Introduction
Acute calcific tendinitis affecting the hand and wrist is an uncommon inflammatory disorder. Calcific deposits tend to arise in tendons secondary to chronic inflammation and sometimes cause acute calcific
tendinitis. The calcific tendinitis of the flexor carpi ulnaris occurs at its insertion into the pisiform. This is the most common type of calcific tendinitis in the hand and wrist and may cause ulnar nerve compression as the nerve traverses Guyon’s canal. It is often resolved without treatment. Also, most patients experience rapid pain relief with the use of anti-inflammatory agents and immobilization. Other treatments options include heat modality, cholchicine, injection using local anesthetics or corticosteroids, and mechanical disruption or aspiration of the calcification. In case of acute ulnar nerve compression, urgent surgical decompression may be necessary.1 In the last few
체외 충격파 치료 이후 발생한 기욘 터널 증후군 - 증례보고 -
유현준1, 권희규1, 박종웅2, 한아름3, 이보람4, 김민현1
고려대학교 의과대학 고려대학교안암병원 1재활의학과교실, 2정형외과교실,
3경인의료재활센터병원 재활의학과, 4국립재활원 재활의학과
Guyon’s Canal Syndrome as a Complication of Extracorporeal Shock Wave Therapy - A Case Report -
Hyun-Joon Yoo1, Hee-Kyu Kwon1, Jong Woong Park2, A-Reum Han3, Boram Lee4, Min-Hyun Kim1
Departments of 1Physical Medicine & Rehabilitation, 2Orthopedic Surgery, Korea University Anam Hospital,
Korea University College of Medicine, Seoul, 3Department of Physical Medicine & Rehabilitation, Gyeongin Rehabilitation Center Hospital, Incheon,
4Department of Public Rehabilitation and Health, National Rehabilitation Center, Seoul, Korea
Received July 5, 2016
Revised (1st) August 21, 2016, (2nd) September 4, 2016 Accepted September 7, 2016
Corresponding Author: Hee-Kyu Kwon
Department of Physical Medicine & Rehabilitation, Korea University Anam Hospital, Korea University College of Medicine, 5 ga 126-1, Anam-dong, Sungbuk-gu, Seoul 02841, Korea
Tel: 82-2-920-6483, Fax: 82-2-929-9951, E-mail: [email protected]
Extracorporeal shock wave therapy (ESWT) is an alternative treatment for various musculoskeletal disorders. However, there are some potential side effects of the therapy such as soft tissue swelling, skin erosion and nerve damage.
Therefore, physicians should be aware of the proper usage and precautions for ESWT. This is a case report of a healthy woman who was diagnosed with ulnar neuropathy at the wrist, Guyon’s canal syndrome after receiving ESWT on her wrist. We also suggest some possible mechanisms for the ulnar neuropathy at the wrist in this case.
Key Words: extracorporeal shock wave therapy, Guyon’s canal syndrome, ulnar neuropathies
Copyright © by Korean Association of EMG Electrodiagnostic Medicine
This is an Open Ac cess article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ISSN 1229-6066 https://doi.org/10.18214/jkaem.2016.18.2.74 J Korean Assoc EMG Electrodiagn Med 18(2):74-79, 2016
J Korean Assoc
Electrodiagn MedEMG
years, extracorporeal shock wave therapy (ESWT), a physical modality that uses pressure waves has been used as a minimally invasive option for the treatment of refractory soft-tissue disorders such as plantar fasciitis, lateral epicondylitis and chronic calcific tendinitis of the shoulder. Since ESWT is effective and minimally invasive, there will be a great increase in the use of ESWT in the near future. According to many research articles, several complications regarding the shock wave in experimental settings have been reported.
Nevertheless, there are few case reports about the complications of ESWT, which are clinically important.
This is the first case report with operative findings and its clinical course after successful treatment of an iatrogenic peripheral nerve injury, Guyon’s canal syndrome, following the use of ESWT for the treatment of calcific tendinitis in the flexor carpi ulnaris. This report led us to be more precautious regarding compli- cations before prescribing ESWT.
