서 론
후골간신경 증후군은 상지에서 발생하는 말초신경 압박 증후군 중 0.7%이하에서 보고되는 드문 질환으로 외상, 공 간 점유 병소, 염증성 변화 등 여러 가지 원인에 의해 발생한 다.1,2 가장 흔한 원인은 골절이나 탈구 등의 외상으로 알려 져 있고, 15%정도는 의원성 원인에 의해 발생하는 것으로
보고된다.3,4 어깨 관절경 후 신경 손상이 발생하는 경우는 드물지만 Sisco 등5이 어깨 관절경 수술 후 발생한 전골간신 경 증후군 3예를 보고한 바 있고, 이후 Pope 등6과 Desliva 등7이 각각 4예와 3예를 보고하기도 했다. 국내에서도 어깨 관절경 수술 후 전골간과 후골간신경 증후군이 동시에 발생 한 예를 보고한 바 있다.8 본 증례에서는 어깨 관절경 수술 후 후골간신경 증후군이 발생하였고, 보존적 치료에도 호전 되지 않아 신경박리술을 시행하였다. 이에 저자들은 본 증례 를 통해 어깨 관절경 수술과 관련하여 발생한 후골간신경 증 후군의 발생 기전과 경과에 대해 문헌 고찰과 함께 보고하고 자 한다.
어깨 관절경 후 발생한 후골간신경 증후군 -증례보고-
김은진, 김경은
국군수도병원 재활의학과
Posterior Interosseous Nerve Syndrome following Shoulder Arthroscopy -A Case Report-
Eun Jin Kim, Kyoung-Eun Kim
Department of Physical Medicine and Rehabilitation, The Armed Forces Capital Hospital, Seongnam, Korea
Received October 4, 2016
Revised (1st) November 3, 2016, (2nd) December 20, 2016, (3rd) January 15, 2017 Accepted January 18, 2017
Corresponding Author: Eun Jin Kim
Department of Physical Medicine and Rehabilitation, The Armed Forces Capital Hospital, 81 Saemaeul-ro 117beon-gil, Bundang-gu, Seongnam 13574, Korea
Tel: 82-31-725-6325, Fax: 82-31-705-6469, E-mail: [email protected]
Shoulder arthroscopy was performed on a 20-year-old male patient with left shoulder instability. In right lateral decubitus position and under general anesthesia, traction was applied for 2 hours to the elbow in extension. Nine days after the surgery, the patient complained of weakness of the extensor muscles of the left fingers. There was left posterior interosseous neuropathy with electrophyisiologic and imaging study. The neurologic deficit persisted for three months and neurolysis was performed on the posterior interosseous nerve. Seven months after neurolysis, the extension power of the fingers did not fully recover. Posterior interosseous nerve syndrome following shoulder arthroscopy might occur probably due to the traction and the position of the patient during the procedure.
