INTRODUCTION
Without doubt, allogenic blood transfusion has been an impor- tant lifesaving option in some circumstances. However, allogenic blood transfusion also has its drawbacks. Side effects of allogenic blood transfusion, blood scarcity and individual religion problem like Jehovah’s witnesses are major issues [1,2]. In this respect, there has been much effort to replace allogenic blood transfusion such as us- ing pharmacological agent, injecting topical vasoconstrictive agent, induced hypotension, intravenous iron, erythropoietin, coagulant and so on [3]. In addition, with growing technology, Cell salvage and Acute normovolemic hemodilution (ANH) has emerged as a substi- tute for allogenic blood transfusion [3,4]. First, Cell salvage became widely known in the late 1970s due to the infection threat like viral
hepatitis and HIV infection from allogenic blood transfusion [5].
Namely, it was introduced in an optimal time to the world. Even now, cell salvage is a useful and effective technique with a low risk of transfusion-borne infection. Second, ANH has been utilized and its efficacy studied since the 1960s [6,7]. ANH is also considered to be helpful in cutting back the volume of allogenic blood transfu- sion and transfusion of autologous whole blood [8]. Nonetheless, still the efficacy and utility of ANH and cell salvage is unclear with pros and cons due to inconsistent conditions among various articles and outcome from journals ranging from effectiveness to insignificance or being unthrifty when considering other facilities. Hence, through this study, we provide clinical information about procedures men- tioned above, gather various articles about cell salvage and ANH and make a conclusion whether cell salvage and ANH is effective or
Perioperative Blood Management: Pros and Cons of ANH and Cell Salvage
Sang Min Ahn1, Jong Hyun Lee2
1Department of Surgery, Hanyang University College of Medicine, Seoul, Korea
2Department of Anesthesiology and Pain Medicine, Sejong General Hospital, Bucheon, Korea Hanyang Med Rev 2018 Mar;38(1):27-37
https://doi.org/10.7599/hmr.2018.38.1.27 pISSN 1738-429X eISSN 2234-4446
Increasingly, autologous blood transfusion has been arousing concern owing to awareness of adverse effects of allogenic blood transfusion, blood shortage and patients, having religious or personal issues. With the development of medicine, Cell Salvage and Acute normovolemic hemodilution (ANH) has been proposed as an alternative to allogenic blood transfusion. This review looked at the use of ANH and cell salvage and evaluated the benefits and usefulness based on the strengths and indications. Although not consistent with all cases of ANH, there were benefits in the amount of hemorrhage and transfusion, and no supplemen- tary plasma or platelet transfusion was needed after surgery when employing ANH. But, it showed a cutoff value only for massive bleeding surgery (at least 500 mL). In the case of cell salvage, the amount of blood transfusion was reduced in most cases and platelet or plasma transfusion was not required in most cases.
When the Leukoreduction filter (LDF) was utilized, it showed the effect of remov- ing bacterial infection or tumor cells. Nonetheless, the effectiveness and ben- efits for patients in certain condition of cell salvage and ANH is ambiguous with discrepancies among studies or patients. Therefore, the aim of this study is to provide clinical knowledge relative to the procedure, measure the efficacy and usefulness of peri-operative blood management mentioned above and discuss the forthcoming prospects and challenges.
Key words: Blood transfusion; Autologous; Operative blood salvage; Hemodilution
Corresponding Author: Jong Hyun Lee Department of Anesthesiology and Pain Medicine, Sejong General Hospital, 28, 489 gil Hohyeon-ro, Bucheon 14754, Korea Tel: +82-32-340-1255
Fax: +82-32-349-3005
E-mail: [email protected] Received
Revised Accepted
12 Oct 2017 25 Jan 2018 12 Feb 2018
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
not [9].
ACUTE NORMOVOLEMIC HEMODILUTION
1. ANH procedure [6]
The ideal timing to undertake ANH is just after anesthesia com- mences, but it also could be done when the patient sheds a lot of blood. Before surgery, the patient’s whole blood has to be extracted from vessels; using a 20G catheter with arterial pressure as a pump when drained from an artery and 16G or 14G catheter when drained from a vein by gravity. The amount of blood to be extracted can be determined by the formula given in Gross [10]: BV=EBV×2(HctIn–
HctTa)/(HctIn+HctTa); HctIn is initial hemoglobin concentration;
HctTa is Target hemoglobin concentration; EBV is the expected amount of bleeding, which is the amount of fluid in the body per kilogram (usually 60 to 65 mL/kg for men and 67 to 70 for women) multiplied by body weight. The extracted blood is stirred with a full dose of anticoagulant to prevent clotting and then kept in a freezer near zero degrees. Then to compensate for hemodilution, crystalloid or colloid fluid should be injected. At this point, it is important to note that the solution may disappear into the interstitium soon after [6]. Fig. 1. shows a blood bag filled with autologous blood.