Case Report
A 55-year-old healthy woman visited the Department
of Physical Medicine and Rehabilitation, Korea University, College of Medicine on July 31, 2014 with complaints of hand weakness. She had suffered from intermittent pain around the left pisiform area for 10 years after falling on her left hand. She visited the private orthopedic clinic because the pain increased over several months. Based on the clinical symptoms and plain radiographic finding showing calcifications around the distal flexor carpi ulnaris tendon (Fig. 1), she was diagnosed with calcific tendinitis of the left flexor carpi ulnaris. And she received ESWT on the lesion on June 15, 2014. The dosage of ESWT was 1,500 shockwaves with an intensity of 2.0 bar. Immediately after the 1st session of ESWT, she felt a tingling sensa- tion in the left 4th and 5th fingers and hand weakness developed on the next day. The weakness became aggravated over the next couple of weeks, and she was referred to us for further evaluation.
All the deep tendon reflexes were normoactive in the left upper extremity. There was no muscle wasting, including in the hand intrinsic muscles. According to the Medical Research Council (MRC) Scale, muscle strength for finger abduction, adduction and 5th finger
A B
C D
Fig. 1. Plain radiographic image (A) and T2 weighted magnetic resonance image in coronal view (B) and axial view (C and D). Plain radiographs of left wrist revealed calcification on the left distal flexor carpi ulnaris tendon (small arrow). Edema along the flexor carpi ulnaris tendon (large arrow) and adjacent soft tissue (arrowhead) at the pisiform were noted. Ulnar nerve (curved arrow) was observed at distal wrist crease.
opposition were grade 4. Other muscles of the left
upper extremity were normal. Sensation to light touch was intact. Tinel’s sign was positive on Guyon’s canal tapping and Wartenberg’s sign and Froment’s sign were positive on the left side.
Magnetic resonance imaging revealed edema along the left flexor carpi ulnaris tendon, abductor digiti minimi muscle and adjacent soft tissue at the pisiform (Fig. 1). Ultrasonography demonstrated ulnar nerve swelling between 1 cm and 2 cm distal to the wrist crease and calcification with loss of fibrillar patterns at the distal flexor carpi ulnaris tendon (Fig. 2). Diffuse bony irregularity of the pisiform with surrounding soft tissue swelling was also noted.
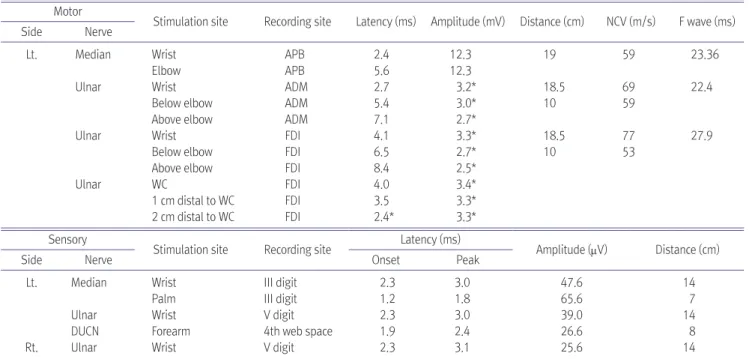
An electrodiagnostic study was performed on July 31, 2014. On the nerve conduction study, the left ulnar compound muscle action potential (CMAP) had low amplitudes for the abductor digiti minimi muscle and the first dorsal interossei muscle recordings. A short segmental conduction study revealed a conduction
delay between 1 cm and 2 cm distal to the wrist crease (Table 1). On needle electromyography, abnormal spontaneous activities and polyphasic motor unit potentials with reduced recruitment patterns were noted in the left abductor digiti minimi and the first dorsal interossei muscles (Table 2). The patient was diagnosed with acute left incomplete ulnar neuropathy at the wrist (Guyon’s canal syndrome, type II2), concurrent with Wallerian degeneration and a conduction delay between 1 cm and 2 cm distal to the wrist crease.
