대 한 방사 선 의 학회 지 1996: 34(5) : 633- 639
우하복부 동통을 동반한 종괴 :초음파 빛 CT 소견 1
남궁숙·임효근·이원재·김태호 · 이순진·임재훈
돔통을 동반하는 우하복부 종괴의 원인으로는 천공성 충수돌기염, 대장의 악성 종앙, 게실염, 결핵성 장염, 기타 장중첩증, 난소 종앙 등이 있으며, 이들의 정확한 감별 진단은 치료 방침의 결정 및 예후 판 정에중요하다.
이 화보에서는 각 질환의 초음파와 CT 소견을 비교하여 각각의 특징이 되는 소견과 감별점을 기술 하고자하였다.
서
론
동통을동반한우하복부종괴의 원인에는천공성 충수돌 기염, 대장의 악성 종양, 게실염이나 결핵성 장염과 같은 염증성 장질환, 장중첩증, 그 외 여성의 경우 난소 종양 등 이 있다. 이들 질환의 임상 증상은 우하복부 동통, 오성, 구 토, 설사 등으로 비특이적이며, 경우에 따라 응급 수술 여 부 결정이 환자의 치료 및 예후에 영향을 미칠 수 있으므로 방사선학적인 정확한 감별 진단이 중요하다. 이들 진단에 는 주로 대장 조영술과
CT
검사가 이용되어 왔고, 최근에 는 초음파 기기의 발달로 위장관 질환의 진단에 많은 발전 을 이루었 3며 응급 검사로서의 유용성이 보고되고 있다 (1,2) .
본화보에서는동통을동반한우하복부총괴의 초음파와
CT
소견을 비교하고 특정적 인 소견과 감별점을 중심으로 기술하고자한다.천공성층수돌기염
급성 충수돌기염이 진행되면 충수물기의 부종으로 업구 가 막히게 되고 충수돌기의 팽창, 허혈, 괴사가 진행되어 천공을 일으키게 된다. 이때 창간막과 같은 대장 주위의 지 방 조직이 천공 부위를 감싸게 되고, 좀더 진행하면 봉와직 염 (phlegmonous change) 을 거쳐 농양을 형성하게 된다.
천공성 충수돌기역의 방사선학적 진단은 맹장 주위의 국소 화된 액체 저류와 봉와직염으로 형성된 종괴 내부에서 충 수 결석 이나 10mm이상 커진 괴 사성 충수돌기를 찾음으로 써 가능하고 (Fig. 1a-c), 충수돌기나 결석을 찾지 못하는
l삼성서울병원 진 단방사선과학교실
이 논문은 1996 년 2월 12일 접수하여 1996 년 6월 13일에 채택되었음
경우에는 대장암 천공이나 다른 원인의 염증성 장질환에 의한농양과감별이 어렵다(1, 3). 충수돌기의 끝이 골반강 깊숙이 위치하는 경우 초음파로 끝부분을 추적하기 어려 운 경우가 있으며, 간흑 충수돌기의 전반부는 정상이면서 염증이 끝부분에 국한되어 천공을 일으켜 골반강 농양을 형성하는 경우가 있는데정상적인 크기를 보이는 전반부를 추적하여 염증을 일으킨 충수돌기의 끝부분과 골반강 농 양의 연관성을 관찰함으로써 진단할 수 있다 (Fig. 2a-c).