2. Advantage of ANH [6,7,11]
Generally, it is easy to understand that up-to-date and new techniques are expensive. Nevertheless, ANH is a quite reasonable remedy in curtailing the volume of allogenic blood transfusion. The powerful advantage is in the technique itself. Because there is only one way to extract ones’ own blood in its entirety, ANH can supply
fresh autologous blood where most platelets and clotting factors are preserved and red blood cells (RBCs) are rarely lost. Moreover, when draining ones’ own blood, there is no need to examine the transfu- sion between the blood and the patients and there is no need to worry about transfusion side effects. Finally, because ANH is sim- pler than any other method, the process is simple, cost effective and can save blood storage time.
3. Indication of ANH [6,12,13]
ANH began with efforts to reduce allogenic blood transfusion by reducing RBC loss from bleeding [8]. For example, if the operation is expected to have a blood loss of 2 L, the RBC loss is twice as low as at 7 when the hematocrit is 14 g/dL. Therefore, it is possible to apply practically if a large amount of bleeding during surgery is expected.
Common indications for its use in surgery are listed in the following Table 1.
4. Effectiveness of ANH
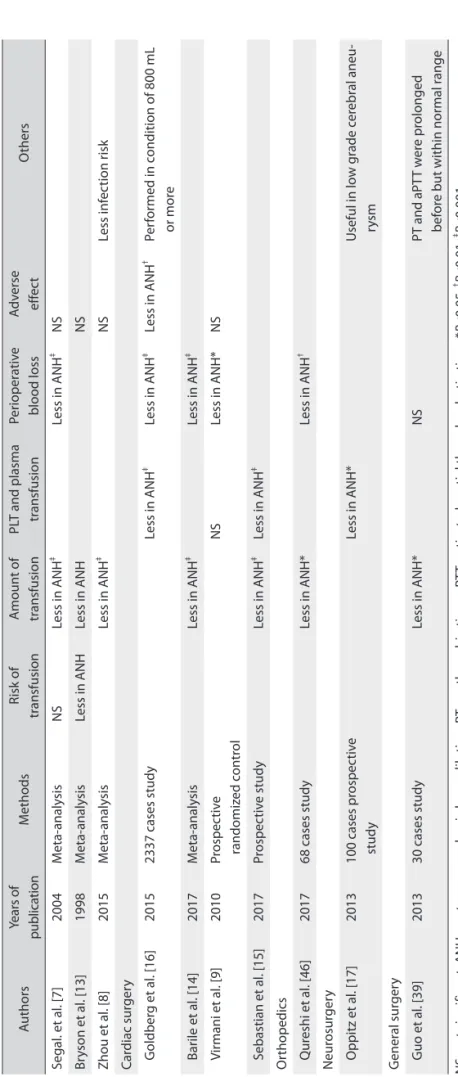
As can be seen from Table 2, the amount of blood transfusion in the ANH meta-analysis performed independently of the depart- ment was reduced consistently [7,8,13]. In a study by Segal et al. [7], the volume of about 303 mL of RBC transfusion could be saved.
There were no more side effects compared to the control group [7,8].
Studies in cardiac surgery have shown that ANH can reduce blood transfusions [14]. In addition, the number and function of platelets (PLTs) are not significantly different before and after sur- gery [9,15]. This is because theoretically PLT or coagulation factor
Table 1. Indication of ANH in surgery part
Department Surgical procedure
Cardiac procedure With or without extracorporeal circulation
Neurosurgery Tumors
Aneurysms Orthopedics Scoliosis
Prosthetics
Vascular Aneurysms
reconstructive surgery
Thoracic Pneumonectomy
Lobectomy
Urologic Prostatectomy
cystectomy nephrectomy
Others Rare blood groups
patients who have never experienced transfusion
Fig. 1. Autologous blood extracted during the perioperative state as shown is contained in the transfusion bag.
Table 2. Studies included in review article concerning effectiveness of ANH AuthorsYears of publicationMethodsRisk of transfusionAmount of transfusionPLT and plasma transfusionPerioperative blood lossAdverse effectOthers Segal. et al. [7]2004Meta-analysisNS Less in ANH‡ Less in ANH‡ NS Bryson et al. [13]1998Meta-analysisLess in ANHLess in ANHNS Zhou et al. [8]2015Meta-analysisLess in ANH‡ NSLess infection risk Cardiac surgery Goldberg et al. [16]20152337 cases studyLess in ANH‡ Less in ANH‡ Less in ANH† Performed in condition of 800 mL or more Barile et al. [14]2017Meta-analysisLess in ANH‡ Less in ANH‡ Virmani et al. [9]2010Prospective randomized controlNSLess in ANH*NS Sebastian et al. [15]2017Prospective studyLess in ANH‡ Less in ANH‡ Orthopedics Qureshi et al. [46]201768 cases studyLess in ANH*Less in ANH† Neurosurgery Oppitz et al. [17]2013100 cases prospective studyLess in ANH*Useful in low grade cerebral aneu- rysm General surgery Guo et al. [39]201330 cases studyLess in ANH*NSPT and aPTT were prolonged before but within normal range NS, not significant; ANH, acute normovolemic hemodilution; PT, prothrombin time; aPTT, activated partial thromboplastin time. *P<0.05. † P<0.01. ‡ P<0.001.