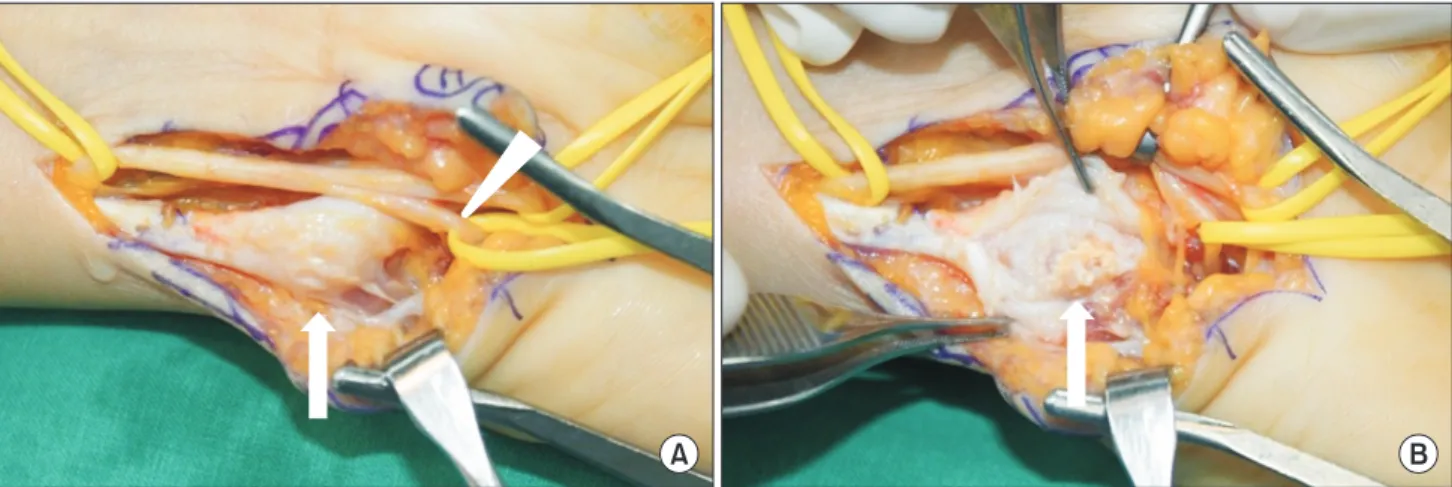
She underwent an exploratory operation on Septem- ber 11, 2014. Flexor carpi ulnaris tendon hypertrophy and large calcification over the pisiform were observed.
The ulnar nerve motor branch was compressed by a thickened flexor carpi ulnaris tendon. After splitting the flexor carpi ulnaris tendon, abundant calcific materials were identified (Fig. 3). Ulnar nerve neurolysis and calcific material removal were performed. Two months after the operation, muscle strength improved, and
E F
A B C
D
Fig. 2. Ultrasonography of ulnar nerve around the wrist crease. Left ulnar nerve circumferences were 1.09 cm, 1.27 cm, and 1.24 cm at distal wrist crease, 1 cm distal to wrist crease, and 2 cm distal to wrist crease, respectively. Left ulnar nerve swelling was observed between 1 cm and 2 cm distal to wrist crease compared to right side. (A) indicates left distal wrist crease; (B), 1 cm distal to wrist crease; (C), 2 cm distal to wrist crease. (D) indicates right distal wrist crease; (E), 1 cm distal to wrist crease; (F), 2 cm distal to wrist crease.
claw hand deformity as well as the Wartenberg’s sign and Froment’s sign disappeared.
Discussion
Extracorporeal shock wave is a focused, single-pulse acoustic wave of microsecond duration. It was initially applied in urology to disintegrate kidney and ureter stones two decades ago. Nowadays, ESWT is widely used for the treatment of certain soft-tissue disorders, such as calcifying tendinitis of the rotator cuff, lateral epicondylitis and plantar fasciitis.3 Moreover, it has
also been known as a stimulator of bone healing and therefore, suggested as a treatment of delayed union or nonunion. However, the Food and Drug Administration approved its use for only plantar fasciitis and lateral epicondylitis.
The therapeutic mechanism underlying the effect of ESWT on calcifying tendinopathy is uncertain.