충수돌기가 터지고 농양을 형성하기 전의 봉와직염 상태 에서, CT에서는충수돌기나봉와직염에 의한종괴 모두가 조영 증강을 보이므로 충수돌기 자체를 찾기가 어렵고 종 괴 양상이 악성 종양과 유사한 형태로 보일 수가 있는데
(3) , 초음파 검사에서는 봉와직엽은 고에코의 종괴로 보이
고 염증을 일으킨 충수돌기는 비교적 저에코의 관상 형태 를 보이므로 조직 대조도가 우수하여 진단에 도움을 줄 수 있다 (Fig. 3a
,
b).대장의악성종양
맹장암을 포함한 우측 대장암은 장관 내부로 자라는 폴 립양종괴,혹은동성성 또는편측성의 불규칙한장관벽 두 께 증가의 형태를 보인다 (4). 폴립양 종괴의 경우 경계가 분명한 고형 종괴로 보이므로 (Fig. 4a, b) 방사선학적으로 쉽게 진단이 가능하나, 장관벽 두께 증가를 보이는 경우는 염증성 장질환에 의한 벽두께 증가와 감별하여야 한다. 대 장암의 경우 벽두께 증가가 암세포의 침윤으로 인하여 생 기므로 초음파 검사나 CT상 벽층들이 소설되는 반면 (Fig. 5a, b), 염증성 장질환에 의한 벽두께 증가는 주로 점막하 층의 부종에 의하여 생기므로 벽층들이 구분되어 보이므 로 (Fig. 1a, 7a, 7c), 벽층 소설 여부가 두 질환의 감별에 유 용한 지표가 될 수 있다. 우측 대장암의 흔한 합병증으로 천공이 있으며 농양 형성으로 언하여 종괴 흑은 벽두께 증 - 633-
대 한 방 사 선 의 학 회 지 1996: 34( 5) : 633-639
a b c
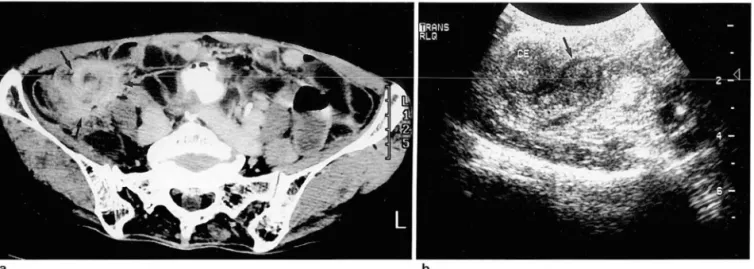
Fig. 1 . Perforated appendicitis
a. Transverse sonogram shows a target-like enlarged appendix(between electronic calipers) within an inflammatory mass (arrows)
b. Transverse sonogram shows an echogenic appendic이 ith(arrow) casting strong posterior shadowing within an echogenic in- flammatory mass(open arrows)‘
c. CT scan at the level of the cecum(ce) shows a large pericecal abscess(arrowheads) with remnant enlarged appendix(arrow).
a
Fig. 2. Pelvic abscess with perforation of appendiceal ti P porti on
a. Transverse sonogram shows normal mid-portion(1) of the appendix with pre served wall layering, and enlarged appen dix(2) with destroyed layering at the tip portion(ia, iv: iliac artery and vein) b. Transverse sonogram shows a large pelvic abscess
c. CT scan at the level of the cecal tip shows relationship between pelvic ab- scess and enlarged appendix with con trast enhancement(arrow)‘
c
가를정확히 분석하기 온란하여 천공성 충수돌기나 염증성 장질환에 의한농양과의 감별이 어려울수있다.대장암천 공의 경우, CT상 앓은 선상의 조영 증강을 보이는 농양벽 과 구별되는 분엽상의 종괴 자체를 찾아냄으로써 진단할 수 있고, 초음파 검사에서는 우상복부로부터의 추적 검사 시 장관과 연결되고 농양과 인접한 분엽상의 종괴 또는 벽 두께 증가를 찾음으로써 진단할 수 있다 (Fig. 8a, b).
a
Fig. 3. Perlorated appendicitis with pericecal phlegmon
남궁숙 오1: 우하복부 동통을 동반한 종괴
게실염
게실엽은 병리적으로 장관 평활근의 비후 소견을 보이며 이와 동반된 연축 (spasm) , 부종 등에 의하여 미만성의 장 관벽 두께 증가를 일으키게 된다 (2). 특정적으로 미만성으 로 두꺼워진 장관벽과 분변 혹은 공기를 함유한 게실 자체 를 찾음으로써 방사선학적 진단을 할 수 있고 (Fig. 6a-d) 다른 염증성 장질환에 의한 벽두께 증가와의 감별점이 될 수 있다 (2, 5).