may disappear in the case of cell saver, but ANH does not lose its coagulation materials because it re-injects fresh whole blood to pa- tients. Notably, the use of ANH is more effective in surgery where massive hemorrhage is expected [15,16]. According to the study by Goldberg et al., ANH can be used to maximize the effect of ANH in bleeding over 800 mL [16].
As it was expected in other areas such as neurosurgery, orthope- dics and general surgery, additional PLT plasma transfusion was not required and did not result in coagulopathy after surgery. Although not consistent, the overall blood transfusion volume was reduced.
Particularly in neurosurgery, the oxygen supply to the brain was better in the ANH group than in the control group [17].
As a result, ANH has shown no consistent results but has positive effects on the volume of RBC transfusion, perioperative blood loss, PLT count, PLT function and loss of coagulation factors. Especially, it is more effective when applied to suspected massive bleeding or bleeding. Although overall ANH is effective, additional research is still needed.
5. Disadvantage of ANH [18]
Hemodynamic repercussion is a problem that can occur when using ANH [18]. For example, coagulation factors and RBCs are lost which can lead to bleeding problems, hypotension and tachycardia during surgery. That is why it is controversial whether it is appli- cable in patients with coronary artery disease, anemia and clotting disorders. In these patients, careful evaluation of potential problems should be completed before application. In addition, the major problem in ANH is sepsis, which is also contraindicated if there are abnormalities in major organs such as the lungs and kidneys or bac- teremia [6].
6. Cell salvage
Cell salvage started with the idea of re-using scattered blood dur- ing postpartum hemorrhage in 1818. Since then, similar attempts have been made in various medical parts. However, most trials re- sulted in a high mortality. In this flow, autologous blood transfusion has lost interest with the appearance of allogenic blood transfusion in the 1940s and 1950s [19]. Even with this trend, self-transfusion methods were considered continuously and were developed, but failed due to various side effects like hemolysis, air embolism and coagulation disorder. Finally, the first available device was intro- duced into the world was called the ‘cell saver’. Today, the cell saver is generally understood as a blood salvage apparatus [5].
7. How to operate cell salvage [5,19]
The ‘cell saver’ machine, which is widely used today, is shown in Fig. 2. Recently, self-transfusion machines, so-called cell saver, work in three phases; gathering, cleaning and re-injection. Gathering blood from patients who are in the operating room and bleeding a lot requires a specially designed double lumen catheter. Why do these devices need two lumens? Red blood cells (RBCs) exposed in air need immediate anticoagulant such as heparin or citrate because of coagulation. Thus, apart from the lumen into which the anti- coagulant is inserted, another lumen is required to pass the blood from patients to reservoir [19]. Blood mixed with heparin or citrate is collected in a bowl and its composition is separated by centrifuga- tion within it [5]. At this time, appropriate bowl volume and filling rate must be considered. Improper bowl volume causes more white blood cells (WBCs) to remain due to inadequate residue removal, which further destroys the balance of the hematocrit. In addition, if the filling rate is too fast, the RBCs will be lost into the debris reservoir. After collection and component separation, the RBCs are washed with a calculated amount of normal saline. That amount Fig. 2. Well-known cell salvage machine: cell saver.
varies from situation to situation, but in most cases, it is estimated to be three times the volume of the bowl. RBCs that have undergone all the procedures so far are put into a transfusion pack with normal saline and then re-injected to the patient, where the hematocrit is about 50 to 80% [19].
8. Advantage of cell salvage
The advance of cell salvage is that it can reduce allogenic blood transfusion and provide better quality RBCs. Allogenic blood trans- fusion can cause blood-borne infections such as hepatitis C or HIV.
In addition, there are still transfusion errors when transfusing glob- ally and immunological problems are being reported. Cell salvage is valuable in relieving allogenic transfusions, specifically lowering their exposure by 39% and minimizing the average reduction of 0.67 units per person [20].
