접수일: 2009년 8월 20일, 게재승인일: 2009년 9월 7일 책임저자: 박기영, 대구시 남구 대명 4동 3056-6번지
705-718, 대구가톨릭대학교 의과대학 재활의학교실
Tel: 053-650-4492, Fax: 053-623-7507 E-mail: [email protected]
엉덩이 질환의 초음파 소견
대구가톨릭대학교 의과대학 재활의학교실
박 기 영
Ultrasonographic Findings of the Hip Disorders
Gi-Young Park, M.D., Ph.D.
Department of Rehabilitation Medicine, School of Medicine, Catholic University of Daegu, Daegu, Korea
The advent of high-resolution ultrasonographic technology has enhanced the value of ultrasonography as a diagnostic imaging modality for the assessment of various hip joint and soft tissue pathologies. The purpose of this paper is to illustrate the ultrasonographic appearance of various dis- orders of the hip. The role of ultrasonography in the evalua- tion of the pediatric hip disorders is well recognized.
However, its usefulness is less well recognized and often underused in adults. Indications include assessment of joint effusion, muscle and tendon abnormalities, and bursitis. In addition, ultrasonography is a valuable tool in assisting with joint aspiration and injections. In the hip disorders, the main value of ultrasonography is the ability to differentiate be- tween intra-articular and extra-articular pathology. This ultra- sonographic information can be provided quickly, at a low cost, and applies to the adult and pediatric patients.
(Clinical Pain 2009;8:96-102)
Key Words: Ultrasonography, Hip, Intra-articular pathology, Ex- tra-articular pathology
서 론
소아 엉덩이 관절 삼출과 유아 엉덩이 관절 불안정을 평 가하는 데 있어 초음파의 역할은 잘 인정되고 있다.1) 그러 나 성인에서는 초음파의 유용성이 잘 인정되지 않고, 자주 적게 사용되고 있다. 엉덩이 초음파의 적응증은 관절 삼출, 근육과 힘줄 이상 및 윤활낭염(bursitis)이다.2) 또한 초음파 는 관절 흡인과 주사에 있어 유용한 도구이다. 그러나 큰
체구는 초음파 검사를 방해할 수 있다. 초음파의 주요 가치 는 엉덩이와 연관된 통증과 부기를 가진 환자에서 관절 내, 외 병변을 구별하는 능력이다. 그러나 초음파는 앞위쪽 절 구테두리(acetabular labrum)의 제한된 부위만 볼 수 있어 자기공명관절 조영술이 테두리 병변을 평가하는데 일차선 택 영상검사이다. 또한 자기공명영상은 무혈관괴사 (avascular necrosis), 골수 병변, 관절 연골 및 관절 형태를 평가하는데 일차선택 영상검사이다.
본 론 1. 관절 내 병변
성인에서 엉덩이 관절 삼출 존재 시 외상, 수술 및 출혈 성 질병과 관련된 출혈, 패혈성 관절염, 염증성과 비염증성 관절염, 무혈성 괴사 및 색소성 융모 결절성 윤활막염(pig- mented villonodular synovitis)과 윤활 연골종증(synovial chondromatosis)과 같은 종양 등이 감별진단 되어야 한다.