Key Words: shoulder, posterior interosseous nerve, arthroscopy
Copyright © by Korean Association of EMG Electrodiagnostic Medicine
This is an Open Ac cess article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ISSN 1229-6066 https://doi.org/10.18214/jkaem.2017.19.1.19 J Korean Assoc EMG Electrodiagn Med 19(1):19-23, 2017
J Korean Assoc
Electrodiagn Med EMG
증 례
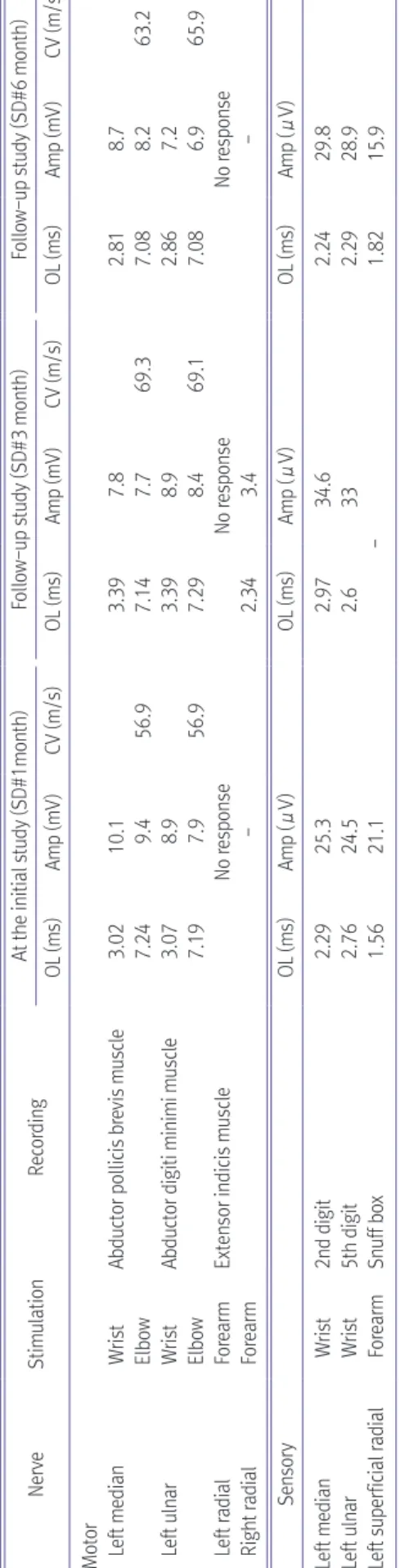
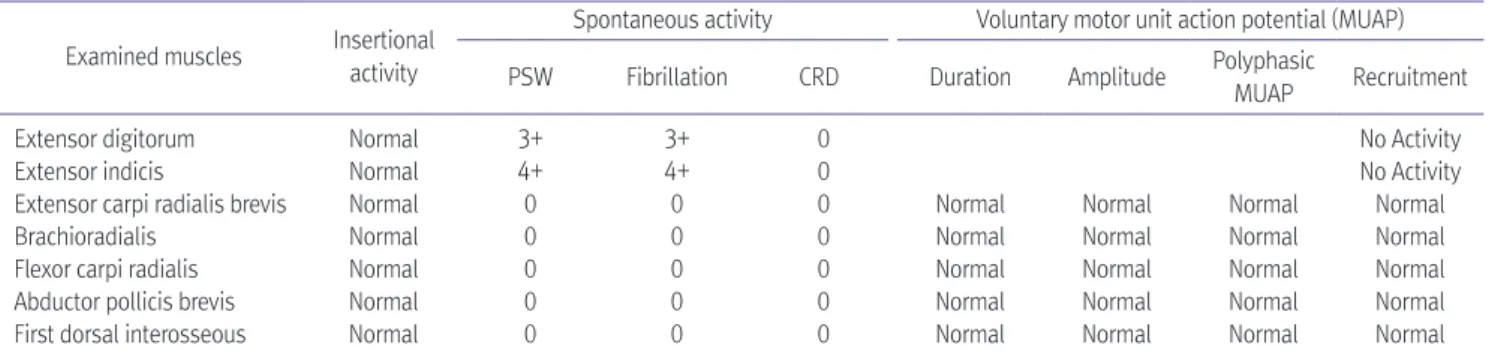
20세 남자가 좌측 어깨 관절의 불안정성을 주소로 본원 정형외과에 입원하였다. 환자는 중학교 시절부터 양측 어 깨가 자주 탈구되었고, 최근 어깨 탈구의 빈도가 증가하는 추세였으며, 좌측 어깨 관절의 관절조영 자기공명영상검사 (magnetic resonance arthrogram)를 시행한 결과 방카르 트병변과 힐삭스병변이 발견되어 수술적 치료를 시행하였 다. 환자는 전신마취 상태에서 우측 측와위 자세로 좌측 주 관절은 신전한 상태에서 압박 붕대를 전완부에 감은 후 접착 성 팔걸이를 상지에 착용시켜 3.5 kg의 무게로 견인을 하여 어깨 관절경 수술을 시행하였다(Fig. 1). 방카르트술식을 시 행하였고 수술 시간은 약 2시간이 소요되었으며 수술 중 특 이 소견은 없었다. 환자는 수술 후 좌측 전완부 근위부 동통 을 호소하였고, 수술 후 9일째부터 수부의 근력 저하를 호 소하였다. 이학적 검사에서 수지 신전 근력이 저하되어 있 고, 상지 감각은 정상이었다. 증상이 시작된 지 한 달 후 시 행한 신경생리학적 검사 결과에서는 신경전도검사 중 감각 신경에서 좌측 천요골신경은 정상 소견을 보였고, 운동신경 에서 인지신근에서 기록하고 손목에서 자극했을 때 좌측 요 골신경검사에서 복합운동전위가 유발되지 않았으며, 침근 전도 검사에서는 좌측 수지신근과 인지신근 등의 근육에서 대량의 비정상 자발전위가 관찰되면서 운동단위유발전위가 관찰되지 않았다(Table 1, 2). 후골간신경 증후군 진단 하에 전완부의 자기공명영상검사를 시행하였고, T2 강조 영상에
Table 1. Serial Findings of Nerve Conduction Studies NerveStimulationRecordingAt the initial study (SD#1month)Follow-up study (SD#3 month)Follow-up study (SD#6 month) OL (ms)Amp (mV)CV (m/s)OL (ms)Amp (mV)CV (m/s)OL (ms)Amp (mV)CV (m/s) Motor Left medianWristAbductor pollicis brevis muscle3.0210.13.397.82.818.7 Elbow7.249.456.97.147.769.37.088.263.2 Left ulnarWristAbductor