■ 접 수 : 2012년 12월 14일, 수정 : 2012년 12월 22일, 채택 : 2013년 1월 8일
■ 교신저자 : 신병철, 경남 양산시 물금읍 금오로 20 부산대학교한방병원 한방재활의학과
한방재활의학과학회지에 수록된 무작위대조임상연구의 양적, 질적 분석(1)
이현엽*⋅허광호†⋅조현우†⋅황의형†⋅신미숙†⋅신병철†
부산대학교한방병원 한방재활의학과*, 부산대학교 한의학전문대학원†
Randomized Controlled Clinical Trials in the Journal of Oriental Rehabilitation Medicine
: A Quantitative and Qualitative Analysis(1)
Hyeon-Yeop Lee, O.M.D.*, Kwang-Ho Heo, O.M.D.†, Hyun-Woo Cho, O.M.D.†
Eui-Hyoung Hwang, O.M.D.†, Mi-Suk Shin, O.M.D.†, Byung-Cheul Shin, O.M.D.†
Dept. of Oriental Rehabilitation Medicine, Pu-San National University Korean Medicine Hospital*
School of Korean Medicine, Pu-San National University
†Objectives :
The aim of this study is to assess the quantity and quality of randomized controlled clinical trials(RCTs) published in the journal of oriental rehabilitation medicine(JORM).
Methods :
After searching RCTs from all the articles published in the JORM from the inception(1991) to Oct, 2012, quantity assessment were made on the study design, sample size, main intervention, intervention versus control design and medical condition. Quality assessment were made on the cochrane risk of bias(RoB) check list. Assessment was performed by 2 independent reviewers and disagreement was discussed based on concensus of all authors.
Results :
Among the 1013 articles, total 59 RCTs were published. First RCT was published in 1994. 49 RCTs were parallel 2-arm designed. Average sample size was 35.1 per study and 16.3 per arm. The most common medical condition is musculoskeletal disease(30.5%). Quality from cochrane RoB was generally low.
Conclusions :
Though RCTs published in JORM were increasing, the quality remains low. Researchers should make a effort to follow the RoB checklists and improve the quantity and quality of studies.
Key words : Evidence based medicine, Randomized controlled clinical trials, Risk of bias, Journal of oriental rehabilitation medicine, Quality assessment
Ⅰ. 서 론
1979년 영국의 역학자 Archie Cochrane이 ‘근 거중심의학(evidence based medicine, EBM)’의 개념을 제시한 이후, 이것은 의학계의 새로운 패 러다임으로서 나날이 발전하고 있다
1). 한의학계 에서도 이러한 시대적 흐름에 따라 근거중심의학 에 대한 관심과 연구가 급격히 증가하는 추세이 다.
근거중심의학은 1990년대부터 국제의학계에서 널리 받아들여지기 시작한 임상의학의 새로운 방 법론이다. 근거중심의학의 핵심정의는 ‘현재 존 재하는 최고의 근거를 양심적이고, 명백하며, 분 별 있게 이용하여 개별 환자의 치료를 결정한다’
는 것이다
2). 근거중심의학은 근거로서의 가치가 크지 않은 비체계적, 단편적 경험에 근거한 임상 적 판단에 대한 반성적 태도를 강조하면서, ‘체계 적 연구’의 결과로 확인된 임상적 근거에 기초하 여 임상적 결정을 내리도록 하고 있다. 여기서
‘체계적 연구’라 함은 일반적으로 ‘무작위대조임 상연구(randomized controlled clinical trial, RCT)’
를 의미한다
3).
무작위대조임상연구는 실험군과 대조군을 무 작위로 설정한 뒤 투입되는 중재를 연구자와 피 실험자가 알 수 없게 제공하여 어떠한 결과가 나 오는지를 보는 연구로, 가장 강력한 설득력을 가 진 연구 설계 방법
4)이며 근거중심의학의 근간이 된다.
하지만 연구 설계 과정에서 오류가 발생하거 나 연구 결과를 불완전하게 기술하면 치료효과를 추정하는데 있어 비뚤림을 유발하게 되어 적절한 연구 설계와 완전한 결과 기술이 매우 중요한 요 소이다
5).