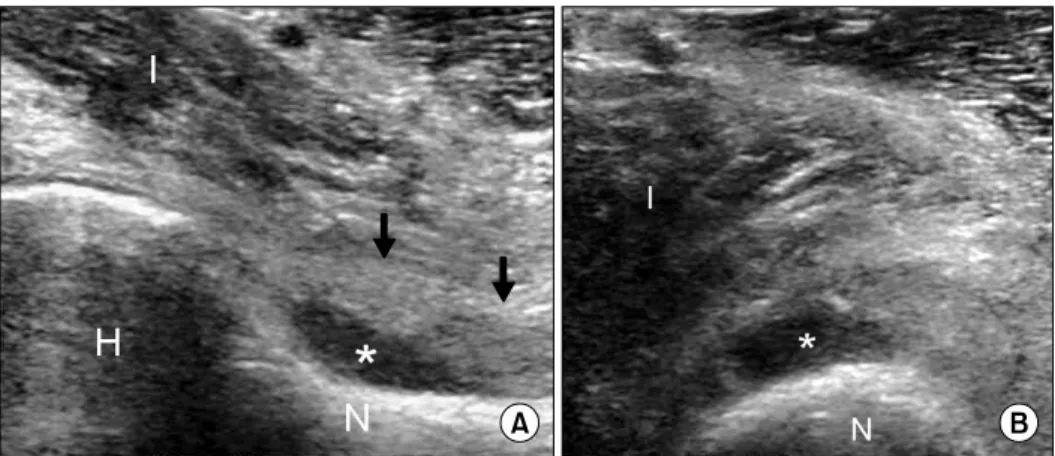
관절 삼출은 엉덩이 관절을 벌림과 바깥 회전한 상태에서 넙다리뼈 목(femoral neck)을 따라 가장 잘 관찰된다(Fig.
1).3) 이와 같은 자세는 넓다리뼈 목으로부터 관절막과 엉덩 넙다리(iliofemoral) 인대를 분리시킨다.4) 관절 액은 초음파 에서 무에코, 저에코 및 복합에코로 나타날 수 있고, 1∼2 ml의 적은 양의 관절액도 초음파에서 탐지될 수 있다. 증상 과 무증상 엉덩이에서 2 ml 이상의 관절액 차이는 의미있 는 소견이다.5-7) 관절액의 크기와 특징으로 감염성과 비감 염성 삼출을 구별할 수 없어 관절 흡인이 필요하다. 초음파 의 최대 가치는 관절액을 탐지하고, 흡인을 실시간 초음파 유도 하에서 쉽게 하는 데 있다. 이를 통해 무효천자(dry tap)의 발생과 다른 주위 액 수집으로부터 관절의 오염을 피할 수 있다. 또한 활막 증식 장애도 초음파 평가와 초음파 유도하 생검으로 분석할 수 있다.
관절내 유리체(loose bodies)는 관절 액이 존재할 때 가 장 잘 탐지되며, 관절 액에 자유롭게 떠다니는 분리된 고에 코의 물체를 관찰할 수 있다.8) 유리체는 뼈연골 골절, os- techondritis dissecans, 골관절염과 연관된 뼈곁돌기(osteo- phyte) 및 윤활연골종증 등에 의해 발생될 수 있다. 초음파 는 단순방사선촬영과 달리 석회성과 비석회성 관절 내 물 체를 볼 수 있다.
박기영: 엉덩이 질환의 초음파 소견
Fig. 1. Hip joint effusion. Longitu- dinal (A) and transverse (B) ultra- sonographic images of the anterior hip demonstrate the hyperechoic joint capsule (arrows), displaced from the echogenic interface of the femoral neck (N) by a joint effu- sion (asterisk). H (femoral head), I (iliopsoas).
Fig. 2. Tear in iliopsoas muscle. Longitudinal ultrasonographic image of the iliopsoas muscle demonstrates a torn muscle fibers (open arrowheads) surrounded by hematoma (arrows). A (acetabulum), H (femoral head), iliofemoral ligament (open ar- rowheads).