If the RBCs come out of the body, they will be damaged in any way. Thus, the values that indicate viability of RBCs such as 2,3-DPG and cell membrane variability are very important [19]. First of all, 2, 3 DPG plays a role in releasing oxygen after transporting oxygen. In case of cell salvage, the level of 2,3-DPG is about 5% lower, which is not significantly different from fresh blood. On the other hand, in the case of blood stored for about 25 days, the value is reduced by 90% or more [5]. Secondly, because RBCs are usually larger than the minimum diameter of the capillaries, the flexibility of the RBC is important to allow smooth passage. According to study by Hovav et al. [21], in blood salvaging, deformability maintains biconcave
disc shape almost similar to fresh blood, but echinocyte shape is observed in long-term stored blood for allogenic blood. Taken to- gether, the above two facts show that salvaged RBCs are more adapt to carry oxygen.
9. Indication of cell salvage
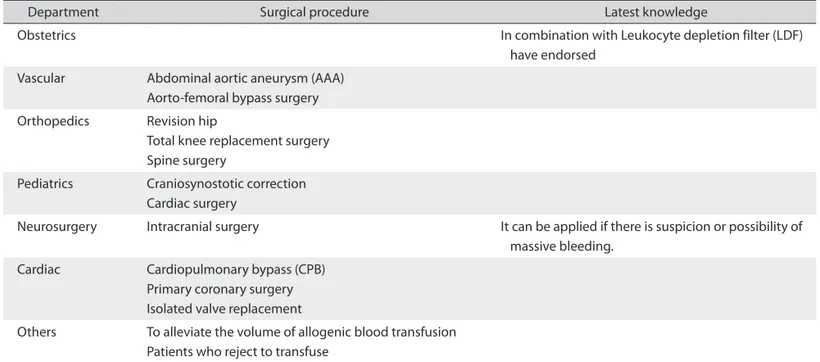
Cell salvage can be performed in elective surgery or in some emergent surgeries where massive bleeding is suspected. In particu- lar, it is now known to be used in obstetrics, vascular, orthopedics, pediatrics, neurosurgery, cardiac and urologic subdivisions [22]. Al- though not used in all operations of all branches, specific examples that are mainly applied are listed in Table 3 below.
10. Effectiveness of cell salvage
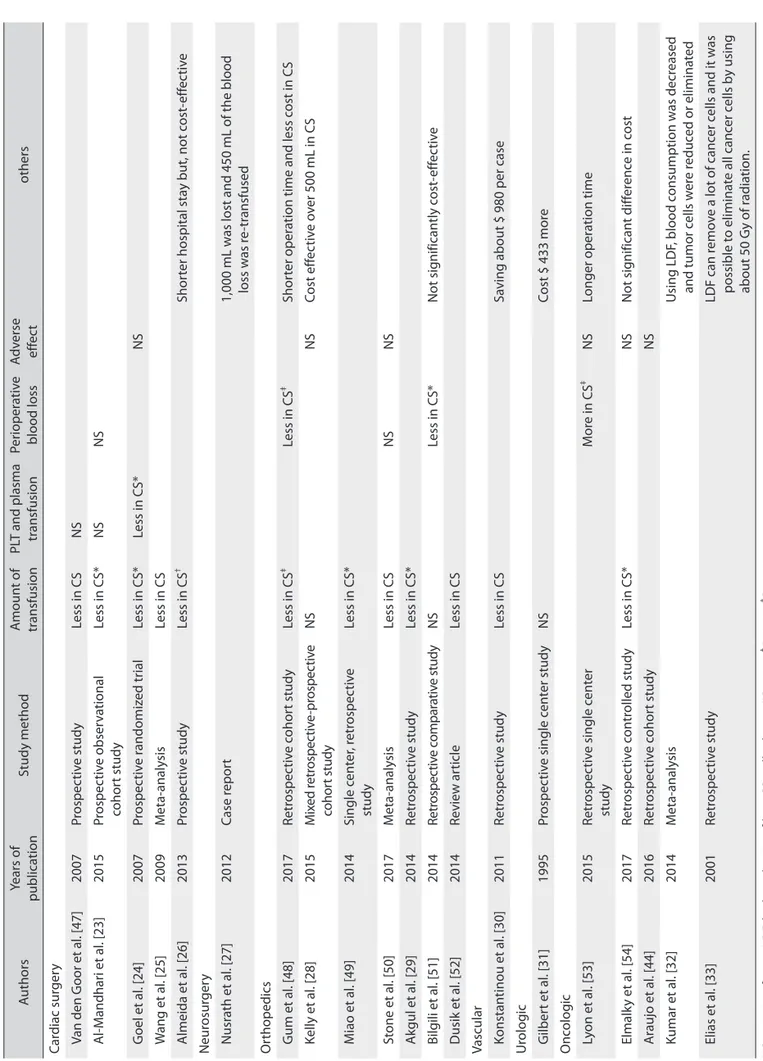
Let’s look at the effect of cell salvage on each part through Table 4. First of all, most articles in cardiac surgery were CABG surgery using cell salvaging. As a result, it has been reported in 4 studies that the cell saver has played an outstanding role in reducing blood transfusion [23-26]. Although disadvantage may be mentioned, it is predicted that the disadvantages of cell salvage may be dilutional coagulopathy, which may lead to a large number of transfusions of platelets or coagulation factors, but there was no difference between the two groups [23-25]. In addition, they have not come to the con- clusion that they are useful in terms of cost or whether or not it is useful [26].
