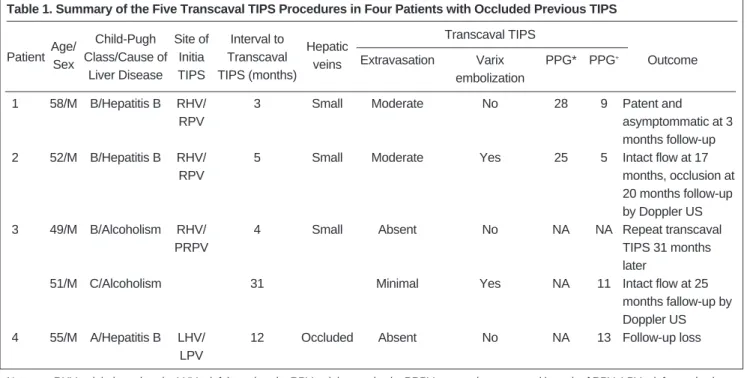
I Transcaval TIPS in Patients with FailedRevision of Occluded Previous TIPS
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
According to the result of this study, to do effective nursing that improve health promoting behaviors of early-stage lung cancer patients, nurses should
The aim of this study was to provide a optimal drug therapy which secures effectiveness and safeness in elderly patients by analyzing polypharmacy and the
Abstract: This study was aimed to investigate the adhesion control standards of pain relieving patch (PRP) drugs and to survey it′s adverse effects on the skin of patients
Empirical results of this study indicate that the incremental explanatory power of earning is greater than that of cash flow in the mature stage of the
In this study, it is shows that the stream of CO 2 is more effective in the reduction of unreacted TEGDMA and the increase of surface microhardness than that of N 2
Objective: The purpose of this study was to analyze recent trend in incidence of basal cell carcinoma and squamous cell carcinoma in patients from the Gwangju City
The purpose of this study was to identify the frequency and related factors of advanced airway management for patients with cardiac arrest by the
Therefore, this paper is to recognize the common mistakes English learners make while using English articles and to provide helpful tips for those who teach
