93
Review
ISSN 2465-8243(Print) / ISSN: 2465-8510(Online) https://doi.org/10.14777/uti.2016.11.3.93 Urogenit Tract Infect 2016;11(3):93-96
http://crossmark.crossref.org/dialog/?doi=10.14777/uti.2016.11.3.93&domain=pdf&date_stamp=2016-12-25
How Do You Diagnose Recurrent Urinary Tract Infections and Confirm the Diagnosis?
Hoon Choi, Jae Hyun Bae
Department of Urology, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
Recurrent urinary tract infections (UTIs) are the most prevalent conditions affected mainly by reinfection by the same bacteria in young women with no functional or anatomic problem. Recurrent UTIs present both storage (dysuria, irritative etc.) and voiding symptoms. For example, frequency subsequently followed by sexual intercourse is a powerful predictor of recurrent UTI. In patients with morbid situations or other factors, recurrent complicated infections or sepsis may be aggravated. Escherichia coli is the most common organism responsible for UTIs, but Pseudomonas, Proteus, Klebsiella, and other organisms are also frequent, particularly, in patients higher risk of complicated infections. Urine culture is not often needed to diagnose typical uncomplicated infection. Generally, urine culture with more than 10² colony-forming units/ml is used to diagnose UTIs in symptomatic patients. Recurrent UTIs could be managed with several techniques with the help of urine culture and by imaging studies when suspicious of anatomical abnormalities.
Keywords: Urinary tract infection; Culture; Anti-bacterial agents
Copyright 2016, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 1 August, 2016 Revised: 17 November, 2016 Accepted: 21 November, 2016
Correspondence to: Jae Hyun Bae http://orcid.org/0000-0001-9862-3545 Department of Urology, Korea University Ansan Hospital, Korea University College of Medicine, 123 Jeokgeum-ro, Danwon-gu, Ansan 15355, Korea Tel: +82-31-412-5190, Fax: +82-31-412-5194 E-mail: [email protected]
INTRODUCTION
Simple urinary tract infections (UTIs) occur in a sound host in cases of no functional or structural anomalies in the urinary tract. Conversely, complicated UTIs occur in a urinary tract that has metabolic, functional, or structural abnormalities [1]. Recurrent uncomplicated UTIs are common presentations to clinicians. Survey data suggest that 30% of women will have had a previously diagnosis and treatment of UTI by the age of 24 years, and more than half will be affected in their lifetime [2,3].
Recurrent UTIs are symptomatic UTIs that follow resolution of a previous event, usually after proper treatment [4].
Recurrent UTIs include relapses (i.e., symptomatic recurrent UTIs with the same organism following suitable
therapy) and reinfection (i.e., recurrent UTIs with previously isolated bacteria after treatment and with a negative interve- ning urine culture, or a recurrent UTI caused by a second bacterial isolate).
In most cases, UTIs develop when a common, normal organism of the genital area are substituted by pathologic bacteria that raise cystitis by ascending from urethra to bladder. The formation of bacteria is assumed to be caused by virulence factors that allow colonization by better adherence and spread of pathogens. The typical pathogens include Escherichia coli , Klebsiella pneumoniae , Proteus mirabilis , and Staphylococcus saprophyticus [5].
A threshold of 3 UTIs in twelve months is used to define recurrent UTI [6].
In the case of bacterial persistence, an identical bacterium
94 Hoon Choi and Jae Hyun Bae. Diagnosis of Recurrent UTI
Urogenit Tract Infect Vol. 11, No. 3, December 2016
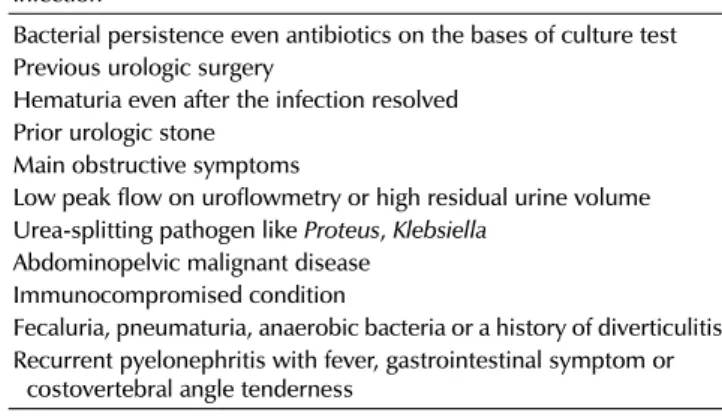
Table 1. Condition for further investigations of recurrent urinary tract infection
Bacterial persistence even antibiotics on the bases of culture test Previous urologic surgery
Hematuria even after the infection resolved Prior urologic stone
Main obstructive symptoms
Low peak flow on uroflowmetry or high residual urine volume Urea-splitting pathogen like Proteus, Klebsiella
Abdominopelvic malignant disease Immunocompromised condition
Fecaluria, pneumaturia, anaerobic bacteria or a history of diverticulitis Recurrent pyelonephritis with fever, gastrointestinal symptom or
costovertebral angle tenderness
is cultured within two weeks after the first sensitivity-based antibiotics. Reinfection is caused by a repeated infection of different organism, or the identical organism after more than 2 weeks of treatment [7].