digiti minimi muscle3.078.93.398.92.867.2 Elbow7.197.956.97.298.469.17.086.965.9 Left radialForearmExtensor indicis muscleNo responseNo responseNo response Right radialForearm-2.343.4- SensoryOL (ms)Amp (μV)OL (ms)Amp (μV)OL (ms)Amp (μV) Left medianWrist2nd digit2.2925.32.9734.62.2429.8 Left ulnarWrist5th digit2.7624.52.6332.2928.9 Left superficial radialForearmSnuff box1.5621.1-1.8215.9 SD: day after symptom developed, OL: Onset latency, Amp: Amplitude, CV: Condution velocity Fig. 1. The use of adhesive foam sling on the forearm with compres-
sive bandage during shoulder arthroscopic surgery.
서 회외근, 지신근, 척수근신근과 장무지외전근 등에서 고강 도 신호 소견을 보였으나, 후골간신경은 특이 이상소견을 보 이지 않았다(Fig. 2). 보존적 치료를 시행하며 경과 관찰하였 으나, 증상 발현 후 3개월 시점에도 증상의 회복이 없어 후 골간신경에 대한 신경탐색술을 계획하였다. 주관절 부위부 터 하방으로 신경박리술을 시행하였고, 후골간신경 주위에 는 육안소견상 압박할 만한 구조물이나 신경섬유의 형태 변 화는 없었다. 신경박리술 전과 3개월 후에 시행한 신경생리 학적 검사의 추적 검사에서 큰 호전을 보이지 않았고, 신경 박리술을 시행한 뒤 7개월 후에도 손가락 신전 근력은 완전 히 회복되지는 않았다.
고 찰
후골간신경은 요골신경의 신경분지로, 주관절 외상과의 상부에서 천요골신경을 분지한 이후를 말하는데, 요골신경 은 경추 5번에서 흉추 1번 신경 섬유로 이루어진 상완신경 총의 후신경다발에서 분지되는 두 말단 신경 중 하나로 액와 부로부터 손목 및 손등까지 다양한 위치에서 여러 원인에 의 해 손상 받을 수 있는 신경이다. 후골간신경은 요골신경에서
분지되어 회외근의 기시부 사이를 지나 전완부의 신전구획 에 위치하여 신전근들의 운동기능을 지배하고, 전완부에서 후골간신경이 압박되는 두 가지 증후군은 요측굴 증후군과 후골간신경 증후군이다.9 요측굴 증후군은 요측굴을 구성하 는 전완부 근육에 의해 이차적으로 원위부 요골신경 혹은 후 골간신경이 자극받아 발생한다고 믿어왔으나 실제로 압박 되는 부위나 구조물에 대해서는 논란이 있다.
후골간신경 증후군은 임상적으로 위약이 주로 문제가 되 기 때문에 외측 근위부 전완부 통증을 주로 호소하여 외측 상과염과 감별이 필요한 요측굴 증후군과 구분되고, 요측굴 의 바깥쪽에서 후골간 신경이 압박되는 경우이기 때문에 주 로 중수수지관절에서의 수지와 무지의 신전력 저하를 호소 한다. 후골간신경 증후군은 감각 이상 없이 주로 단요수근 신근, 수지신근, 장무지외전근, 장 및 단무지신근, 인지신근, 소지신근의 근력 약화나 마비를 일으킨다. 침근전도 검사에 서도 장요수근신근을 제외한 전완부의 신전근에서 이상을 보일 수 있고, 후골간신경 증후군에서 자기공명영상의 유용 성은 이미 보고된 바 있다.10 특히, 공간점유 병소를 확인하 는데 도움이 되며 임상적 그리고 전기진단학적으로 확진이 어려운 경우에는 보완할 수 있는 검사법이다.
