https://doi.org/10.35827/cp.2020.19.2.124
접수일 : 2020 년 7 월 28 일 , 게재승인일 : 2020 년 8 월 14 일 책임저자 : 강시현 , 서울시 동작구 흑석로 102
06973, 중앙대학교병원 재활의학과
Tel: 02-6299-1865, Fax: 02-6298-1866 E-mail: [email protected]
대상포진후 상완신경총병증으로 진단된 편측 상지의 통증과 위약
중앙대학교병원 재활의학과
조준모ㆍ강시현ㆍ서경묵ㆍ김돈규ㆍ김두환ㆍ신현이
Pain and Weakness on Unilateral Upper Extremity Diagnosed as Brachial Plexopathy after Herpes Zoster Infection
Junmo Cho, M.D., Si Hyun Kang, M.D., Ph.D., Kyung Mook Seo, M.D., Ph.D., Don-Kyu Kim, M.D., Ph.D., Du Hwan Kim, M.D., Ph.D. and Hyun Iee Shin, M.D.
Department of Physical Medicine & Rehabilitation, Chung-Ang University College of Medicine, Seoul, Korea
Motor paralysis is a less common neurologic complication of herpes zoster. Until now, a few cases have been reported, and most of these cases showed brachial plexopathy involving one or two segments. We report a patient with pain and weakness on upper extremity diagnosed as brachial plexopathy after herpes zoster infection. An 88-year-old female patient complained not only tingling sense, pain, and swelling on right whole arm, but also weakness on this right upper extremity.
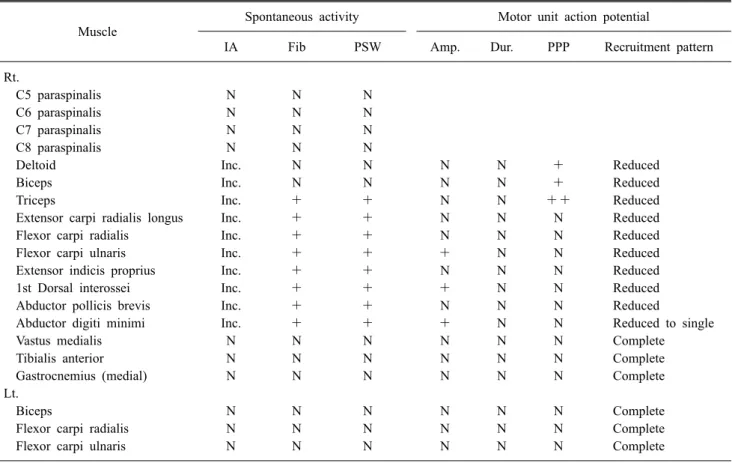
On physical examination, weakness is seen in right shoulder abductionㆍshoulder flexionㆍelbow flexionㆍelbow extensionㆍ wrist extension (grade 4), finger flexionㆍfinger abductionㆍfinger extensionㆍfinger DIP flexion (grade 3). In electrodiagnostic study and magnetic resonance imaging study, she was diagnosed as the brachial plexopathy, whole branch involved. This is the only case of post-herpetic brachial plexopathy involving whole branch in domestic. (Clinical Pain 2020;19:124-128) Key Words: Brachial plexus neuropathy, Herpes zoster, Electrodiagnosis
INTRODUCTION
Herpes zoster is an infectious disease characterized by vesicobullous skin eruptions in a dermatomal distribution and neurological complication.
1After primary varicella in- fection, the virus is latent in the ganglia of sensory cranial nerves and spinal dorsal root ganglia.
In elderly and in immunocompromised individuals, Varicella-zoster virus (VZV) reactivates and travels along the sensory nerves to the skin, causing the distinctive pro- dromal pain followed by eruption of the rash.
2The most common neurologic complication of herpes zoster is chronic pain, and motor paralysis is a less common complication.
3Until now, a few cases have been reported about motor pa- ralysis as brachial plexopathy after herpes zoster infection.
4,5Most of these cases showed brachial plexopathy involving
one or two segments, and in this case report we report a patient with brachial plexopathy involving whole branch confirmed by needle electromyography and magnetic reso- nance imaging study.