Even urine culture is one of the representative tools to identify recurrent uncomplicated UTI, and clinical judgment should be grounded in the results of urine dipstick and microscopy with symptomatic signs.
CLINICAL ASPECT
Documentation of symptoms and responses to treatment should be performed in patients suspected of UTI. Common symptoms include frequency, urgency, nocturia, and dysuria, and additionally, hematuria, back pain, costovertebral angle tenderness, and vaginal discharge or irritation. Regardless of urine culture positivity, self-diagnosis of UTI is also possible in patients who can sense the progress of infectious process by visible symptoms [8,9].
Features that affect the recurrence of uncomplicated UTI include the use of spermicides menopause, sexual activity, current antimicrobial use, and family history [10,11].
The history taking and physical examination should be performed. Physical examination, including pelvic examination, should also be applied to rule out functional or structural anomalies of the urinary tract [12].
In addition, uroflowmetry with postvoid residual urine are possible tests. By review of 149 postmenopausal women with recurrent uncomplicated UTI, the amount of postvoid residual urine was higher in women with recurrent UTIs than in women without a history of UTI (control patients) (23% vs. 2%). Moreover, the proportion of patients with reduced maximal flow rates are more likely to have recurrent uncomplicated UTI (45%) than those without a history of UTI (23%). Other previous studies did not report any significant differences in the residual urine volume and maximal flow rates between those with recurrent UTI and those without UTI [13,14].
The most powerful factor that warrant an investigation of UTIs is the rate of sexual contact in young women (18-30 years old) [4]. In fact, no evidence was made between recurrent UTIs and before voiding peri-coital patterns, method of wiping genital area, dressing tight underwears, urinary frequency, or interruption of voiding [2].
One controlled trial of aged women reported that
circumstances around bladder emptying, like postvoiding residual urine, incontinence, and cystocele, showed a strong correlation with recurrent UTIs [7].
An increase of residual urinary volume of more than 50 ml after voiding has been shown as an independent risk factor for recurrent UTIs in a previous study [1].
INVESTIGATIONS
It is important to double check the urine culture and sensitivity test for patients with symptomatic condition to find an appropriate antibiotic that best suppresses the causative pathogens. This process confirms recurrent UTI as the origin of the present lower urinary tract symptoms.
Moreover, modification of empirical antibiotics based on their bacterial sensitivity could eliminate the pathogens and prevent the development of resistant bacterial strains as a source for persistent UTI. For the midstream specimen of the voided urine, bacterial count of 1×10
5colony- forming units/L could be regarded as a positive urine culture, even in patients with mild symptoms [9]. A cautious assessment of midstream urine is needed due to the risk of contagion; and even with a negative urine culture result, there is a minor portion of patients who are responsive to antibiotic treatments [15]. If a urine culture showed no pathogen and minimal response to drugs, these may connote another disease. Then subjects could be re-cultured after 1 to 2 weeks following the initial therapy based on the sensitivity test to rule out bacterial persistence.
With respect to the cystoscopic examination, most studies
have revealed a relatively low incidence of structural
anomalies (from 0% to 15%) for recurrent UTI [16]. By
this low probability of positive findings on cystoscopy,
Hoon Choi and Jae Hyun Bae. Diagnosis of Recurrent UTIs 95
Urogenit Tract Infect Vol. 11, No. 3, December 2016
performing a cystoscope on all women presenting recurrent uncomplicated UTI seems ineffective. According to previous studies, a factor analysis for abnormal cystoscopic findings suggested complicated UTIs; however, the number of studies regarding this is too small to be conclusive [17,18].
Furthermore, performing an imaging study on all patients with recurrent UTI seems unnecessary due to the low possibility of complicated UTIs. A number of data revealed a low portion of non-incidental outcomes by a diagnostic approach by imaging modalities; therefore, these are not routinely recommended for recurrent UTI according to the guidelines, including the European Association of Urology guidelines [19,20].
Table 1 lists the cases of abnormalities with high suspicion;
and in these instances, a computed tomography of the abdomen and pelvis would be a suitable imaging method for further investigation to rule out complicated UTIs [21].
To minimize radiation exposure, ultrasound imaging in the urinary tract with an additional plain X-ray is also recommendable [22-24].
It is true that there are no definite indications for imaging in patients who have recurrent UTIs, but rational indications for imaging to exclude specific causes of recurrent are listed in Table 1.
In general, patients with recurrent uncomplicated UTI could be managed effectively by primary care physicians, regardless of specialty [25]. Referral to an infection specialist for recurrent uncomplicated UTI is warranted when risk factors for complicated UTI exist. Moreover, referral is necessary if the only way to correct the cause of UTI is through surgical intervention and if patients have recurrent lower urinary tract symptoms with uncertain origin. Prior to referral, urine culture while symptomatic and 2 weeks after sensitivity based antibiotics may help in confirming UTI, as well as guiding additional assessment and management by the specialist.