2. 관절 외 병변
초음파는 윤활낭염, 특히 엉덩허리근(iliopsoas)과 큰돌 기(greater trochanter) 윤활낭을 진단하는데 유용하다. 팽창 된 엉덩허리근 윤활낭은 임상적으로 샅고랑부위(groin) 덩 어리로 나타날 수 있어 샅굴 탈장(inguinal hernia), 넙다리 거짓동맥 류(femoral artery aneurysm), 혈종, lymphocele, 림프절병증(lymphaenopathy), 농양 및 종양 등과 감별진단 이 필요하다.9) 엉덩허리근 윤활낭은 초음파에서 찌부러졌 을 때 보이지 않을 수 있으나 팽창되었을 때 액을 먼쪽 엉 덩이허리근 힘줄 주위에서 액을 확인할 수 있다. 엉덩허리 근 윤활낭은 활액막 비후, 사이막형성(septation) 및 조직파 편(debris)의 복잡한 소견을 나타낼 수 있다.10) 큰돌기 윤활 낭은 큰돌기 위에 팽창된 액 공간으로 확인될 수 있다. 궁둥 뼈볼기(ischiogluteal) 윤활낭염은 덩어리와 연관된 궁둥이 통증의 원인일 수 있다.11) 윤활낭 진단에 있어 초음파의 장 점은 탐침자로 압박했을 때 윤활낭의 모양 변화, 활액막 비 후와 충혈(hyperemia)의 평가, 환자 증상과의 연관성 및 흡 인과 주사에 용이성이다. 포착하기 힘든 윤활낭은 탐침자 로 너무 많은 압력을 가했을 때 초음파에서 쉽게 발견되지 않을 수 있다.
엉덩이의 운동과 연관된 손상은 넙다리 곧은 근(rectus femoris muscle)과 뒤넙다리 근(hamstring muscle)에서 가 장 자주 발생한다. 초음파는 특히 급성기에 근육 파열을 확 진하는 데 정확한 검사 방법으로 이완된 근육 내 다양한 정도의 저에코 혹은 불연속성을 나타낸다(Fig. 2). 급성 파 열은 근육의 정상 날개(pennate) 형태를 왜곡시킨다. 부분 파열은 국소적 근섬유의 불연속성이나 근육 다발의 불규칙 한 불길 형태로 나타나며, 출혈이 동반된 파열 부위는 더욱 고에코로 보일 수 있다(Fig. 2).12) 동적 검사는 근육의 굽힘 (수축)과 폄(이완) 동작 동안 시행하며, 파열된 근육과 혈종 을 구별하는 데 도움을 준다. 큰 근육 파열인 경우 액체화된
혈종에 둘러싸인 자유로이 움직이는 파열된 근육 섬유에 부드럽게 탐침자 압력을 가했을 때 종 추(bell clapper) 징후 를 나타낸다.13) 만성적으로 치유된 파열은 비틀어진 근육 의 불균질 부위로 나타난다. 섬유화는 근육 내 고에코 변화 로 나타나며, 뒤소리그림자(posterior acoustic shadowing) 지역, 석회화 및 골화가 동반될 수 있다.12) 큰 근육 파열 혹 은 섬유화 결과로 생긴 부위는 거짓종양(pseudotumor)으로 나타날 수 있고 넓적다리에서 가장 흔한 거짓종양은 넙다 리곧은근의 파열로 발생한다.14) 종괴 혹은 만질 수 있는 덩 이의 크기가 시간 경과에 따라 점진적으로 감소되었다는 환자의 과거력이 중요하다. 진짜 종양인 경우 병변은 대개 시간경과에 따라 커지게 된다. 또한 덩이는 종종 안정 때
Fig. 3. Necrotizing fascitis. Longi- tudinal (A) and transverse (B) ul- trasonographic images over the greater trochanter (GT) demon- strate accumulation of fluid along facial planes (arrows). Ultrasound color-scale elastography (C) dem- onstrates the heterogenicity of fluid nature from purple for tissue with the greatest strain (softest tissue) to red for those with no strain (hardest tissue, arrow head), be- tween facial planes (arrows).
미묘하거나 소실되나 근육을 굽힐 때 딱딱해지고 두드러진 다.
힘줄 손상은 부분층 혹은 전층 파열을 포함하며, 손상 정 도에 따라 초음파에서 힘줄의 다양한 내부 저에코 혹은 불 연속성을 나타낸다. 이와 같은 저에코 부위는 힘줄-뼈 삽입 부, 근위부 힘줄 및 근육-힘줄 접합부에서 발생할 수 있다.