Neurosurgery included only one case report, but the case was re-
Table 3. Indication of cell salvage
Department Surgical procedure Latest knowledge
Obstetrics In combination with Leukocyte depletion filter (LDF)
have endorsed Vascular Abdominal aortic aneurysm (AAA)
Aorto-femoral bypass surgery Orthopedics Revision hip
Total knee replacement surgery Spine surgery
Pediatrics Craniosynostotic correction Cardiac surgery
Neurosurgery Intracranial surgery It can be applied if there is suspicion or possibility of massive bleeding.
Cardiac Cardiopulmonary bypass (CPB) Primary coronary surgery Isolated valve replacement
Others To alleviate the volume of allogenic blood transfusion Patients who reject to transfuse
Table 4. Studies included in review article concerning effectiveness of cell salvage AuthorsYears of publicationStudy methodAmount of transfusionPLT and plasma transfusionPerioperative blood lossAdverse effectothers Cardiac surgery Van den Goor et al. [47]2007Prospective studyLess in CSNS Al-Mandhari et al. [23]2015Prospective observational cohort studyLess in CS*NSNS Goel et al. [24]2007Prospective randomized trialLess in CS*Less in CS*NS Wang et al. [25]2009Meta-analysisLess in CS Almeida et al. [26]2013Prospective studyLess in CS† Shorter hospital stay but, not cost-effective Neurosurgery Nusrath et al. [27]2012Case report1,000 mL was lost and 450 mL of the blood loss was re-transfused Orthopedics Gum et al. [48]2017Retrospective cohort studyLess in CS‡ Less in CS‡ Shorter operation time and less cost in CS Kelly et al. [28]2015Mixed retrospective-prospective cohort studyNSNSCost effective over 500 mL in CS Miao et al. [49]2014Single center, retrospective studyLess in CS* Stone et al. [50]2017Meta-analysisLess in CSNSNS Akgul et al. [29]2014Retrospective studyLess in CS* Bilgili et al. [51]2014Retrospective comparative studyNSLess in CS*Not significantly cost-effective Dusik et al. [52]2014Review articleLess in CS Vascular Konstantinou et al. [30]2011Retrospective studyLess in CSSaving about $ 980 per case Urologic Gilbert et al. [31]1995Prospective single center studyNSCost $ 433 more Oncologic Lyon et al. [53]2015Retrospective single center studyMore in CS‡ NSLonger operation time Elmalky et al. [54]2017Retrospective controlled studyLess in CS*NSNot significant difference in cost Araujo et al. [44]2016Retrospective cohort studyNS Kumar et al. [32]2014Meta-analysisUsing LDF, blood consumption was decreased and tumor cells were reduced or eliminated Elias et al. [33]2001Retrospective studyLDF can remove a lot of cancer cells and it was possible to eliminate all cancer cells by using about 50 Gy of radiation. NS, not significant; LDF, leukoreduction filter; CS, cell salvage. *P<0.05. † P<0.01. ‡ P<0.001.
transfused in about 450 mL of massive bleeding with an EBL of 40%, even for younger patients, with no additional complications or side effects observed. One notable point is that LDF was used to prevent the movement of infection or tumor cells in head and neck surgery. LDF has been shown to be useful for removing various particles as well as tumor cells in various articles [27].
In the orthopedic department, overall results are inconsistent. All but two of the seven studies report that allogenic blood transfu- sion has decreased. One of the reports stated that blood transfusion was not helpful was that there was no difference, but it is effective in large volumes of estimated blood loss after dividing into sub- groups based on the amount of hemorrhage. This study said that the minimal threshold is 500 mL [28]. In the other study, there were no significant differences between groups in most variables includ- ing perioperative transfusion [29]. Costs vary from reduced to more heavily expensive. The reason for this is that the price of blood transfusion varies from country to country and the price of cell sal- vage machines is also different.
It is known to be used mainly in AAA or AFB in the field of vas- cular surgery. In a study involving 62 patients, 2.52 units of packed RBCs could be reduced and cost savings of $ 980 per case was seen [30]. Of course, because it is a study conducted in Greece, the fact that it is not costly when considering differences across countries is encouraging the use of cell salvage in various fields. However, the radical prostatectomy performed at the urologic field did not show any advantage and in fact costed $ 433 more [31]. However, still seri- ous side effects are not seen in the cell saver group, and the costs are different for each country and can still be considered as an option.