Table 2. Findings of Needle Electromyography of Left Upper Extremity Examined muscles Insertional
activity
Spontaneous activity Voluntary motor unit action potential (MUAP) PSW Fibrillation CRD Duration Amplitude Polyphasic
MUAP Recruitment
Extensor digitorum Normal 3+ 3+ 0 No Activity
Extensor indicis Normal 4+ 4+ 0 No Activity
Extensor carpi radialis brevis Normal 0 0 0 Normal Normal Normal Normal
Brachioradialis Normal 0 0 0 Normal Normal Normal Normal
Flexor carpi radialis Normal 0 0 0 Normal Normal Normal Normal
Abductor pollicis brevis Normal 0 0 0 Normal Normal Normal Normal
First dorsal interosseous Normal 0 0 0 Normal Normal Normal Normal
PSW: positive sharp wave, CRD: complex repetitive discharge
A B
Fig. 2. Left forearm magnetic resonance imaging of a case patient. (A) T2 weighted magnetic resonance imaging of axial section showed posterior interosseous nerve (white arrow) and (B) diffuse high signal intensity in posterior interosseous nerve innervated muscles (black arrow).
본 증례에서는 이학적 검사에서 장무지외전근, 인지신근
및 수지신근에서 근력 저하가 관찰되고, 신경생리학적 검사 에서 후골간신경 마비를 시사하는 소견이 관찰되며 자기공 명영상에서도 후골간신경의 지배를 받는 근육에서 이상 소 견을 보여 후골간신경 증후군으로 진단하였다. 저자들은 어 깨 관절경 수술 후에 전완부 근위부의 동통과 근력 약화가 시작되었기 때문에 후골간신경 증후군의 발생이 관절경 수 술과 연관 가능성이 높다고 판단했다. 자발적으로 발생한 후 골간신경 증후군의 경우 대부분 예후가 좋은 것으로 알려져 있지만, 어깨 관절경 후 발생한 신경 손상의 증례를 분석한 결과 11명 중 3명은 본 증례와 같이 1년 이상 경과한 시점에 도 증상이 지속되었다.
수술 중 술기 자체뿐만 아니라 마취나 출혈 방지를 위한 압박, 수술 중의 환자의 자세 등 여러 요인들이 신경병증의 원인이 될 수 있음은 이미 알려져 있고11,12 특히, Sisco 등5은 어깨 관절경 수술 후 발생한 신경 증후군의 원인으로 세 가 지를 언급하였다. 수술 전 시행한 사각근간 마취가 말초 신 경병증을 발생시킬 수 있고, 수술 중 어깨 내의 세척액이 혈 관 외로 유출되어 신경포착 증후군의 원인이 될 수 있다고 하였다. 뿐만 아니라 수술 중의 자세 및 견인과 같은 물리적 요인에 의해 신경병증이 발생할 가능성을 제시하였다.
Pope 등6은 보고한 4예의 환자 중 3예가 Beach chair position이였던 점으로 미루어 보아 세 가지 원인 중 세척액 의 유출에 비중을 두어 보고하였으나, Collins 등13은 상완부 의 견인에 의해 신경의 부분적 긴장을 높일 수 있다는 견해 를 제시한 바 있고, Rains 등14도 측와위 자세가 팔의 자세와 견인 때문에 상완신경총에 과도한 부하를 주게 되고, 이런 자세를 한 뒤 10%의 환자에서 일과성 감각이상 혹은 실제적 인 신경 손상이 발생한다고 보고하였다. Lundberg15는 상지 의 혈류 장애가 발생할 때 신경섬유 속사이의 부종이 발생 할 수 있음을 보고하였다. 섬유속 사이의 부종으로 인해 섬 유속의 뻣뻣함이 야기되어 주관절의 굴곡 등의 움직임에 의 해 쉽게 신경섬유속이 꼬일 수 있다. 이를 뒷받침할 수 있는 소견으로 어깨 관절경 후 발생한 전골간 및 후골간신경 증후 군 환자의 신경탐색술 결과 후골간신경에서 모래시계 모양 의 섬유속 협착을 관찰한 바 있다.8 이런 여러 기전으로 어깨 관절경 후 직접적인 손상 없이도 수술 술기나 상지의 견인 혹은 압박을 포함한 환자의 자세에 의한 신경 손상이 발생할 가능성을 설명할 수 있다.