샅고랑부위 통증을 야기하는 모음근(adductor) 힘줄병증은 광범위한 부기와 에코 소실을 나타내며, 반대쪽과 주의 깊 게 비교하면 진단할 수 있다. 만성 석회화 힘줄병증은 초음 파에서 석회화 부위의 크기에 따라 뒤소리그림자를 동반하 거나 동반하지 않으면서 힘줄 내 국소적 고에코 부위를 나 타낸다.15) 엉덩이의 석회화 힘줄병증은 큰 돌기위의 큰 볼 기 근(gluteus maximus muscle), 아래 앞 엉덩뼈 가시(ante- rior inferior iliac spine)의 넙다리 곧은 근 기원부위 및 작은 돌기의 엉덩허리근 삽입부위에서 자주 발생한다. 다른 관 절 외 병변은 혈종, 고름집, 림프절병증 및 거짓동맥류 등이 있다.16,17)
퉁김소리 엉덩이 증후군(snapping hip synrome)은 환자
가 통증 유무와 상관없이 엉덩이 관절 운동 동안 퉁김소리 를 경험하는 것을 말한다.18) 초음파로 퉁김소리 엉덩이 증 후군을 검사 할 때 신중히 환자에게 그 운동을 재현하도록 하고, 실시간 동영상으로 저장하여야 한다. 이와 같은 장애 의 동적인 특성을 고려할 때 초음파는 퉁김소리를 재생할 수 있는 환자에서 증상의 원인을 밝히는 데 자기공명영상 보다 확실한 장점을 가지고 있다. 퉁김소리는 다양한 관절 내외 원인들에 의해 발생하기 때문에 임상적으로 원인을 밝히는 것은 어려울 수 있다.18,19) 관절 내 원인은 절구테두 리 파열, 뼈곁돌기, 윤활연골종증 및 유리체 등이 있다.2,19) 관절 외 원인은 환자의 증상 위치에 따라 좌우된다. 가쪽 퉁김소리는 엉덩정강 환(iliotibial band)이 큰 돌기 위로 미 끄러질 때 발생하며, 달리기 선수에서 자주 볼 수 있다.2) 반면에 안쪽 퉁김소리는 엉덩허리근 힘줄이 엉덩허리근볼 기 융기(iliopectineal eminence) 혹은 작은 돌기(lesser tro- chanter) 위에서 걸릴 때 발생하며, 발레 무용수에서 자주 볼 수 있다.19-21) 다른 원인으로 넙다리두갈래근(biceps femoris muscle)의 긴 갈래(long head)가 궁둥뼈 결절
박기영: 엉덩이 질환의 초음파 소견
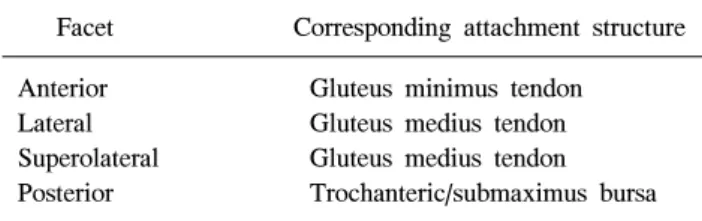
Table 1. Anatomical Landmarks on Greater Trochanter
Facet Corresponding attachment structure Anterior Gluteus minimus tendon
Lateral Gluteus medius tendon
Superolateral Gluteus medius tendon Posterior Trochanteric/submaximus bursa (ischial tuberosity)의 뒤쪽에서 퉁길 때 발생할 수 있다.2)
초음파는 엉덩이 관절성형술(arthroplasty) 후 통증이 있 는 환자에서 관절 내 삼출을 발견하거나, 관절 외 액 수집의 위치를 확인하거나, 초음파 유도하 천자를 시행하는 데 효 과적으로 사용되어 왔다.22) 인공삽입물(prosthesis)에 의해 발생하는 인공음영(artifact)은 컴퓨터 전산화 단층촬영과 자기공명영상 사용을 어렵게 한다. 초음파에서 관절 외 액 수집을 동반하면서 관절 내 삼출이 인공 삽입물과 뼈 경계 에서 3.2 mm 이상 측정될 때 감염에 대한 높은 특이성이 있다.23)