무작위대조임상연구의 비뚤림 위험평가는 Cochrane
group의 Risk of bias(RoB) 도구가 가장 보편적 으로 활용된다. Risk of bias는 2005년 Cochrane Collaboration에서 무작위대조임상연구의 질을 평 가하기 위해 만든 도구로서, 5가지의 비뚤림 위험 에 대한 7가지의 평가항목으로 구성되어 있다
6).
한방재활의학과학회지는 1991년 동의물리요법 학회지라는 이름으로 최초로 발간되었으며 1996 년부터 한방재활의학과학회지로 이름을 바꾸어 2012년 10월까지 현재 총 62권이 발간되었다. 본 논문은 현재까지 발간된 동의물리요법학회지를 포함한 한방재활의학과학회지에 수록된 무작위 대조임상연구 논문을 대상으로 양적・질적 평가를 시행하여 개선점을 찾아보고, 향후 발표될 무작 위대조임상연구의 질적 향상을 도모하기 위하여 기획되었다.
본 논문은 내용이 다소 방대하여 지면상 두 편 으로 보고될 것이다. 현재까지 발간된 동의물리 요법학회지와 한방재활의학과학회지에 수록된 무 작위대조임상연구를 선정하여 먼저 양적 평가와 Risk of bias 도구를 사용한 질적 평가를 시행하여 보고하고, 다른 논문에서는 CONSORT(consolidated standards of reporting trials) Statement의 CONSORT 2010 checklist
7)를 이용하여 평가하고 그 중에서 침 연구는 STRICTA(standards for reporting interventions in clinical trials of acupuncture)
8)를 잘 준수하고 있는지 평가하여 무작위대조임상연구에 대해 좀 더 심화된 분석을 진행하여 보고하도록 하겠다.
Ⅱ. 방 법
1. 연구 대상 및 문헌 검색
최초의 발간연도인 1991년부터 2012년 10월까
지 발간된 한방재활의학과학회지에 수록된 모든
논문을 대상으로 하였다. 논문 검색은 한방재활 의학과학회 홈페이지(http://www.ormkorea.org) 를 기본으로 하였으며 주제에 제한을 두지 않고 전수조사 하였다. 데이터베이스에서 검색이 불가 능한 경우 출판이 이루어진 학회지를 입수하여 직접 목차와 내용을 전수조사 하였다.
2. 무작위대조임상연구의 선정 기준
먼저 사람을 대상으로 하고, 실험군과 대조군 을 설정하며, 전향적인 연구 설계를 가지며, 중재 가 개입되었고, 연구 방법에서 군배정이 무작위 로 이루어진 연구를 선정하였다. 연구 방법에 ‘무 작위’ 혹은 ‘random’이라는 용어가 없더라도 제 목이나 초록에서 언급된 경우 포함하였다. 주저 자를 포함한 2인의 독립된 저자(HYL, KHH)가 제목과 초록을 통해 1차 검토를 한 후 걸러진 논 문들에 대하여 2차로 전문을 검토하여 최종 선정 하였다. 서로 의견이 다른 경우 연구에 참여한 모든 저자들과의 토의를 통하여 결정하였다.
3. 제외 기준
동물실험, 세포실험, 문헌고찰 등 사람 대상이 아닌 경우와 대조연구가 아닌 case report, case series, 관찰연구, 후향적연구 및 전후비교연구, 환자대조군연구 등과 무작위 배정이 안 된 대조 임상연구는 그 수는 파악하되 연구의 평가에서는 제외하였다.
4. 무작위대조임상연구의 양적 평가
분류된 무작위대조임상연구를 발간 연도별로 분류하여 그래프로 나타내었으며 해당 논문들을
설계 형태 및 중재의 종류, 군 배정, 대상 질환 등으로 분류하여 백분율로 나타내었다.
5. 무작위대조임상연구의 질적 평가
Cochrane group의 Risk of bias 도구를 사용하여 선택 비뚤림(selection bias), 실행 비뚤림(performance bias), 결과 확인 비뚤림(detection bias), 탈락 비 뚤림(attrition bias), 보고 비뚤림(reporting bias) 등 다섯 가지의 비뚤림 위험을 평가하기 위해 Cochrane Handbook의 평가 기준
9)을 참고하여 각 7개의 평가항목에 대하여 비뚤림 위험을 ‘높 음(high)', '낮음(low)', '불확실(unclear)'의 세 가 지로 판정하였다. 2인의 평가자(HYL, KHH)는 Cochrane group에서 발간된 Risk of bias에 대한 세부 설명을 참조로 하여 독립적으로 평가를 시 행하였고, 평가 후 2인의 평가를 비교하여 서로 다른 것은 상호 토의를 통하여 통일하였다. 전체적 인 결과는 Cochrane group에서 제공하는 Review Manager(RevMan) 5.2 프로그램을 사용하여 그 래프로 나타내었다.
