beta-blocker and exercise complex group; BB, beta-blocker group; Ex, exercise group; Con, control group;
HR, heart rate; Max, maximal; 1 min, 1 minute at recovery stage; 2 min, 2 minute at recovery stage; *P<.05
와 Con (-1.30 ± 7.48 bpm)에 비해 각각 유의하게 높은 것으로 나타났다 (P=.014와 P=.002). 집단 간 최대 심박 수에서 회복기 2분 심박수를 뺀 HRR2의 전 · 후 차이 값은 집단 간 차이가 없는 것으로 나타났다 (P=.057). 사 후검증 결과 <Fig. 2>에서 보듯이 BB-Ex (10.30 ± 6.36 bpm)가 Con (1.90 ± 6.70 bpm)보다 높은 경향만 보였다 (P=.065).
심폐 운동 능력의 변화
베타차단제 약물 복용과 유산소 운동 처치에 따른 집 단 내 최대산소섭취량 (VO
2max)은 BB-Ex 집단에서 운 동 전 · 후 30.46 ± 8.63에서 36.33 ± 8.10으로 유의하게 증가 (P=.006)하였지만 BB 집단에서는 6주 전 · 후 27.87
± 5.56에서 29.24 ± 6.73으로 유의한 차이가 없었다 (P=.232). Ex 집단에서는 운동 전 · 후 29.04 ± 4.93에서 34.31 ± 5.19로 유의한 증가 (P=.001)를 보였지만 Con 집
단에서는 6주 전 · 후 27.23 ± 7.58에서 27.35 ± 7.20으로 유의한 차이가 없었다 (P=.858). VO
2max의 6주 전 · 후 차이 값에 대한 집단 간 차이 검증결과 BB-Ex (5.87 ± 5.19 ml/kg/min)는 Con (0.12 ± 2.06 ml/kg/min)에 비해 (P=.007), Ex (5.27 ± 3.16 ml/kg/min)는 Con (0.12 ± 2.06 ml/kg/min)에 비해 (P=.018) 유의하게 높은 것으로 나타 났다 <Table 3>.
집단 내 총 운동 시간 (maximal exercise time, MT)에서 운동 전 · 후 BB-Ex 집단은 906.30 ± 158.57에서 1018.50
± 151.21로 유의하게 증가 (P=.002)하였으며, BB 집단에 서도 6주 전 · 후 805.70 ± 182.94에서 897.50 ± 160.16로 유의한 증가 (P=.001)를 보였다. 또한 Ex 집단에서도 운 동 전 · 후 870.00 ± 145.63에서 961.90 ± 107.29로 유의 한 증가 (P=.003)를 보였으나 Con 집단에서는 820.00 ± 127.52에서 823.50 ± 137.37으로 유의한 차이가 없었다 (P=.704).
총 운동 시간 (maximal exercise time, MT)의 전 · 후 차이
Table 3. Difference of VO2max and MT between pre and post test
BB-Ex BB Ex Con F P-value
VO2max (ml/kg/min) 5.87 ± 5.19 1.37 ± 3.38 5.27 ± 3.16 0.12 ± 2.06 6.142 BB-Ex** > Con Ex* > Con MT (sec) 112.20 ± 83.32 91.80 ± 60.92 91.90 ± 73.94 3.50 ± 28.14 5.568
BB-Ex** > Con BB* > Con Ex* > Con Values are mean ± SD. VO2max: maximal oxygen uptake. MT, maximal exercise time; BB-Ex, beta-blocker and exercise complex group;
BB, beta-blocker group; Ex, exercise group; Con, control group. **, P<.01; *, P<.05 Fig. 1. The difference in heart rate recovery at 1 minute after
exercise. BB-Ex, beta-blocker and exercise complex group; BB, beta-blocker group; Ex, exercise group; Con, control group. *, P<.05; **, P<.01
Fig. 2. The difference in heart rate recovery at 2 minute after exercise. BB-Ex, beta-blocker and exercise complex group; BB, beta-blocker group; Ex, exercise group; Con, control group
값에 대한 집단 간 차이 검증결과 BB-Ex (112.20 ± 83.32 sec)는 Con (3.50 ± 28.14 sec)에 비해 (P=.004), BB (91.80
± 60.92 sec)는 Con (3.50 ± 28.14 sec)에 비해 (P=.027) 그리고 Ex (91.90 ± 73.94 sec)는 Con (3.50 ± 28.14 sec)에 비해 (P=.026) 유의하게 높은 것으로 나타났다 <Table 3>.