According to Loew et al.4 the shock wave increases pressure within the target lesion, inducing fragmen- tation and cavitation of the amorphous calcifications, which finally leads to disintegration and elimination of the deposits. These mechanical actions can also
Table 1. Motor and Sensory Nerve Conduction Study Motor
Stimulation site Recording site Latency (ms) Amplitude (mV) Distance (cm) NCV (m/s) F wave (ms)
Side Nerve
Lt. Median Wrist APB 2.4 12.3 19 59 23.36
Elbow APB 5.6 12.3
Ulnar Wrist ADM 2.7 3.2* 18.5 69 22.4
Below elbow ADM 5.4 3.0* 10 59
Above elbow ADM 7.1 2.7*
Ulnar Wrist FDI 4.1 3.3* 18.5 77 27.9
Below elbow FDI 6.5 2.7* 10 53
Above elbow FDI 8.4 2.5*
Ulnar WC FDI 4.0 3.4*
1 cm distal to WC FDI 3.5 3.3*
2 cm distal to WC FDI 2.4* 3.3*
Sensory
Stimulation site Recording site Latency (ms)
Amplitude (μV) Distance (cm)
Side Nerve Onset Peak
Lt. Median Wrist III digit 2.3 3.0 47.6 14
Palm III digit 1.2 1.8 65.6 7
Ulnar Wrist V digit 2.3 3.0 39.0 14
DUCN Forearm 4th web space 1.9 2.4 26.6 8
Rt. Ulnar Wrist V digit 2.3 3.1 25.6 14
NCV: nerve conduction velocity, APB: abductor pollicis brevis muscle, ADM: Abductor digiti minim muscle, FDI: first dorsal interossei muscle, DUCN: dorsal ulnar cutaneous nerve, WC: wrist crease, Lt: Left, Rt: Right
Abnormal values are represented with asterisk
Table 2. Needle electromyography Study
Muscle Insertional
activity
Spontaneous activity
Motor unit action potentials
Normal Polyphasia Amplitude Duration IP
Lt. Brachioradialis N - N F
Pronator teres N - N F
Flexor carpi ulnaris N - N F
Extensor digit. comm. N - N F
Abductor digiti minimi F&P(+++) (400 μV) Polyphasic Large (6 mV) R
First dorsal interosseus F&P(+) Polyphasic R
Lt. C5/6, C6/7 PVM N -
N: normal, F: full, R: reduced, F&P: fibrillation potentials and positive sharp waves, IP: interference pattern, PVM: paravertebral muscle, Lt: Left
activate an inflammatory response on a cellular level
with leukocyte recruitment, extravasation, chemotaxis, and phagocytosis, which promote wound healing.
Wang et al.5 hypothesized that the shock wave enhances neovascularization and circulation at the tendon-bone junction and helps the absorption of calcium deposits on a molecular level. Others support the theory of hyperstimulation analgesia. According to this theory, pain is alleviated by a moderate to intense sensory input through stimulation of a brain stem feedback loop that exerts a descending inhibitory control of pain signal transmission.6
As stated above, owing to the direct tissue trauma and/or cavitation effects by ESWT, some complications can occur. Usually the side effects of ESWT are dose- dependent. Local soft-tissue swelling, cutaneous erosions, and skin reddening usually resolve sponta- neously after 48 hrs. When an energy level between 0.04 and 0.22 mJ/mm2 is used, pain and small hematomas are the main complications.7 Durst et al.8 reported a case of humeral head osteonecrosis after ESWT. They suggested that damage to the ascending branch of the anterior humeral circumflex artery, which is the main supply to the proximal humeral epiphysis, could cause osteonecrosis. Therefore, care must be taken when targeting calcium deposits at the intertubercular groove. Also, there is a clinical case
report about ESWT-related nerve injury. Shim et al.9 reported an iatrogenic ulnar neuropathy at the elbow after ESWT for the treatment of medial epicondylitis.
The patient underwent an exploratory operation and cubital tunnel release was performed although there was no other structural lesion compressing the ulnar nerve. Three months after the operation, pain on the right hand improved while hand weakness did not improve remarkably. They suggested that ESWT could cause ulnar neuropathy directly or in combination with regional inflammatory reaction. Compared to the above case, calcified materials which compressed the ulnar nerve motor branch existed in this case and after neurolysis and calcific material removal, pain and the hand weakness improved.