Ⅲ. 결 과
1. 연구의 흐름
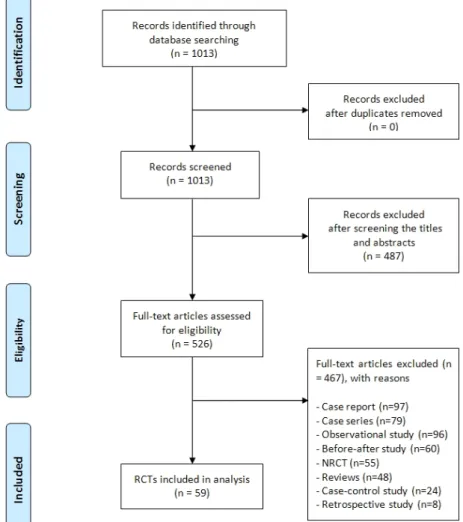
최초의 출간연도인 1991년부터 2012년 10월까
지 총 1013개의 논문이 검색되었다. 그 중 제목
과 초록을 살펴보아 사람을 대상으로 하지 않는
487편의 논문이 배제되었고, 원문 검토를 통해
97편의 case report, 79편의 case series, 96편의
관찰연구, 60편의 전후비교연구, 55편의 비무작위
대조임상연구(non-randomized controlled clinical
trial, NRCT), 48편의 고찰논문, 24편의 환자대조 군연구, 8편의 후향적연구가 배제되어 최종 59편
의 무작위대조임상연구가 포함되었다 (Fig. 1).
Fig. 1. PRISMA flow diagram for literature search.
RCT : randomized controlled clinical trial NRCT : non-randomized controlled clinical trial
2. 양적 분석
무작위대조임상연구로 분류된 논문은 총 59편 으로 전체 논문 1013편의 5.8%에 해당하였다. 무 작위대조임상연구가 처음으로 학회지에 실린 것
은 1994년도이며, 2003년 이후로 본격적으로 발
표되기 시작하였다. NRCT는 1992년에 처음 학회
지에 실렸으며 1998년부터 본격적으로 발표되기
시작했다(Fig. 2).
Fig. 2. Number of RCTs and NRCTs according to publication year.
RCT : randomized controlled clinical trial NRCT : non-randomized controlled clinical trial
또한 포함된 59편의 RCT 중에서 2-arm parallel study design이 49편(83.1%)으로 압도적으로 많 았으며, 연구에 포함된 환자 수의 경우 연구 당 약 35.1명(최소 10명~최대 125명), arm 당 약 16.3명 으로 나타났다.
중재와 관련해서는 침 연구가 19편(32.2%), 추 나 및 운동치료 관련 연구가 15편(25.4%), 한약 연구가 10편(16.9%), 한방물리요법 연구가 8편 (13.6%), 부항 연구가 2편(3.4%), 보완대체의학 (complementary and alternative medicine, CAM) 관련 연구가 5편(8.5%)으로 침 연구가 가장 많았 다.
실험군-대조군 설정에 있어서는 해당중재와 기 타 치료의 병행과 기타 치료 단독 시행의 비교가 25편(42.4%), 해당 중재의 다른 형태와의 비교가 13편(22.0%), sham 치료와의 비교가 11편(18.6%), 무처치군과의 비교가 6편(10.2%), 다른 치료법과 의 비교가 4편(6.8%) 으로 나타났다(Table Ⅰ).