고 찰
본 연구는 심장재활에 참여한 급성관상동맥증후군 환 자를 대상으로 베타차단제 복용과 유산소 운동이 회복기 심박수에 미치는 영향에 대해 연구하였다. 일반적으로 운 동부하가 증가되면 카테콜라민의 증가와 함께 교감신경 의 항진으로 심박수와 수축기 혈압이 증가한다. 최대 심 박수에서 심부전 환자는 정상인과 비교했을 때 20% 정 도 감소되어 있지만, 26개의 연구들에서 심부전 환자들의 운동 트레이닝 효과를 비교한 결과 운동 시 최대 심박수 가 증가하거나 변화가 없었다고 하였다 (Keteyian et al., 1997). 또한 Rainer 등 (2004)은 PCI 환자들을 대상으로 12개월 동안 운동 트레이닝을 한 집단에서 최대 심박 수가 유의하게 증가하였고 운동을 하지 않은 집단에서 는 변화가 없다고 하였다. 본 연구에서는 최대 심박수 (MHR)는 복합군에서만 유의하게 증가하였으며 운동군 에서는 유의하지는 않았지만 증가하는 경향성 (P=.098) 을 보인 결과가 선행연구들과 부분적으로 일치하였다. 이 는 트레이닝을 통한 운동 내성 증가로 전보다 더 높은 강도를 소화해 내기 위해 심박출량이 증가해야 하며, 심 박출량의 증가를 위해 심박수의 증가가 동반되기 때문인 것으로 사료된다.
운동 후 지연된 회복기 심박수 (HRR)는 자율 신경계 기능의 평가를 위한 요인으로 간단하게 측정할 수 있으 며, 심장재활 2단계 완료 후 심장재활 효과를 보여주는 결과 방법으로써 실용성이 증명되었다 (Tiukinhoy et al., 2003). 또한 Lipinski 등 (2004)은 HRR 1, 2분의 심박수 감 소율은 심혈관계 사망률 예측의 좋은 지표이지만 3분 이 후 HRR의 감소율은 심혈관계 사망률을 예측할 수 없다 고 하였다. 심부전 환자들에게 있어 운동 트레이닝은 운 동 시간 증가나 최대산소섭취량의 개선뿐만 아니라 자율 신경계 기능에도 긍정적인 변화를 준다 (Jett et al., 1991;
Kiilavuori et al., 1995; Keteyian et al., 1996; Giannuzzi et al., 1993). 심장재활에 참여하는 환자들은 심장사건과 관상동 맥의 재협착을 막기 위해 여러 가지 약물을 복용하는데, 그 중 베타차단제는 안정 시와 운동 시의 심박수와 혈압
그리고 운동 시 부정맥을 감소시켜주며 협심증 환자에 있어 운동 능력을 증가 시켜준다 (ACSM, 2006). 특히 선 택적 베타 1 차단제는 주로 심장에 작용하여 심장의 지 나친 수축을 억제하고 심박수 증가를 차단하는 것으로 알려져 있다 (Metra et al., 2001; Talbert, 2004). 또한 임상에 서 사용하는 베타차단제는 운동의 효과로 나타나는 심장 의 긍정적인 반응과 비슷하게 관상동맥질환으로 증가된 교감신경 활성을 감소시키고 감소된 부교감신경 활성도 를 증가시킴으로써 심박수 회복을 정상화시킨다 (Kim et al., 2006). 본 연구에서 복합군이 HRR1, 2 모두에서 가장 유의한 개선을 보였는데 이것은 베타차단제 약물과 유산 소 운동이 복합적으로 작용하여 HRR 개선에 영향을 준 것이라 사료된다. 또한 HRR2에서 운동군이 복합군 다음 으로 개선을 보였으며, HRR1의 전 · 후 차이 값을 집단 간 비교한 결과 운동군에서만 복합군과 유의한 차이를 나타내지 않았는데, 이러한 결과들은 복합군 다음으로 운 동군이 회복기 심박수의 개선을 보인 것이라 볼 수 있다.
이렇듯 운동군이 약물군보다 HRR의 개선을 보인 것은 약물군은 입원과 함께 일주일 정도 베타차단제를 복용하 고 있는 상태로 사전 검사가 이루어졌으며 6주 후 사후 검사에서도 베타차단제 복용 중에 검사가 이루어졌다. 그 러나 운동군은 유산소 운동 참여 전에 사전 검사가 이루 어졌으며 6주 간의 유산소 운동 참여 후 사후 검사가 이 루어졌기 때문에 약물군보다 운동군에서 HRR의 개선을 보인 것이라 사료된다.