초음파는 소아에서 엉덩이의 발달 형성이상(dysplasia) 을 진단하는 데 널리 사용되고 있다. 초음파는 패혈 관절염 혹은 일시적 윤활막염과 연관된 액의 발견과 특성화, 윤활 비대를 확인하는 데 도움이 된다. 초음파는 관절 삼출 발견 에 민감한 검사이므로 관절 액이 발견되지 않았을 때 불필 요한 엉덩이 천자를 시행하지 않는다.24,25)
괴사성 근막염(necrotizing fascitis)은 자주 과거 외상과 연관되어 세균이 피하 조직, 근막 및 근육을 포함한 주위 연 조직을 침범하여 괴사를 일으키는 치명적인 중증 감염 질환이다. 비교적 드문 질환이지만, 병소가 급속도로 확산 되기 때문에 환자의 생명을 위협할 수 있어 조기 진단과 조기 치료만이 괴사성 근막염과 관련된 높은 사망률을 낮 출 수 있다. 대부분의 경우 환자는 당뇨, 면역약화 혹은 만 성적 중증 질환을 가지고 있다. 연조직 질환이 연조직염 (cellulitis)과 유사할 때 비록 초음파가 감염의 초기 단계에 서 진단에 도움이 되지 않을 수 있으나 근막 비후와 깊은 근막을 따라 축적된 혼탁 액의 범위를 확인하는 데 도움이 될 수 있다. 액의 양이 깊이 4 mm 초과될 때 괴사성 근막염 진단에 높은 민감도와 특이도를 보인다.26) 또한 초음파는 병이 진행된 경우 연 조직에서 가스 형성과 근막 면에서 방형성 고름집(loculated abscess)을 확인할 수 있으며, 초음 파 유도하 진단적 흡인을 시행할 수 있다(Fig. 3).27,28) 공격 적 죽은조직절제술(debridement)과 광범위항생제의 사용이 환자의 생명을 구하는 데 중요하다.
3. 큰 돌기 통증 증후군(greater trochanteric pain syndrome)
작은 돌기 근(gluteus minimus)과 중간 돌기 근(gluteus medius)은 바깥 엉덩 오목(external iliac fossa)에서 시작되 어 해당 힘줄들은 큰 돌기에 부착된다. 두 근육들은 엉덩이 주 벌림근으로 작용하며, 안쪽 회전, 굽힘 및 안정성에 도움 을 준다.29) 큰 돌기 바깥 표면의 4 면(앞쪽 면, 바깥쪽 면, 위바깥쪽 면 및 뒤쪽 면) 개념은 큰 돌기 통증 증후군 평가 를 위한 유용한 자기공명영상과 초음파의 해부학적 기준점 을 제공한다(Table 1).30,31) 작은 돌기와 중간 돌기 힘줄들은
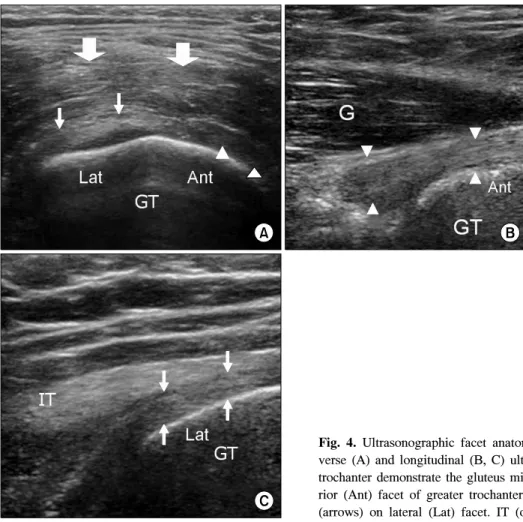
각각 앞쪽과 뒤쪽 큰 돌기 면에 부착된다(Fig. 4A). 작은 돌기 근은 거의 중간 돌기 근에 의해 덥여 있고, 작은 볼기 힘줄의 모양은 삼각형으로부터 불규칙한 L 형태까지 다양 하다(Fig. 4B). 중간 볼기 힘줄은 바깥 면에 넓게, 위쪽 바깥 쪽 면에 좁게 부착한다(Fig. 4C). 작은 돌기 밑 윤활낭 (subgluteus minimus bursa)은 작기 돌기 힘줄과 앞쪽 면 사 이에 위치하고, 중간 돌기 밑 윤활낭(subgluteus medius bursa)은 중간 돌기 힘줄의 바깥 면 삽입 부위 아래에 파묻 혀 있다. 돌기 윤활낭(trochanteric bursa)은 큰 돌기 근육 아 래에 파묻혀 있으면서 뒤쪽 면을 덮으며, 바깥쪽과 먼쪽으 로 확장되어 있다. 추가 윤활낭이 엉덩정강 환과 큰 돌기 사이에 존재할 수 있다.30)