b
a. CT scan at the level 01 the cecum shows a spiculated and heterogeneously enhanced mass(arrows) with no clearly delined appendix
b. Transverse sonogram shows markedly enlarged hypoechoic appendix(arrow) arising lrom the cecal tip(CE), and surrounding echogenic phlegmon
a
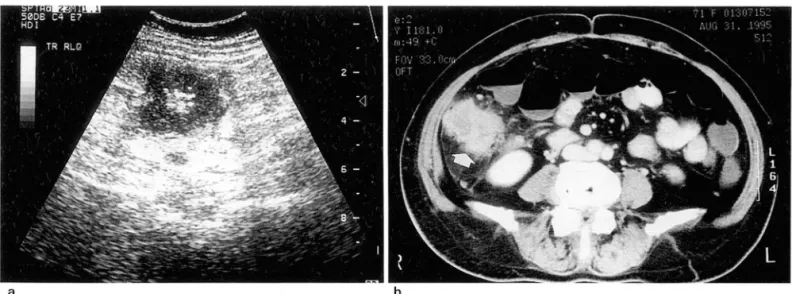
Fig. 4. Polypoid cecal cancer
a. Transverse sonogram 01 the cecum shows a well demarcated and lobulated hypoechoic mass with no evidence 01 bowel wall thickening
b. CT scan at the level 01 the cecum shows a lobulated intralu- minal p이 yp이 d mass(arrow) without cecal wall thickening
- 635
대 한 방 사 선 의 학 회 지 1996 : 34( 5) : 633-639
a b
Fig. 5. Ascending colon cancer presenting as wall thickening
a. Transverse sonogram shows irregular and concentric wall thickening with destroyed wall layering
b. CT scan at the level 01 the ascending colon shows an irregular and heterogeneously enhanced mass(arrow) with concentric wall thickening and obliterated colonic lumen
c
Fig. 6. Diverticulitis
a. Longitudinal sonogram shows diffusely thickened wall 01 the ascending colon with preserved wall layering
b. Transverse sonogram at the level 01 the ascending colon shows concentric wall thickening(arrowheads), lecolith(arrow) within an inllammed diverticulum(curved arrows), and surrounding phlegmonous change(between electronic calipers).
c. CT scan at the level 01 the cecum shows multiple air-lilled diverticula(arrowheads) and surrounding phlegmonous change (arrows)
d. CT scan at the level 01 the ascending colon shows a lecolith(arrow) within an inllammed diverticulum and surrounding phleg- monous change(curved arrows)
α α
연관성을 추적함으로써 진단할 수 있다.
결핵성장염
결핵성 장염은 우리나라에서 흔한 염증성 장질환의 하나 로 크론씨 병이나 궤양성 장염같은 다른 만성 염증성 장질 환과의 감별이 중요하고, 임파절 종대를 흔히 동반하므로 엄파종 혹은 임프절 전이 등과 감별을 요할 때가 있다 (6).
초음파 검사에서는 주변 임프절 종대를 통반하고 회맹판을 포함한 말단 회장부에 벽층이 유지되는 미만성의 두께 증
a b
c
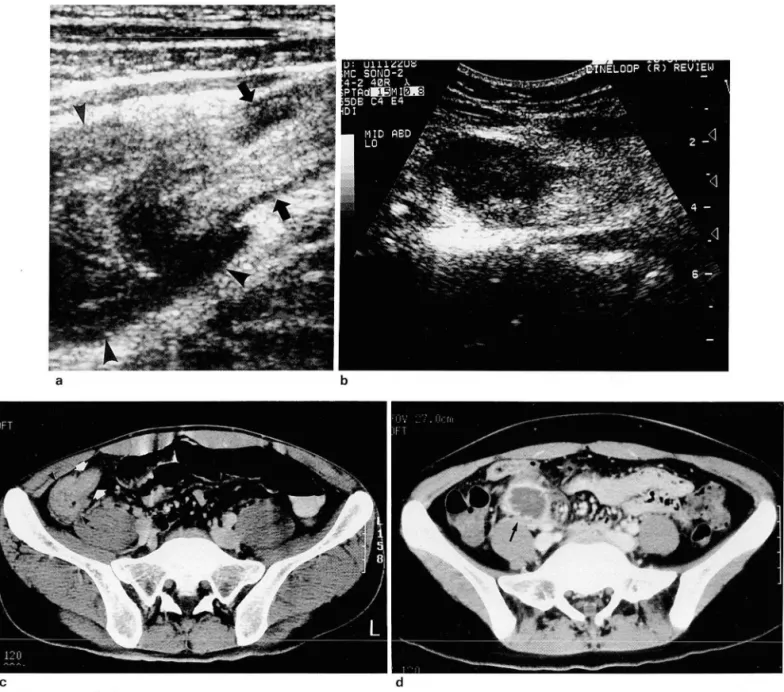
Fig. 7. Ileocecal(I-C) tuberculosis
d
남궁숙 외 · 우하복부 동통을 동반한 종괴
가를 보이는 경우 진단할 수 있고 (Fig. 7a, b), 뚜렷한 장관 벽의 두께 증가없이 수 cm까지 커지는 심한 임파절 종대를 보이는 경우 악성 임파절과의 감별이 어렵다. CT에서도 회맹판을 포함한 말단 회장부의 미만성 벽두께 증가와 주 변 임프절 종대를 보이고, 초음파 소견과는 달리 특징적으 로 앓은 테두리 조영 증강을 보이므로 악성 임파절과 쉽게 감별할 수 있다 (Fig. 7c, d).
a. Transverse sonogram shows dilluse wall thickening 01 the terminal ileum(arrows) and cecum(arrowheads). Notice preserved layering pattern 01 the cecum and terminal ileum.
b. Another transverse sonogram shows an enlarged hypoechoic mesenteric Iymph node
c. CT scan at the level 01 the I-C valve shows diffuse and even wall thickening 01 the cecum(arrowheads) and terminal ileum (arrows). Again layering pattern 01 the wall is preserved