CASE REPORT
An 88-year-old female patient visited the hospital with bullous skin lesion in neck, right whole arm. She com- plained tingling sense, pain, and swelling on the involved area. Under diagnosis of Herpes zoster, she took the an- ti-viral agents, famciclovir (FAMVIR Tab 250 mg;
Novartis Korea., Seoul, Korea). Three days later, the bul- lous skin lesion in hands proceeded to the proximal part of the body, and pain of right upper extremity was aggravated. She was admitted in the neurology department and her symptoms were improved with proper medication (intravenous methylprednisolone 250 mg [SALON INJ;
Hanlim Pharm Co., Ltd., Seoul, Korea] 2 days, intravenous
aciclovir [ZOYLEX INJ 250 mg/10 ml; Korea United
Pharm. INC., Seoul, Korea] per 8 hours 7 days, and famci-
clovir [FAMVIR Tab 250 mg; Novartis Korea., Seoul,
Fig. 1. Chronic scar change of bullous skin lesion in right upper extremity two months after the onset of Herpes zoster infection.
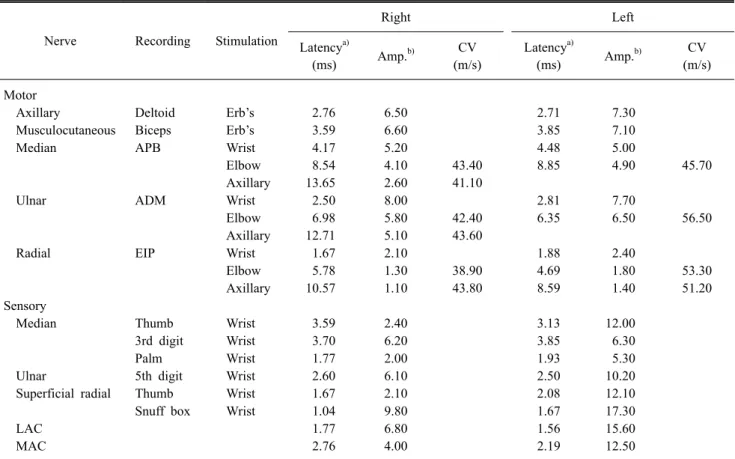
Table 1. Nerve Conduction Study
Nerve Recording Stimulation
Right Left
Latency
a)(ms) Amp.
b)CV
(m/s)
Latency
a)(ms) Amp.
b)CV
(m/s)
Motor
Axillary Deltoid Erb’s 2.76 6.50 2.71 7.30
Musculocutaneous Biceps Erb’s 3.59 6.60 3.85 7.10
Median APB Wrist 4.17 5.20 4.48 5.00
Elbow 8.54 4.10 43.40 8.85 4.90 45.70
Axillary 13.65 2.60 41.10
Ulnar ADM Wrist 2.50 8.00 2.81 7.70
Elbow 6.98 5.80 42.40 6.35 6.50 56.50
Axillary 12.71 5.10 43.60
Radial EIP Wrist 1.67 2.10 1.88 2.40
Elbow 5.78 1.30 38.90 4.69 1.80 53.30
Axillary 10.57 1.10 43.80 8.59 1.40 51.20
Sensory
Median Thumb Wrist 3.59 2.40 3.13 12.00
3rd digit Wrist 3.70 6.20 3.85 6.30
Palm Wrist 1.77 2.00 1.93 5.30
Ulnar 5th digit Wrist 2.60 6.10 2.50 10.20
Superficial radial Thumb Wrist 1.67 2.10 2.08 12.10
Snuff box Wrist 1.04 9.80 1.67 17.30
LAC 1.77 6.80 1.56 15.60
MAC 2.76 4.00 2.19 12.50
Amp: amplitude, CV: conduction velocity, APB: abductor pollicis brevis, ADM: abductor digiti minimi, EIP: extensor indicis proprius, LAC: lateral antebrachial cutaneous, MAC: medial antebrachial cutaneous.
a)
All motor and sensory latencies are onset latencies.
b)