작은 돌기와 중간 돌기 힘줄병증은 큰 돌기 통증 증후군 의 잘 알려진 원인으로 주로 바깥쪽 엉덩이의 무딘 통증, 국소적 압통 및 엉덩이 벌림의 약화를 나타낸다.32) 자기공 명영상은 바깥쪽 엉덩이 통증의 다른 원인들을 배제하거나 돌기 힘줄병증의 직접 증후(주위 연조직 부종, 힘줄 비후, 힘줄 내 신호 이상 및 힘줄 섬유의 국소적 불연속성 혹인 소실) 혹은 간접 증후(작은 돌기 혹은 중간 돌기 및 윤활낭 염, 큰 돌기 삽입부를 따라 부착부병증(enthesopathy) 및 지 방 위축)를 평가하는 데 유용하다.33) 또한 초음파도 중간과 작은 돌기 힘줄 삽입을 평가할 수 있다.
초음파는 힘줄을 정확히 확인하는데 도움을 주는 큰 돌 기 면의 해부를 잘 증명할 수 있다. 신체 다른 부위의 힘줄 과 마찬가지로 힘줄병증은 종종 힘줄 비후와 더불어 감소 혹은 불균질의 에코를 나타낸다(Fig. 5). 파열은 힘줄이 얇 아지거나 힘줄 내 부분 혹은 전층 무 에코 결손으로 나타난 다(Fig. 6A). 색 도플러에서 증가된 혈관분포정도는 힘줄병 증과 파열 진단에 도움이 되나 드문 소견이다(Fig. 6B). 벗 어진 면(bald facet)은 완전 파열과 일치되는 소견으로 힘줄 섬유의 소실을 의미한다. 근육 쇠약은 근육 부피의 감소와 지방 대체로 인해 고 에코로 나타날 수 있다. 겉질 뼈 불규 칙(cortical irregularity)은 돌기 삽입부 아래에서 발견될 수 있으므로 검사자는 위에 위치한 힘줄을 자세히 평가해야 한다. 윤활낭 액 수집과 비후는 쉽게 감지될 수 있다(Fig. 7).
석회화 볼기 힘줄병증은 자기공명영상보다 초음파에서 잘 보일 수 있으며, 초음파 유도하 흡인과 주사를 할 수 있다.33)
Fig. 4. Ultrasonographic facet anatomy of greater trochanter (GT). Trans- verse (A) and longitudinal (B, C) ultrasonographic images over the greater trochanter demonstrate the gluteus minimus insertion (arrow heads) on ante- rior (Ant) facet of greater trochanter and the gluteus medius (G) insertion (arrows) on lateral (Lat) facet. IT (open arrow, iliotibial tract).
Fig. 5. Gluteus medius tendinosis.
Longitudinal ultrasonographic im- age demonstrate abnormal thicken- ing of the right gluteus medius ten- don at the insertion of gluteus medius tendon on greater tro- chanter (GT) compared with left one.