Two possible mechanisms can be suggested for this case of ulnar neuropathy at the wrist. First, the extracorporeal shock wave could have mechanically injured the neural tissues directly. The patient stated that she felt a tingling sensation and numbness on her left 4th and 5th fingers during the procedure and just after the 1st session of the ESWT. Considering the temporal relationship between symptoms and intervention as well as the anatomical course of the ulnar nerve, which is relatively superficial at the wrist, ESWT may have injured the ulnar nerve at the target lesion. Schelling et al.10 reported that ESWT generated compound action
A B
Fig. 3. Operative findings. (A) Flexor carpi ulnaris tendon hypertrophy and calcification (arrow) over the pisiform and ulnar nerve motor branch (arrowhead) compressed by thickened flexor carpi ulnaris tendon were observed. (B) Abundant calcific materials (arrow) were identified after splitting flexor carpi ulnaris tendon.
potentials and damaged the sciatic nerves of frogs in in-vitro experiments, which supports the possibility of direct nerve injury by ESWT. Second, Guyon’s canal is essentially a closed space surrounded by the volar and transverse carpal ligaments with medial and lateral bony margins. Any lesion within this region has the potential to compress the ulnar nerve. In this situation, a large calcified mass was found in the left flexor carpi ulnaris tendon during surgery. That means that the patient’s Guyon’s canal was relatively narrow and anatomically vulnerable to ulnar neuropathy. Even a small amount of regional inflammation and soft tissue swelling around the wrist which was exacerbated by ESWT could compress the ulnar nerve. Also, the calcified mass might have displaced after ESWT and this may compress the ulnar nerve.
After surgical decompression with removal of the calcified material, her symptoms improved. This clinical course suggests that some compressive lesions existed as well as direct nerve injury.
In conclusion, the possibility of peripheral nerve injury after ESWT always exists. Therefore, physicians should be careful not to injure the peripheral nerve when performing ESWT, especially when applying it near the course of a superficial nerve. Screening of structural abnormality and local edema using ultrasound or other imaging techniques might be helpful.
Conflicts of Interest
No conflicts of interest have been reported by the authors or by any individuals in control of the content of this
References
1. Torbati SS, Bral D, Geiderman JM: Acute Calcific Tendinitis of the Wrist. Journal of Emergency Medicine 2013: 44: 352- 354
2. Shea JD, Mcclain EJ: Ulnar-Nerve Compression Syndromes at and Below Wrist. Journal of Bone and Joint Surgery- American Volume 1969: A 51: 1095-1103
3. Speed CA: Extracorporeal shock-wave therapy in the management of chronic soft-tissue conditions. J Bone Joint Surg Br 2004: 86: 165-171
4. Loew M, Jurgowski W, Mau HC, Thomsen M: Treatment of calcifying tendinitis of rotator cuff by extracorporeal shock waves: a preliminary report. J Shoulder Elbow Surg 1995: 4:
101-106
5. Wang CJ, Wang FS, Yang KD, Weng LH, Sun YC, Yang YJ: The effect of shock wave treatment at the tendon-bone interface - an histomorphological and biomechanical study in rabbits.
Journal of Orthopaedic Research 2005: 23: 274-280
6. Ogden JA, Toth-Kischkat A, Schultheiss R: Principles of shock wave therapy. Clin Orthop Relat Res 2001: 8-17 7. Mouzopoulos G, Stamatakos M, Mouzopoulos D, Tzurbakis M:
Extracorporeal shock wave treatment for shoulder calcific tendonitis: a systematic review. Skeletal Radiol 2007: 36:
803-811
8. Durst HB, Blatter G, Kuster MS: Osteonecrosis of the humeral head after extracorporeal shock-wave lithotripsy. J Bone Joint Surg Br 2002: 84: 744-746
9. Shim JS, Chung SG, Bang H, Lee HJ, Kim K: Ulnar Neuropathy After Extracorporeal Shockwave Therapy: A Case Report. PM R 2015: 7: 667-670
10. Schelling G, Delius M, Gschwender M, Grafe P, Gambihler S: Extracorporeal shock waves stimulate frog sciatic nerves indirectly via a cavitation-mediated mechanism. Biophys J 1994: 66: 133-140