Characteristics n(%)
Study design 59(100.0)
Parallel, 2-arm 49(83.1)
Parallel, 3-arm 7(11.9)
Parallel, 4-arm 3(5.1)
Sample size(n)
mean per study(range) 35.1(10~125)
mean per arm 16.3
Main Intervention* 59(100.0)
Acupuncture 19(32.2)
Acupuncture alone 10
Acupuncture + Moxibustion 1
Acupuncture + Exercise 1
Electro-acupuncture 2
Electro-acupuncture + Exercise 2
Pharmacopuncture 3
Herbal medicine 10(16.9)
Herbal medicine alone 7
Herbal medicine + Exercise 1
Iontophoresis treatment† 2
Cupping 2(3.4)
Cupping alone 2
Chuna manipulation / Exercise 15(25.4)
Chuna manipulation alone 9
Chuna manipulation + Burning Acupuncture 1
Exercise alone 4
Exercise + Diet 1
Oriental physical therapy 8(13.6)
CAM therapy‡ 5(8.5)
Intervention vs. Control design 59(100.0) main intervention vs. no treatment 6(10.2) main intervention vs. sham treatment 11(18.6) main intervention vs. different types of same main
intervention 13(22.0)
main intervention vs. other main intervention 4(6.8) main intervention + other intervention(s) vs. other
intervention(s) alone 25(42.4)
RCT : randomized controlled clinical trial
*Main intervention is oriental medicine treatment include acupuncture, herbal medicine, cupping, chuna manipulation, exercise and oriental physical therapy.
†Iontophoresis is the induction of ionized herb-medications topically via low level electric current.
‡Complementary and alternative medicine(CAM) therapies include meditation(n=1), aroma therapy(n=1), splint(n=1), mind-body therapy(n=1) and visual bio-feedback training(n=1).
Table Ⅰ. Characteristics of RCTs in Journal of Oriental Rehabilitation Medicine
논문에서 다루고 있는 질환에 대해서는 근골 격계질환이 18편(30.5%)으로 가장 많았고, 그 중 에서도 요통이 7편으로 가장 많았다. 순환기계질 환은 17편(28.8%)이 모두 중풍에 대한 논문이었 다. 그 외에는 비만이 5편(8.5%), 두통 2편(3.4%), 불면 1편(1.7%), 알코올중독 1편(1.7%)이었다. 건 강인에 대한 생리적 특성 및 기전연구가 15편 (25.4%)으로 대상 질환중에 세 번째로 많은 것도 중요한 특징이다(Table Ⅱ).
Medical conditions n(%)
Musculoskeletal Disease 18(30.5)
Low back pain (including disk disorder) 7
Ankle sprain 5
Knee osteoarthritis 2
Neck pain 2
Temporo-mandibular joint disorder 1
Axial Spondyloarthritis 1
Circulatory disease 17(28.8)
Stroke 17
Obesity 5(8.5)
Headache 2(3.4)
Insomnia 1(1.7)
Alcohol addiction 1(1.7)
Healthy subject(s)* 15(25.4)
Total 59(100.0)
RCT : randomized controlled clinical trial
*Examined healthy subjects for autonomic nervous system function(n=1), acupuncture sensation comparison(n=1), body temperature(n=1), change of body temperature and blood(n=1), change of body composition and cardiopulmonary function(n=1), hormonal change(n=1), muscle activity and pain reception(n=1), muscle flexibility(n=1), muscle tension(n=2), physiological activity (n=2), stress(n=1), sensation threshold(n=1) and recovery after exercise(n=1).
Table Ⅱ. Categories of Medical Conditions of RCTs in Journal of Oriental Rehabilitation Medicine
3. 질적 분석
Cochrane group의 Risk of bias 도구를 사용하 여 최종 분류된 59편의 무작위대조임상연구논문 을 평가한 결과, 무작위 배정순서 생성(random
sequence generation) 항목에서 6.8%는 비뚤림 위험이 높음, 23.7%는 낮음으로 평가되었고 배정 순서 은폐(allocation concealment) 항목에서 3.4%
는 높음, 13.6%는 낮음으로 평가되었고 연구 참여자 와 연구자에 대한 눈가림(blinding of participants and personnel) 항목에서 8.5%는 높음, 13.6%는 낮음으로 평가되었고 결과 평가에 대한 눈가림 (blinding of outcome assessment) 항목에서는 8.5%가 낮음으로 평가되었고 불충분한 결과자료 (incomplete outcome data) 항목에서 32.2%는 높 음, 5.1%는 낮음으로 평가되었고 선택적 보고 (selective reporting) 항목 전체는 높음이나 낮음 으로 평가된 논문이 없었다. 그 외 비뚤림(other bias) 항목은 6.8%가 높음으로 평가되었다. 높음 과 낮음으로 평가된 부분 이외에는 모두 불확실 로 평가되었다(Fig. 3).
Fig. 3. Risk of bias graph of RCTs in Journal of Oriental Rehabilitation Medicine.