박기영: 엉덩이 질환의 초음파 소견
Fig. 6. Gluteus medius tendon par- tial-thickness tear. Longitudinal (A) ultrasonographic image dem- onstrate focal partial-thickness de- fect (arrow) at the superficial fiber of gluteus medius tendon on great- er trochanter (GT). Power Doppler examination (B) demonstrate in- creased vascularity around the defect.
Fig. 7. Trochanteric bursiits. Longitudinal ultrasonographic im- age at the greater trochanter demonstrate small amount of fluid collection (arrows) on the greater trochanter (GT) of femur un- der iliotibial tract (IT).
결 론
초음파는 어린이의 엉덩이 관절 삼출과 유아의 엉덩이 불안정을 평가하는 데 일차선택 영상검사이나 성인에서 초 음파의 역할은 낮게 정의되어 임상적으로 적게 사용되고 있다. 성인 엉덩이와 주위 연조직의 초음파는 근육과 힘줄 파열, 힘줄윤활염, 윤활낭염, 관절 삼출, 연조직 감염 및 엉 덩이 수술 후 액 수집 등을 평가하는데 도움이 되며, 감염이 의심될 때 흡인을 쉽게 한다. 동적 초음파는 자기공명영상 에 비해 명백한 장점으로 퉁김소리 엉덩이의 원인들을 동 적으로 진단할 수 있다. 엉덩이 초음파의 가장 큰 제한은
환자의 체형으로 검사 때 조직을 적절히 통과할 수 있는 낮은 주파수를 사용해야 한다. 초음파 엉덩이 질환에 대해 저렴한 비용으로, 빠른 정보를 제공하므로 성인과 소아에 모두 적용될 수 있다.
참 고 문 헌
1. Harcke HT, Grissom LE. Pediatric hip sonography.
Diagno_sis and differential diagnosis. Radiol Clin North Am 1999;37:787-96.
2. Cho KH, Park BH, Yeon KM. Ultrasound of the adult hip.
Semin Ultrasound CT MR 2000;21:214-30.
3. Chan YL, Cheng JC, Metreweli C. Sonographic evaluation of hip effusion in children. Improved visualization with the hip in extension and abduction. Acta Radiol 1997;38:867-9.
4. Berman L, Fink AM, Wilson D, McNally E. Technical note:
identifying and aspirating hip effusions. Br J Radiol 1995;
68:306-10.
5. Zeiger MM, Dorr U, Schulz RD. Ultrasonography of hip joint effusions. Skeletal Radiol 1987;16:607-11.
6. Koski JM, Anttila PJ, Isomaki HA. Ultrasonography of the adult hip joint. Scand J Rheumatol 1989;18:113-7.
7. Shiv VK, Jain AK, Taneja K, Bhargava SK. Sonography of hip joint in infective arthritis. Can Assoc Radiol J 1990;
41:76-8.
8. Frankel DA, Bargiela A, Bouffard JA, Craig JG, Shirazi KK, van Holsbeeck MT. Synovial joints: evaluation of in- traarticular bodies with US. Radiology 1998;206:41-4.
9. Meaney JF, Cassar-Pullicino VN, Etherington R, Ritchie DA, McCall IW, Whitehouse GH. Ilio-psoas bursa enlar- gement. Clin Radiol 1992;45:161-8.
10. Fessell DP, van Holsbeeck MT. Sonography of the hip. In:
van Holsbeeck M, Introcaso JH, editors. Musculoskeletal ultrasound. 2nd ed. St. Louis: Mosby; 2001. p.573-86.
11. Swartout R, Compere EL. Ischiogluteal bursitis: the pain in the arse. JAMA 1974;227:551-2.
12. van Holsbeeck MT, Introcaso JH. Sonography of muscle.
In: van Holsbeeck M, Introcaso JH, editors. Musculoskel- etal ultrasound. 2nd ed. St. Louis: Mosby; 2001. p.23-75.