운동 트레이닝은 심장병 환자들의 최대산소섭취량과
운동 능력을 향상시켜 준다 (Jette et al., 1991; Giannuzzi et
al., 1993). 선행연구들에 의하면 베타차단제 투여가 운동
지속시간은 증가시키더라도 최대산소섭취량 (VO
2max)은
저하시킨다고 하였으며 (Metra et al., 2001; Provencher et
al., 2006; Witte et al., 2005), 다른 연구에서는 베타차단제
가 운동 자극에 대한 혈류역학적 반응을 감소시키며 운동
능력의 감소는 보이지 않았다고 하였다 (Lund-Johansen,
1987). 또한 Richter 등 (1984)과 Fink 등 (1986)은 장기간
의 베타차단제 투여 후 심초음파에서 좌심실 기능의 변
화는 볼 수 있었으나 운동부하검사에서 산소섭취량에는
어떠한 개선을 보이지 않았으며, 이러한 결과는 혈류 역
학적 변화가 개선되어도 운동 능력의 개선에는 영향을
미치지 않았기 때문이라고 하였다. 본 연구에서는 최대산
소섭취량 (VO
2max)이 복합군과 운동군에서만 유의한 증
가를 보였으며, 총 운동 시간 (MT)은 통제군을 제외한
세 집단에서 증가를 보여 선행연구들과 부분적으로 일치
하였다. 베타차단제를 복용했던 약물군에서 최대산소섭 취량의 증가는 미비하지만 총 운동 시간은 유의하게 증 가하는 결과가 나타난 것은 운동 동안 힘든 자각도의 개 선과 관련이 있을 것이다 (Klaus et al., 2005). 또한 약물 군에서 총 운동 시간 (MT)이 사전 검사에서 보다 사후 검사에서 유의한 증가를 보였는데, 이러한 결과는 사전 검사 전 일주일 간의 약물 복용보다 6주 간의 약물 복용 이 충분한 약물 적응 효용성을 보이며 이로 인해 운동내 성을 증가시킨 것이라 생각된다. 즉, 베타차단제가 교감 신경을 차단하여 심박수와 혈압을 강하시킴에 따른 결 과로서 심근부담은 감소시킬지라도 운동수행력 측면에 서는 부정적 효과를 유도한 것이라 생각된다 (Kim et al., 2007).
이상의 결과로 미루어 보았을 때, 급성관상동맥증후군 환자들에게 베타차단제 약물 복용과 유산소 운동이 HRR 과 운동 능력의 개선에 주는 영향은 베타차단제와 유산 소 운동이 상호적으로 작용하였을 때 가장 긍정적인 것 으로 사료된다. 또한 약물군에서 HRR과 최대산소섭취량 의 개선을 보이지 못한 것은 심장재활 프로그램에서 회 복과 생존률을 높여주는 운동이 무엇보다 강조되어야 하 는 결과라고 생각되어진다. 그러나 본 연구는 표본수가 적고 환자의 검사 시간을 오전으로만 통일하였지만 시간 의 차이가 있을 수 있다. 약물 복용은 심장내과 전문의의 처방에 의존함으로써 집단 간에 발생한 내재적 편견이 있을 수 있다. 이러한 제한점들을 고려하여 더욱 많은 연 구들이 이루어져야 할 것이다.
REFERENCES
ACSM's guidelines for exercise testing and prescription-seven edition. 2006. seven edition. American College of Sports Medicine. USA.
Arai Y, Saul JP, Albrecht P, Hartley LH, Lilly LS, Cohen RJ, Colucci WS. Modulation of cardiac autonomic activity during and immediately after exercise. Am J Physiol. 1989. 256: 132 -141.
Bigger JT Jr, Fleiss JL, Steinman RC, Rolnitzky LM, Kleiger RE, Rottman JN. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation.
1992. 85: 164-171.
Billman G. Aerobic exercise conditioning: a nonpharmacological antiarrhythmic intervention. J Apple Physiol. 2002. 92: 446 -454.
Black & Matassarin-Jacobs, E. Medical-Surgical Nursing. 1997.
(5th ed.). Philadelphia, Saunders Co.
Blair SN, Kohl HW 3rd., Paffenbarger RS Jr, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA. 1989.
3; 262: 2395-2401.
Bonnemeier H, Hartmann F, Wiegand UK, Irmer C, Kurz T, Tolq R, Katus HA, Richardt G. Heart rate variability in patients with acute myocardial infarction undergoing primary coronary angioplasty. Am Cardiol J. 2000. 85: 815-820.