CONCLUSIONS
Urine culture and further analysis alone are not sufficient to diagnose recurrent UTI. A careful review of risk factors for complicated UTIs and optional uroflowmetry or imaging tests are needed. Defining the values of promising diagnostic tools could facilitate a development of new diagnostic tools and treatment of recurrent UTI.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Dason S, Dason JT, Kapoor A. Guidelines for the diagnosis and management of recurrent urinary tract infection in women. Can Urol Assoc J 2011;5:316-22.
2. Foxman B, Barlow R, D'Arcy H, Gillespie B, Sobel JD. Urinary tract infection: self-reported incidence and associated costs.
Ann Epidemiol 2000;10:509-15.
3. Foxman B. Recurring urinary tract infection: incidence and risk factors. Am J Public Health 1990;80:331-3.
4. Hooton TM. Recurrent urinary tract infection in women. Int J Antimicrob Agents 2001;17:259-68.
5. Echols RM, Tosiello RL, Haverstock DC, Tice AD. Demographic, clinical, and treatment parameters influencing the outcome of acute cystitis. Clin Infect Dis 1999;29:113-9.
6. Epp A, Larochelle A, Lovatsis D, Walter JE, Easton W, Farrell SA, et al. Recurrent urinary tract infection. J Obstet Gynaecol Can 2010;32:1082-101.
7. Hooton TM. Recurrent urinary tract infection in women [Internet]. Wolters Kluwer Health; 2011 [cited 2011 Sep 21].
Available from: http://www.uptodate.com/contents/recurrent- urinary-tract-infection-in-women.
8. Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this woman have an acute uncomplicated urinary tract infection?
JAMA 2002;287:2701-10.
9. Giesen LG, Cousins G, Dimitrov BD, van de Laar FA, Fahey T.
Predicting acute uncomplicated urinary tract infection in women: a systematic review of the diagnostic accuracy of symptoms and signs. BMC Fam Pract 2010;11:78.
10. Dielubanza EJ, Schaeffer AJ. Urinary tract infections in women.
Med Clin North Am 2011;95:27-41.
11. Hooton TM, Scholes D, Hughes JP, Winter C, Roberts PL, Stapleton AE, et al. A prospective study of risk factors for symptomatic urinary tract infection in young women. N Engl J Med 1996;335:468-74.
12. Neal DE Jr. Complicated urinary tract infections. Urol Clin North Am 2008;35:13-22.
13. Raz R, Gennesin Y, Wasser J, Stoler Z, Rosenfeld S, Rottensterich E, et al. Recurrent urinary tract infections in postmenopausal women. Clin Infect Dis 2000;30:152-6.
14. Hooton TM, Stapleton AE, Roberts PL, Winter C, Scholes D, Bavendam T, et al. Perineal anatomy and urine-voiding characteristics of young women with and without recurrent urinary tract infections. Clin Infect Dis 1999;29:1600-1.
15. Nicolle LE. Uncomplicated urinary tract infection in adults including uncomplicated pyelonephritis. Urol Clin North Am
96 Hoon Choi and Jae Hyun Bae. Diagnosis of Recurrent UTI
Urogenit Tract Infect Vol. 11, No. 3, December 2016 2008;35:1-12.
16. Lawrentschuk N, Ooi J, Pang A, Naidu KS, Bolton DM.
Cystoscopy in women with recurrent urinary tract infection. Int J Urol 2006;13:350-3.
17. van Haarst EP, van Andel G, Heldeweg EA, Schlatmann TJ, van der Horst HJ. Evaluation of the diagnostic workup in young women referred for recurrent lower urinary tract infections.
Urology 2001;57:1068-72.
18. Nickel JC, Wilson J, Morales A, Heaton J. Value of urologic investigation in a targeted group of women with recurrent urinary tract infections. Can J Surg 1991;34:591-4.
19. Engel G, Schaeffer AJ, Grayhack JT, Wendel EF. The role of excretory urography and cystoscopy in the evaluation and management of women with recurrent urinary tract infection. J Urol 1980;123:190-1.
20. Fowler JE Jr, Pulaski ET. Excretory urography, cystography, and cystoscopy in the evaluation of women with urinary-tract infection: a prospective study. N Engl J Med 1981;304:462-5.
21. Wollin T, Laroche B, Psooy K. Canadian guidelines for the
management of asymptomatic microscopic hematuria in adults. Can Urol Assoc J 2009;3:77-80.
22. Spencer J, Lindsell D, Mastorakou I. Ultrasonography compared with intravenous urography in investigation of urinary tract infection in adults. BMJ 1990;301:221-4.
23. Andrews SJ, Brooks PT, Hanbury DC, King CM, Prendergast CM, Boustead GB, et al. Ultrasonography and abdominal radiography versus intravenous urography in investigation of urinary tract infection in men: prospective incident cohort study. BMJ 2002;324:454-6.
24. McNicholas MM, Griffin JF, Cantwell DF. Ultrasound of the pelvis and renal tract combined with a plain film of abdomen in young women with urinary tract infection: can it replace intravenous urography? A prospective study. Br J Radiol 1991;64:221-4.
25. Kodner CM, Thomas Gupton EK. Recurrent urinary tract infections in women: diagnosis and management. Am Fam Physician 2010;82:638-43.