123
A Case of Synovial Hemangioma of the Knee
Sung-Il Shin, M.D., Jung-Woo Kang, M.D. and Joo-Hyun Ahn, M.D.
Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital, Hallym University School of Medicine, Seoul, Korea
Received: March 9, 2011 Revised: April 12, 2011 Accepted: May 7, 2011
Corresponding author: Sung-Il Shin, M.D.
Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital Hallym University School of Medicine, 445 Gil-dong, Gangdong-gu, Seoul 134-701, Korea
TEL: 82-2-2224-2230, FAX: 82-2-489-4391 E-mail: [email protected]
We report an unusual case of a 17-years-old male with complaints of pain and swelling of the left knee for the last 3 years with limitation of movement. He presented with spontaneous hemarthrosis of the knee joint. Magnetic resonance imaging revealed an intra articular mass. Arthroscopic excision was performed and the histology was characteristic of synovial hemangioma. After 1 year, the patient was completely asymptomatic and showed no signs of recurrence.
Key Words: Knee, Synovial hemangioma, Arthroscopic excision
Synovial hemangioma is a benign tumor in a joint rarely occurring in children or young adults, charac- terized by local pain, tenderness, soft tissue swelling, movement restrictions and hemarthrosis occurring with- out trauma2). Due to its nonspecific symptoms, it is dif- ficult to diagnose, and thus treatment is delayed easily.
The authors excised a case of synovial hemangioma oc- curring in the knee joint through an arthroscopic oper- ation, obtained satisfactory results through follow-up, so make a report along with a literary review.
CASE REPORT
A male patient aged 17 came to the hospital with pain and swelling of left knee joint as his chief com- plaint which had slowly progressed since about 3 years
ago. He neither experienced any special trauma nor had drug use or special diseases. Before the visit, for 3 years, he got swelling occurred and went down 6 times totally when he had walked for a long time but didn’t receive any special treatment.
Physical examination findings showed a swelling in his left knee joint and infrolateral patella tenderness and a movable mass was palpated directly under the patella. The range of knee joint movement was limited approximately from 0o to 120o, he complained pain when flexed more than 120o. Hemarthrosis was observed in the joint aspiration. In simple radiographs, there was no special finding observed (Figs. 1-3), and no abnor- mal finding in laboratory tests including one for defect in the coagulation of blood. In an magnetic resonance imaging (MRI), between directly under the patella and outer thigh, there was a swelling with a diameter of about 30 mm, and in a T1-weighted image, similar to or slightly higher signal intensity than muscle appeared while in T2-weighted image, high signal intensity was shown. Overall, irregular shape appeared as lobation (Figs. 4, 5).
For the removal of lesions and the biopsy, surgical treatment was performed. Through the operation, we
대한슬관절학회지:제 23 권 제 2 호 2011
124 Volume 23, Number 2, June 2011
Fig. 1. Anteroposterior radiograph. No significant bony abnormality.
Fig. 2. Lateral radiograph. No significant bony abnormality.
Fig. 3. Merchant view. No significant bony abnormality.
Fig. 4. T1-weighted sagittal MR image shows mass, have the signal intensity similar to muscle.
checked whether there was any abnormality in the joint including meniscus using arthroscope under general an- esthesia, and in a arthroscopic finding through ante- romedial portal, a mass was attached to the infrapatella fat pad (Figs. 6, 7). After insertion of a probe, they were detached from the base and they were relatively easily separated and a complete excision was performed including partial synovial capsule.
The excised tissue was sized about 30 mm, with pete-
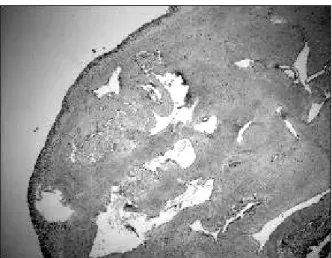
chial spots on the surface and reddish color overall due to the extended blood vessel. In the biopsy, a lot of blood vessels with a variety of size in the synovial tissue could be observed which could be diagnosed of synovial hemangioma (Figs. 8, 9).
As a result of 1 year follow-up after the operation, there were no knee joint pain & tenderness and a nor- mal range of knee joint movement, was shown after 3 months. The patient was satisfied and there was no
Fig. 5. T2-weighted sagittal MR image shows heterogenous high signal intensity mass including low signal intensity septa within the lesion.
Fig. 6. Arthroscopic view of synovial hemangioma.
Fig. 7. Arthroscopic view shows removal of synovial hemangioma.
Fig. 8. Microscopic finding shows several proliferation of vascular channel with synovial lining (H&E stain, ×40).
proof of relapse.
DISCUSSION
Synovial hemangiomas are rare causes of recurrent, non-specific joint complaints and take place most often in the knee joint. Till now, fewer than 200 cases have been reported in the world published reports. By defi- nition, a synovial hemangioma is a benign vascular le-
sion arising from any structure lined by synovium in- cluding the intra-articular region, bursal spaces and ten- don sheaths3).