Finally, the oncologic field is the most noticeable and controver- sial field of the present indications. Although, theoretically there is possibility of dissemination of cancer cells, all oncologic surgeries did not show any recurrence or death complications in the review articles presented above. Contrary to common sense, LDF showed better results than did not [32,33]. Because of the effect of LDF on tumor cells and lowering the inflammatory response, it can be said that LDF can overweigh the various disadvantages of the cell saver, especially when considering cancer [34]. However, because there is still lack of studies such as RCT, it is difficult to apply it directly to patients.
In addition to studies in six branches, cost-effectiveness of cell salvage is mentioned in several articles. Davies et al. show that alter- natives to cell salvage as well as other transfusions are sufficiently effective and cost-effective [35]. In addition, the study of intraop- erative cell salvage efficiency in South Africa was also found to be beneficial and economical [34,36]. Because of the lack of equipment
such as a cell saver, the cost of the equipment is not a benefit, but it is still reasonable in countries where the amount of transfusions is insufficient and the price per RBC unit is high.
11. Contraindication of cell salvage [5,19,22]
Prior to referring to contraindications, the taboo of cell salvage is divided into absolute and relative contraindications, which may or may not be contraindicated depending upon how the condition is controlled, so no mention of the distinction is made. There are four major cases of blood salvage. First, it is an infection problem. For example, if the amniotic fluid, fat, urine, bowel contents, etc. in the cesarean section are mixed, the extracted blood cannot be used. In addition, bacteria or viruses cannot be used for sepsis in the blood.
There is a LDF, antibiotics, etc., which will be mentioned again in the discussion [22]. Second, there is cell lysis. If the RBC is originally easy to be damaged, such as sickle cell anemia, there will also be a lot of smashed RBCs in the cell salvage pool. Third, there is a cancer problem. This is currently contraindicated in the opinion that cancer cells may be present in the blood and, if reintroduced, affects recur- rence after surgery. However, active research is currently underway on cell salvage in cancer. Finally, patients using agents that cause coagulation, such as thrombin or fibrin, may have problems with coagulation during migration to the saver reservoir [19].
12. Disadvantage of cell salvage
As can be seen from the indications, the problems that blood salvage can pose is that it can cause clotting problems. Autologous blood transfusions with blood salvage can lead to dilutional co- agulopathy because only normal saline is mixed with RBCs, unlike ANH [19]. This is similar to the situation where a large amount of allogenic transfusion is required to give platelets with the appropri- ate ratio among components. For example, in a traumatic situation with a lot of bleeding, there is also a paper written by Holcomb et al.
suggesting a ratio of 1: 1: 1 to compensate for platelet reduction [37].
DISCUSSION
Through the Cell saver and ANH, this review article has exam- ined the global flow of peri-operative blood management. Since blood management is a hot potato around the world, various efforts are being made to reduce blood transfusion from others. In the United States, the amount of blood transfusions used in periopera- tive situations amounts to 14.5 million units, which exceeds 10 bil- lion $ [15]. However, such a new blood management method is not fully established as an allogenic blood transfusion system, so there
is controversy as to when it can be applied and in what situations it should not be applied. Therefore, it is necessary to discuss the prob- lems and how to solve them.
First, ANH extracts the blood to the target hematocrit in a short time and after the course is completed it puts the fluid back into the patient. Thus, tachycardia, hypotension and myocardial infarction or ischemia may occur as a result of the decrease of the blood cells, which reduces the oxygen supply of the tissue. However, according to Barile et al., if the critical threshold is not exceeded, the reduced RBC viscosity is more effective in delivering oxygen to the tissue during CPB surgery [14,17]. Of the 646 patients who underwent ANH, 9 had myocardial infarction or ischemia, and there were no differences in the number of patients in the control group (634 patients, 10) [8]. Because it provides better supply of collateral or stenotic blood vessels in the myocardium and thus compensates for reduced oxygen delivery capacity [8,14,38]. However, some studies still point to the problem of anemic oxygen supply and there is no study to clarify the relationship, so further research is needed.
Second, coagulopathy occurs during surgery because PLT and coagulation factor are collected in transfusion bags after blood is drawn. In addition, as the hematocrit is removed to keep the target hematocrit, PLT and coagulation factors are also diluted, increasing the risk of intra-operative bleeding. Of course, ANH will only raise the intra-operative complication risk because it is a technique that extracts the entire blood back and puts it back in. In this regard, it is said that a reduction of less than 20% of the initial value does not increase the bleeding tendency during surgery [6,13]. Moreover, according to Sebastian et al. study, there was no statistically signifi- cant difference between PLT counts and functions before and after surgery, and even with syringes, there was no significant difference in turbulence and PLT degradation [15]. However, the differences in coagulation parameters, different blood sampling times, and differ- ent methods of measurement are still limitations [39].