d. CT scan 2-cm caudal to Fig. 7-c shows a markedly enlarged hypodense Iymph node with peripheral rim enhancement(arrow) that is characteristic linding 01 the tuberculous Iymphadenopathy
-637 -
대 한 방사섣 의 학회 지 1996: 34(5) : 633-639
a b
Fig. 8. Perforated cecal cancer
a. CT scan at the level of the cecum shows eccentric and lobulated enhancing mass lesions(arrows) and abscess formation (arrowheads) with interruption of the bowel wall pattern.
b. Oblique longitudinal sonogram shows lobulated wall thickening of the cecum(curved arrows) and pericecal abscess(ar- rowheads). Secondary enlargement of the appendix is also demonstrated(arrow)
a b
Fig. 9. Intussusception
a. Transverse sonogram of right lower abdomen shows a doughnut shaped slightly echogenic mass with surrounding hypoechoic area. Right half of the doughnut shape is obscured by reverbration artifact resulting from intraluminal gas(arrowheads)
b. CT scan shows an onion-peel like mass representing an intussusception(arrows)‘
a b
Fig. 10. Krukenberg tumor
a. Transverse sonogram of right lower abdomen shows a lobulated hypoechoic solid mass lesion(between electronic calipers) adjacent to the uterus(U)
b. CT scan at the level of the acetabulum shows a homogeneously enhanced and lobulated solid mass(arrows) that is an- terolateral to the uterus. The patient has a proven gastric carcinoma
기 타
장중첩증, 난소 종양 등이 우하복부 동통을 통반한 종괴 로 나타날 수 있고, 장중첩증의 경우 도우넷 모양, 양파 껍 질 모양 등의 특징적인 소견을 보이며 (Fig. 9a
,
b),
난소 종양은 낭성 흑은 고형 종괴로 보이고(Fig. lOa
,
b) 자궁과의 연관성을추적함으로써 진단할수있다.jξL = 고 ~ C그 ~ 헌
1. Borushok KF, Jeffrey Jr. RB, Laing FC, Townsend RR. Sono- graphic Diagnosis of Perforation in Patients with Acute Ap-
남궁숙 오1: 우하복부 동통을 동반한 종괴
pendicitis. AJR 1990; 154: 275-278
2. Wilson SR, Toi A. The Value of Sonography in the Diagnosis
。fAcute Diverticulitis of the Colon. AJR 1990;154:1199-1202 3 강현일, 강경옥, 서명옥 등 충수주위 농앙의 전산화단층촬영 소견
대한방사선의학회지 1987; 23 : 277.282
4. Keeney G, Jafri SZ, Mezwa DG. Computed Tomographic Evaluation and Staging of Cecal Carcinoma. Gastrointest Radiol 1989; 14 : 65-69
5. Scatarige JC, Fishman EK, Crist DW, Cameron JL, Siegelman SS. Diverticulitis of the Right Colon: CT Observations. AJR 1987; 148: 737-739
6. Balthazar EJ, Gordon R, Hulnick D. lIeocecal Tuberculosis:
CT and Radiologic Evaluations. AJR 1990; 154 : 499-503
Journal of the Korean Radiological Society 1996; 34(5) : 633-639
The Tender Masses in Right lower Abdomen:
Ultrasonographic and CT Features'
500k Namkung,
M.D
, Hyo Keun Lim,M.D
, Won Jae lee,M.D
, Tae Ho Kim,M.D
, 500n Jin lee,M.D
, Jae Hoon Lim,M.D.