13. Fornage BD, Touche DH, Segal P, Rifkin MD. Ultrasono- graphy in the evaluation of muscular trauma. J Ultrasound Med 1983;2:549-54.
14. Temple HT, Kuklo TR, Sweet DE, Gibbons CL, Murphey MD. Rectus femoris muscle tear appearing as a pseudo- tumor. Am J Sports Med 1998;26:544-8.
15. Kälebo P, Swärd L, Karlsson J, Peterson L. Ultrasonog- raphy in the detection of partial patellar ligament ruptures (jumper’s knee). Skeletal Radiol 1991;20:285-9.
16. Holt PD, Keats TE. Calcific tendonitis: a review of the usu- al and unusual. Skeletal Radiol 1993;22:1-9.
17. Sarkar JS, Haddad FS, Crean SV, Brooks P. Acute calcific tendonitis of the rectus femoris. J Bone Joint Surg [Br]
1996;78:814-6.
18. Pelsser V, Cardinal E, Hobden R, Aubin B, Lafortune M.
Extraarticular snapping hip: sonographic findings. Am J Roentgenol 2001;176:67-73.
19. Cardinal E, Buckwalter KA, Capello WN, Duval N. US of the snapping iliopsoas tendon. Radiology 1996;198:521-2.
20. Janzen DL, Partridge E, Logan PM, Connell DG, Duncan CP. The snapping hip: clinical and imaging findings in tran- sient subluxation of the iliopsoas tendon. Can Assoc Radiol J 1996;47:202-8
21. Howse AJ. Orthopaedists aid ballet. Clin Orthop 1972;
89:52-63.
22. Gibbon WW, Long G, Barron DA, O'Connor PJ. Compli- cations of orthopedic implants: sonographic evaluation. J Clin Ultrasound 2002;30:288-99.
23. van Holsbeeck MT, Eyler WR, Sherman LS, Lombardi TJ,
Mezger E, Verner JJ, et al. Detection of infection in loos- ened hip prosthesis: efficacy of sonography. Am J Roentge- nol 1994;163:381-4.
24. Adam R, Hendry GM, Moss J, Wild SR, Gillespie I.
Arthrosonography of the irritable hip in childhood: a review of 1 year’s experience. Br J Radiol 1986;59:205-8.
25. Peck J. Ultrasound of the painful hip in children. Br J Radiol 1986;59:205-8.
26. Yen ZS, Wang HP, Ma HM, Chen SC, Chen WJ. Ultraso- nographic screening of clinically-suspected necrotizing fascitis. Acad Emerg Med 2002;9:1448-51.
27. Robben SGF. Ultrasonography of musculoskeletal in- fections in children. Eur Radiol 2004;14:165-7.
28. Wilson DJ. Soft-tissue and joint infection. Eur Radiol 2004;14(suppl 3):64-71.
29. Beck M, Sledge JB, Gautier E, Dora CF, Ganz R. The anat- omy and function of the gluteus minimus muscle. J Bone Joint Surg Br 2000;82:358-63.
30. Dunn T, Heller CA, McCarthy SW, Dos Remedios C.
Anatomical study of the “trochanteric bursa”. Clin Anat 2003;16:233-40.
31. Pfirrmann C, Chung C, Theurmann N, Trudell D, Resnick D. Greater trochanter of the hip: attachment of the abductor mechanism and a complex of three bursae-mr imaging and MR bursography in cadavers and MR imaging in asympto- matic volunteers. Radiology 2001;221: 469-77.
32. Kingzett-Taylor A, Tirman PF, Feller J, McGann W, Prieto V, Wischer T etc. Tendinosis and tears of gluteus medius and minimus muscles as a cause of hip pain: MR imaging findings. AJR 1999;173:1123-6.
33. Kong A, Van der Vliet A, Zadow S. MRI and US of gluteal tedninopathy in greater trochanteric pain syndrome. Eur Radiol 2007;17:1772-83.