Third, the expected blood loss has a significant impact on the ap- plication of ANH. In many studies, ANH is not effective in surgery where a small amount of bleeding is expected. The main advantage of ANH is that it reduces allogenic blood transfusion, as less bleed- ing reduces the amount of autologous transfusion and reduces the effect of blood transfusion frugality [15,16]. However, there is a need to study the cost savings of ANH which has been well adjusted for each country, because the costs for the unit of transfusion and pre- paring the equipment and manpower for each country or region are different.
Cell salvage cannot be adapted when contamination occurs.
For example, a contraindication is made in the case of sepsis with
bacterial infection and the case of a cesarean section with amni- otic rupture. Some studies have shown that infections with high frequency were observed in salvage blood, and in as many as 54%
of cases, blood culture was positive even after aseptic surgery [40].
Accordingly, washed cell salvage was used to cleanse collected RBCs to reduce risk of infection [41]. In addition, when LDF was added to the cell salvage, the load of infection was reduced by about 98% to 99%, and even when vancomycin was used, negative results were obtained in all culture results [5,40]. However, it is doubtful whether vancomycin can be used in a situation where the use of antibiotics is currently restricted worldwide. In addition, vancomycin is an anti- biotic that can be used in Gram-positive bacteria, but further studies are needed to know how other bacteria can be managed. Finally, it is known that LDF also helps to remove or lessen tumor cells [27,32,33], WBCs [42] and amniotic fluid [43] besides bacterial infection. Fur- ther study is needed to quantify the degree of LDF removal [33].
Since this cell salvage is a method of collecting and reusing blood cells from the operation, it has been known that cancer cells cannot be reintroduced because they may be present in the blood. However, there have been no studies showing a clear relationship between salvaged blood and cancer recurrence. According to Araujo TLC et al., liver transplantation with HCC did not show a significant differ- ence in recurrence rate and mortality in patients with salvaging and in those without. Rather, early stage cases showed better results [44].
Also, as mentioned in the previous paragraph, the use of LDF sig- nificantly reduced cancer cells, and it was clear that all of the tumor cells could be removed by irradiation of about 50 Gy [33]. Nonethe- less, there is still a limit to the extent to which RCT cannot proceed from an ethical point of view because cancer is likely to recur in theory.
Finally, it is a matter of platelets and coagulation factors. Cell salvage literally preserves only the red blood ‘cell’, so the aforemen- tioned platelets or clotting factors can be lost [19]. Cell saver group received more plasma and platelets and had a statistically significant difference [45]. In this situation, the use of anticoagulants to prevent coagulopathy cannot be used because of the increased risk of intra- operative bleeding. Therefore, can ‘PLT saver’ which preserve PLTs by directly collecting blood from the body and treating the antico- agulant be developed?
Concerning the transfusion problem, developed countries are not adequately balanced in demand and supply as they undergo an ag- ing population, and in the developing country, the price is still too expensive to use properly. Thus, based on the results of previous studies, the use of cell salvage or ANH is clinically well worth con- sidering and may be a good solution to the shortage of blood trans-
fused in the future. However, several factors hamper the progress of the study and application of perioperative blood management (PBM). First, there is no clear guideline concerning PBM because the exact effect is not known. Second, it is difficult to make a compari- son between studies because there are differences in enforcement method and scope of application for each hospital. Finally, each country has different conditions. For example, the introduction of such a new technology is useful when the blood is insufficient, but it is an obstacle to the application of such machinery when blood is administered nationwide. If we continue to use Cell salvage, ANH or other new methods in a wide range, we will need to study and agonize how to solve the various problems mentioned so far. In ad- dition, these new technologies are approached through evidence- based medicine as to why this expertise is needed and used in order to be accepted globally.
REFERENCES
1. Waters JH, Potter PS. Cell Salvage in the Jehovah’s witness patient.
pdf. Anesth Analg 2000;90:227-34.
2. Vries Hd. Use of the cell saver in blood management.pdf. EACTA 2012:33-5.
3. Eeles A, Baikady RR. Peri-operative blood management. Indian J Anaesth 2017;61:456-62.
4. Themistoklis T, Theodosia V, Konstantinos K, Georgios DI. Peri- operative blood management strategies for patients undergoing total knee replacement: where do we stand now? World J Orhop 2017;8:441-54.
5. Sikorski RA, Rizkalla NA, Yang WW, Frank SM. Autologous blood salvage in the era of patient blood management. Vox Sang 2017;112:499-510.