Devaney et al.3) classified hemangioma into capillary, cavernous, mixed and venous; and out of all, cavernous hemangioma occurs most frequently (50%), followed by capillary hemangioma (25%), mixed hemangioma (20%), and venous hemangioma (5%). In 1939, Bennet and Cobey1) classified hemangioma morphologically into dif- fuse hemangioma and circumscribed hemangioma based
대한슬관절학회지:제 23 권 제 2 호 2011
126 Volume 23, Number 2, June 2011
Fig. 9. Microscopic finding shows thin walled vascular space of varying sizes lined with a single layer of endothelial cells (H&E stain, ×100).
on the 29 cases that had been reported. Diffuse he- mangioma is mostly cavernous, with intermittent pain and swelling: circumscribed hemangioma is capillary, and most of them are pedunculated. The case in this study can be considered to be diffuse hemangioma, which easily separates from surrounding synovial; histo- logically, it can be seen as capillary hemangioma.
Synovial hemangiomas mostly present as a non-trau- matic joint swelling combined with recurrent hemor- rhagic effusions in early childhood. Like this case re- ported, the symptoms usually persist for several years before the time of diagnosis. In most cases, a spongy compressible mass can be palpated over the joint, which decreases in size with elevation of the extremity4). According to Moon6), 75% of the symptoms are found in children under the age of 16; patient’s average age is 10.9 for girls and 12.5 for boys.
In regular radioactive examination, it may look like tumor-related phlebolithe, but it is not very useful in diagnosing the exact condition. Shapiro and Fanton10) stated the significance of adopting MRI in diagnosing the hemangioma in the joint. In case of synovial he- mangioma, the boundary is not clear on T1-weighted image, showing the same intensity in the muscle and high signal in the area with low blood flow; on
T2-weighted image, the boundary is clearer, with me- dium to high signal. MRI is not beneficial to all types of ailment in the knee joint, but it is useful when there is a mass on the joint or intermittent exudation from non-trauma; it helps distinguish the boundary in the joint as well as the condition of the joint. In the case study in this paper, we were able to identify the boun- dary of the mass by using MRI before operation, but on the T2-weighted image it showed low signal. This type of condition should be carefully distinguished from lo- calized pigmented villonodular synovitis that also shows low signal on MRI and T1/T2-weighted image. Paley and Jackson7) argued that arthroscopy is the best way to diagnose hemangioma in the knee joint and the final di- agnosis is made only on histopathology8).
The origin of synovial hemangiomas continues to be an enigma. Whether they merely represent late stages of post-traumatic lesion of are they true neoplastic vascular proliferations; is not yet clear.
Management of a case of synovial hemangioma de- pends on the anatomical distribution of the lesion.
Management of synovial hemangioma include open ex- cision, arthroscopic excision, embolization, and arthro- scopic excision by laser. Schechter9) reported a success in using radioactive therapy after wide excision. Moon6), however, considered excision by operation as the best way to treat the localized hemangioma and didn’t rec- ommend radioactive therapy for cases that can be surgi- cally treated. Meislin and Parisien5) reported that they had diagnosed synovial hemangioma by using arthro- scopy and successfully removed it by arthroscopic excision. Arthroscopic excision is carried out, if the le- sion is pedunculated and well-circumscribed. Diffuse le- sions are difficult to excise arthroscopically. For such cases, open wide excision is recommended. In Korea, such case has not been reported yet, and the use of ar- throscopy is limited in diffuse hemangioma. When syno- vial hemangioma in knee joint is local and easily re- moved, arthroscopic excision is recommendable.
슬관절에 발생한 활액막 혈관종
한림대학교 의과대학 강동성심병원 정형외과
신성일ㆍ강정우ㆍ안주현
17세 남자환자의 좌측 슬관절에, 관절부종과 운동제한을 동반한 활액막 혈관종의 증례를 보고한다. 환자 는 자발적 혈관절증이 발생하였고, MRI에서 관절내 종괴가 발견되었다. 슬관절경적 절제술 및 생검을 시행하였고, 조직학적 검사상 활액막 혈관종으로 판명되었다. 환자의 증상은 완전 호전되었고, 1년간 재발의 징후는 나타나지 않고 있다.
색인 단어: 슬관절, 활액막 혈관종, 관절경적 절제술 CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Bennet GE, Cobey MC: Hemangioma of joints: report of five cases. Arch Surg, 38; 487-500: 1939.
2. Boe S: Synovial hemangioma of the knee joint--a case report. Arthroscopy, 2; 178-180: 1986.
3. Devaney K, Vinh TN, Sweet DE: Synovial heman- gioma: a report of 20 cases with differential diagnostic considerations. Hum Pathol, 24; 737-745: 1993.
4. Enzinger FM, Weiss SW: Benign tumors and tumor- like lesions of blood vessels. In: Enzinger FM, Weiss WS ed. Soft tissue tumors. 2nd ed. St Louis, Mosby;
489-453: 1988.
5. Meislin RJ, Parisien JS: Arthroscopic excision of synovial hemangioma of the knee. Arthroscopy, 6;
64-67: 1990.
6. Moon NF: Synovial hemangioma of the knee joint. A review of previously reported cases and inclusion of two new cases. Clin Orthop Relat Res, (90); 183-190:
1973.
7. Paley D, Jackson RW: Synovial haemangioma of the knee joint: diagnosis by arthroscopy. Arthroscopy, 2;
174-177: 1986.
8. Rogalski R, Hensinger R, Loder R: Vascular abnor- malities of the extremities: clinical findings and manage- ment. J Pediatr Orthop, 13; 9-14: 1993.
9. Schechter DC: Intra-articular hemangioma of the knee.
Am Surg, 27; 638-641: 1961.
10. Shapiro GS, Fanton GS: Intraarticular hemangioma of the knee. Arthroscopy, 9; 464-466: 1993.