Casolo GC, Stroder P, Signorini C, Calzolari F, Zucchini M, Balli E, Sulla A, Lazzerini S. Heart rate variability during the acute phase of myocardial infarction. Circulation. 1992. 85: 2073 -2079.
Cole CR, Blackstone EH, Pashkow FJ, Snader CE, Lauer MS.
Heart rate recovery immediately after exercise as a predictor of mortality. N Eng J Med. 1999. 341: 1351-1357.
Fink LI, Wilson JR, Ferraro N. Exercise ventilation and pulmonary artery wedge pressure in chronic stable congestive geart failure.
Am J Cardiol. 1986. 57: 249-253.
Fletcher GF. Exercise training during chronic beta blockade in cardiovascular disease. Am Cardiol J. 1985. 55: 110-113 Giannuzzi P, Tavazzi L, Temporelli PL, Corrà U, Imparato A,
Gattone M, Giordano A, Sala L, Schweiger C, Malinverni C.
Long-term physical training and left ventricular remodeling after anterior myocardial infarction: results of the Exercise in Anterior Myocardial Infarction (EAMI) trial. EAMI Study Group. J Am Coll Cardiol. 1993. 22: 1821-1829.
Goldsmith RL, Bigger JT, Bloomfield DM. Physical fitness as a determinant of vagal modulation. Med Sci Sports Exerc. 1997.
29: 812-817.
Kim C, Bang IG, Kim YJ. Effect of beta blocker on heart rate variability at rest and heart rate recovery after maximum exercise for coronary artery disease. KJSS. 2006. 17: 23-32.
Kim HS, Lee JH, Kwon YS, Lee HS, Yang DH, Park HS, Jo YK, Chae SC, Jun JE, Park WH. Changes in Heart Rate during and after Exercise Treadmill Test as Prognostic Factor in Cardiovascular Disease. KCJ. 2004. 34: 170-177.
Kim YJ, Shin YO, Kim SH, Oh JK. Effect of beta blocker and ACE inhibitor treatment after percutaneous coronary inter- vention on blood pressure during exercise stress test. JKSR.
2007. 18: 61-72.
Iellamo F, Legramante JM, Massaro M, Raimondi G, Galante A.
Effects of a residential exercise training on baroreflex sensitivity and heart rate variability in patients with coronary
artery disease: a randomized, controlled study. Circulation.
2000. 102: 2588-2592.
Imai K, Sato H, Hori M, Kusuoka H, Ozaki H, Yokoyama H, Takeda H, Inoue M, Kamada T. Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol. 1994.
24: 1529-1535.
Jetté M, Heller R, Landry F, Blümchen G. Randomized 4-week exercise program in patients with impaired left ventricular function. Circulation. 1991. 84: 1561-1567.
Ju DU, Kang HJ, Kim SW, No TM, Son HS, Kang BJ, Kim SR, Lee BR, Jung BC, Lee JJ. The difference of heart rate recovery in ischemic heart dissease comparing to normal. Korean J Intern Med. 2004. 66: 586-593.
Keteyian SJ, Levine AB, Brawner CA, Kataoka T, Rogers FJ, Schairer JR, Stein PD, Levine TB, Goldstein S. Exercise training in patients with heart failure. A randomized, controlled trial. Ann Intern Med. 1996. 124: 1051-1057.
Klaus KA, Witte Simon Thackray, Nikolay P, Nikitin John GF, Cleland Andrew L, Clark. The effects of long-term b-blockade on the ventilatory responses to exercise in chronic heart failure. The European Journal of Heart Failure 2005. 7: 612 -617.
Kiilavuori K, Toivonen L, Naveri H, Leinonen H. Beversal of autonomic derangements by physical training in chronic geart failure assessed by geart rate variability. Eur Geart J. 1995.
16: 490-495.
Larsen AI, Gjesdal K, Hall C, Aukrust P, Aarsland T, Dickstein K.
Effect of exercise training in patients with heart failure: a pilot study on autonomic balance assessed by heart rate variability. Eur J Cardiovasc Prev Rehabi. 2004. 11: 162-167.
Lauer MS. Heart rate response in stress testing: clinical implication.
ACC Curr J Rec. 2001. 10: 16-19.
Lavie CJ, Milani RV, Littman AB. Benefits of cardiac rehabilitation and exercise training in secondary coronary prevention in the elderly. J Am Coll Cardiol. 1993. 22: 678-683.