본 증례에서는 전신 마취를 시행하여 부위 마취에 의한 합 병증이나 부분적 신경병증의 가능성이 없었고, 어깨 내 유입
액의 압력도 30 mmHg로 높지 않았으며 수술 후 주관절과 전완부에서 통증 외에는 상지의 부종이나 혈종 등 그 외 특 이 증상이 관찰되지 않아 유입액의 혈관 외 유출에 의한 압 박 가능성은 낮다고 판단했다. 환자는 우측 측와위 자세에서 주관절을 신전시킨 상태에서 전완부에 압박붕대를 감은 후 접착성 팔걸이를 장착하여 3.5 kg의 무게로 2시간 동안 견 인을 시행하였고, 견인을 하는 동안 압박 붕대 일부가 말려 서 압박되거나 접착성 팔걸이에 의해 주관절 근처가 압박되 었을 가능성이 있었으며, 이로 인해 부분적 혈류 장애를 초 래하여 신경병증이 발생하였을 가능성도 있다.
후골간신경 증후군이 비외상성으로 발생하는 경우는 드물 고, 수술 후에 발생하는 경우는 환자가 호소하는 주관절 부 위의 통증을 술 후 통증으로 오인할 수 있기 때문에 이를 간 과하여 지나칠 수 있다. 어깨 관절경 수술을 할 때 술기나 환 자의 자세로 인해 신경 손상이 발생할 가능성을 이해하고, 관련 증상들을 숙지하여야 어깨 관절경 후 환자가 근력 저하 혹은 감각 이상을 호소할 경우 신경생리학적 및 영상의학적 검사를 통해 조기에 진단할 수 있다. 저자들은 어깨 관절경 수술 후 발생한 비외상성 후골간신경 증후군을 경험하였기 에 문헌 고찰과 함께 보고하는 바이다.
References
1. Young C, Hudson A, Richards R: Operative treatment of palsy of the posterior interosseous nerve of the forearm. J Bone Joint Surg Am 1990: 72: 12151219
2. Hazani R, Engineer NJ, Mowlavi A, Neumeister M, Lee A, Wilhelmi BJ: Anatomic landmarks for the radial tunnel.
Eplasty 2008: 8: 377382
3. Monteiro E, Moura A, Barros F, Carvalho P: Lipoma causing a posterior interosseous nerve syndrome. European Journal of Plastic Surgery 2002: 25: 3537
4. Vreiling C, Robinson PH, Geertzen JHB: Posterior interos
seous nerve syndrome: literature review and report of 14 cases. European Journal of Plastic Surgery 1998: 21: 196202 5. Sisco M, Dumanian GA: Anterior interosseous nerve
syndrome following shoulder arthroscopy. A report of three cases. J Bone Joint Surg Am 2007: 89: 392395
6. Pope D, Wottowa C: Mixed neuropathy presenting clinically as an anterior interosseous nerve palsy following shoulder arthroscopy: a report of four cases. J Shoulder Elbow Surg 2016: 25: e1699e1703
7. Deslivia MF, Lee HJ, Lee S, Zhu B, Jeon IH: Anterior interosseous nerve syndrome after shoulder arthroscopy:
report of 3 cases. J Shoulder Elbow Surg 2016: 25: e348e352 8. Seo JS, Kim JH, Kang DH: Simultaneous anterior and
posterior interosseous nerve syndrome following shoulder arthroscopy in the lateral decubitus position case report .
Clinics in Shoulder and Elbow 2013: 16: 148152
9. Bevelaqua AC, Hayter CL, Feinberg JH, Rodeo SA: Posterior interosseous neuro pathy: electrodiagnostic evaluation. HSSJ 2012: 8: 184189
10. Han ZA, Shim JE, Kim HI, Choi JY: Nontraumatic spontaneous posterior interosseous nerve palsy: sonography and magnetic resonance imaging with electromyographic correlation a case report . J Korean EMG Electrodiagn Med 2013: 15: 4752
11. Parks BJ: Postoperative peripheral neuropathies. Surgery 1973: 74: 348357
12. Saidha S, Spillane J, Mullins G, McNamara B: Spectrum of peripheral neuropathies associated with surgical interventions; a neurophysiological assessment. Journal of Brachial Plexus and Peripheral Nerve Injury 2010: 5: 9 13. Collins DN, Weber ER: Anterior interosseous nerve avulsion.
Clin Orthop 1983: 181: 175178
14. Rains DD, Rooke AG, Wahl CJ: Pathomechanism and complications related to patient positioning and anesthesia during shoulder arthroscopy. Arthroscopy 2011: 27: 532541 15. Lundborg G: Commentary: hourglasslike fascicular nerve
compressions. J Hand Surg [Am] 2003: 28: 212214