IDepartment of Diagnostic Radiology, Samsung Medical Center
Perforated appendicitis with an abscess formation is known to be the most common cause of tender mass in right lower abdomen. The differential diagnosis of a tender mass in right lower abdomen, however, is broad and includes various intraabdominal and intrapelvic lesions in origin. Preoperative accurate diagnosis is essen- tial in order to avoid unnecessary surgery or complications resulting from delayed surgery. The purpose of this pictorial essay is to illustrate examples of various causes and methods to differentiate them with ultrasono- graphy and CT.
Index Words: Gastrointestinal tract, US Neoplasms, CT
Abdomen, abscess
Address reprint requests to : Sook Namkung, M.D., Department of Diagnostic Radiology, Hallym University Hospital.
" 153 Kyo-Dong, Chuncheon, Gangwon-Do 200-060 Korea.
Tel. 82-361-52-9970(1 58) Fax.82-361-55-6244
%
핵의한과 전문의 자격 취득 앞내
1 써써 γ! ~ 1.:π&했앙당1싸인 (상싼
신설과목인 핵의학과 전문의 자격 취득에 있어서 1 차시험 면제의 규정이 1999년 종 료됨에 따라 1차시험을 면제받는 방법과 요령을 아래와 같이 안내하오니 적극 참여하 시어 자격을 취득할 수 있도록 바랍니다.
-아 래
1.
1 차시험 자격요건1) 핵의학전문분야가설치되어 있는종합병원급이상의 의료기관에서 4년이상실무 또는 연구업무에 종사한 의사(외국에서 동일기간 이상 실무 또는 연구엽무 종사 자포함)
@ 내과, 진단방사선과, 임상병리과 전문의 자격취득자에 대하여 2년의 실무 또는 연구업무 종사경력을 인정함.
@ 기타다른전문의 자격 취득자에 대하여 1년의 실무또는연구엽무종사경력을 인정함.
2)
위 1)항 해당자로서 학회가 인정한 점수가 60점 이상인 자 3) 점수산정 방법@
최근 3년 이내에 대한핵의학회 참석빈도 점수 30점 5회이상25점 4회 20점 3회 15점 2회 10점 1 회
@핵의학관련논문의 저자점수(제 1 저자가아니어도무방) 30점 3편이상
20점 2편 10점 1 편
@ 대한핵의학회 발표연제 점수(제 1 저자가아니어도무방) 20점 3편이상
15점 2편 10점 1 편
@기타
20점 방사선 동위원소 취급 특수면허 소지자
2.1 차시험 면제요건
1) 외국에서 핵의학 전문의 자격을 취득한 자
2)
영제 17조 제 1 항 제 3호에 해당된 자로서 국내외 의과대학, 수련병원 또는 수련기 관에서 핵의학관련 분야에 4년이상의 교육또는수련지도경력이 있는자(단, 학회가 인정한 점수가 60점 이상인 자)