Lipinski MJ, Vetrovec GW, Froelicher VF. Importance of the first two minutes of heart rate recovery after exercise treadmill testing in predicting mortality and the presence of coronary artery disease in men. Am J Cardiol. 2004. 15; 93: 445-449.
Lund-Johansen P. Exercise and antihypertensive therapy. Am J Cardiol. 1987. 23; 59: 98-107.
Malfatto G, Facchini M, Sala L, Branzi G, Bragato R, Leonetti G.
Effects of cardiac rehabilitation and beta-blocker therapy on heart rate variability after first acute myocardial infarction.
Am J Cardiol. 1998. 8: 834-840.
Metra M, Nodari S, Dei Cas L. Beta-blockade in heart failure:
selective versus nonselective agents. Am J Cardiovasc Drugs.
2001. 1: 3-14.
O'Connor GT, Buring JE, Yusuf S, Goldhaber SZ, Olmstead EM, Paffenbarger RS Jr, Hennekens CH. An overview of ran- domized trials of rehabilitation with exercise after myocardial infarction. Circulation. 1989. 80: 234-244.
Provencher S, Herve P, Jais X, Lebrec D, Humbert M, Simonneau G, Sitbon O. Deleterious effects of beta-blockers on exercise capacity and hemodynamics in patients with portopulmonary hypertension. Gastroenterology 2006. 130: 120-126.
Pollock ML, Lowenthal DT, Foster C, Pels AE, Rod J, Stoiber J, Schmidt DH. Acute and chronic responses to exercise in patients treated with beta blockers. J Cardiopul Rehabil. 1991.
11: 132-144.
Rainer Hambrecht, Claudia Walther, Sven Mobius-Winkler, Stephan Gielen, Axel Linke, Katrin Conrandi, Sandra Erbs, Regine Kluge, Kai Kendziorra, Osama Sabri, Peter Sick, Gerhard Schuler. Percutaneous coronary angioplasty compared with exercise training in patients with stable coronary artery disease. Circulation. 2004. 109: 1371-1378.
Richter EA, Sonne B, Mikines KJ, Ploug T, Galbo H. Muscle and liver glycogen, protein, and triglyceride in the rat. Effect of exercise and of the sympatho-adrenal system. Eur J Appl Physiol Occup Physiol. 1984. 52: 346-350.
Rosenwinkel ET, Bloomfield DM, Arwady MA, Goldsmigh RL.
Exercise and autonomic function in health and cardiovascular disease. Cardiol Clin. 2001. 19: 369-387.
Shah PK. New insighis in the pathogenesis and prevention of acute coronary dyndromes. The American Journal of Cardiology 1997. 79: 17-23.
Talbert RL. Pharmacokinetics and pharmacodynamics of beta blockers in heart failure. Heart Fail Rev. 2004. 9: 131-137.
Thompson PD, Buchner D, Pina IL, Balady GJ, Williams MA, Wenger N. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: A statement from the council on clinical cardiology (subcom- mittee on exercise, rehabilitation, and prevention) and the council on nutrition, physical activity, and metabolism.
Circulation. 2003. 107: 3109-3116.
Tiukinhoy S, Beohar N, Hsie M. Improvement in Heart Rate Recovery After Cardiac Rehabilitation. Journal of Cardio- pulmonary Rehabilitation 2003. 23: 84-87.
Tuttle N, Horvath SM. Comparison of effect of static and dynamic
work on blood pressure and heart rate. J Appl Physiol. 1957.
10: 294-296.
Vivekananthan DP, Blackstone EH, Pothier CE, Lauer MS. Heart rate recovery after exercise is a predictor of mortality, independent of the angiographic severity of coronary disease.
J Am Coll Cardiol. 2003. 3; 42: 831-838.
Wilmore JH, Wambsgans KC, Kunkel RC, Baron SB, Ewy GY, Goolsby JP, Morris DL, Robinson WA, Strauss M, Kalis JK.
Effect of beta-adrenergic blockade on achievement of the trained state in post-MI patients: non-selective vs beta-selective blockers. J Cardiopul Rehabil. 1990. 10: 50-57.
Witte KK, Thackray S, Nikitin NP, Cleland JG, Clark AL. The effects of long-term beta-blockade on the ventilatory responses to exercise in chronic heart failure. Eur J Heart Fail. 2005. 7:
612-627.
Yamamoto Y, Hughson RL, Peterson JC. Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J Appl Physiol. 1991. 71: 1136-1142.
Yeo NH, Kim SS. The effect of aerobic exercise training on blood pressure and electrocardiogram (ECG) in chronic heart failure.
Exercise Science. 2001. 10: 31-41.