6. De Araújo LMT, Garcia LV. Acute normovolemic hemodilution: a practical approach. Open J Anesthesiol 2013;3:38-43.
7. Segal JB, Blasco-Colmenares E, Norris EJ, Guallar E. Preoperative acute normovolemic hemodilution: a meta-analysis. Transfusion 2004;44:632-44.
8. Zhou X, Zhang C, Wang Y, Yu L, Yan M. Preoperative acute nor- movolemic hemodilution for minimizing allogeneic blood transfu- sion: a meta-analysis. Anesth Analg 2015;121:1443-55.
9. Virmani S, Tempe DK, Pandey BC, Cheema AS, Datt V, Garg M, et al. Acute normovolemic hemodilution is not beneficial in patients undergoing primary elective valve surgery. Ann Card Anaesth 2010;13:34-8.
10. Gross JB. Estimating allowable blood loss: corrected for dilution.
Anesthesiology 1983;58:277-80.
11. Zhou J. A review of the application of autologous blood transfu- sion. Braz J Med Biol Res 2016;49:e5493.
12. Drummond JC, Petrovitch CT, Lane TA. Hemostasis and transfu- sion medicine. 6 ed. 2009.
13. Bryson GL, Laupacis A, Wells GA. does acute normovolemic he- modilution reduce perioperative allogenic transfusion? A meta- analysis. Anesth Analg 1998;86:9-15.
14. Barile L, Fominskiy E, Di Tomasso N, Alpizar Castro LE, Landoni G, De Luca M, et al. Acute normovolemic hemodilution reduces allogeneic red blood cell transfusion in cardiac surgery: a system- atic review and meta-analysis of randomized trials. Anesth Analg 2017;124:743-52.
15. Sebastian R, Ratliff T, Winch PD, Tumin D, Gomez D, Tobias J, et al. Revisiting acute normovolemic hemodilution and blood trans- fusion during pediatric cardiac surgery: a prospective observational study. Paediatr Anaesth 2017;27:85-90.
16. Goldberg J, Paugh TA, Dickinson TA, Fuller J, Paone G, Theurer PF, et al. Greater volume of acute normovolemic hemodilution may aid in reducing blood transfusions after cardiac surgery. Ann Tho- rac Surg 2015;100:1581-7; discussion 7.
17. Oppitz PP, Stefani MA. Acute normovolemic hemodilution is safe in neurosurgery. World Neurosurg 2013;79:719-24.
18. Murray D. Acute normovolemic hemodilution. Eur Spine J 2004;13 Suppl 1:S72-5.
19. Ashworth A, Klein AA. Cell salvage as part of a blood conservation strategy in anaesthesia. Br J Anaesth 2010;105:401-16.
20. Carless PA, Henry DA, Moxey AJ, O’Connell D, Brown T, Fergus- son DA. Cell salvage for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev 2010:CD001888.
21. Hovav T, Yedgar S, Manny N, Barshtein G. Alteration of red cell aggregability and shape during blood storage. Transfusion 1999;39:277-81.
22. Esper SA, Waters JH. Intra-operative cell salvage: a fresh look at the indications and contraindications. Blood Transfus 2011;9:139.
23. Al-Mandhari S, Maddali MM, Al-Bahrani MJ. Cell salvage dur- ing coronary artery bypass surgery and allogenic blood exposure.
Asian Cardiovasc Thorac Ann 2015;23:913-6.
24. Goel P, Pannu H, Mohan D, Arora R. Efficacy of cell saver in re- ducing homologous blood transfusions during OPCAB surgery: a prospective randomized trial. Transfus Med 2007;17:285-9.
25. Wang G, Bainbridge D, Martin J, Cheng D. The efficacy of an in- traoperative cell saver during cardiac surgery: a meta-analysis of randomized trials. Anesth Analg 2009;109:320-30.
26. Almeida RM, Leitao L. The use of cell saver system in cardiac surgery with cardiopulmonary bypass. Rev Bras Cir Cardiovasc
2013;28:76-82.
27. Nusrath MA, Edge CJ, Ahmed-Nusrath A. Intraoperative red cell salvage in head and neck surgery. Br J Oral Maxillofac Surg 2012;50:272-4.
28. Kelly PD, Parker SL, Mendenhall SK, Bible JE, Sivasubramaniam P, Shau DN, et al. Cost-effectiveness of cell saver in short-segment lumbar laminectomy and fusion (</=3 levels). Spine (Phila Pa 1976) 2015;40:E978-85.
29. Akgul T, Dikici F, Ekinci M, Buget M, Polat G, Sar C. The efficacy of cell saver method in the surgical treatment of adolescent idio- pathic scoliosis. Acta Orthop Traumatol Turc 2014;48:303-6.
30. Konstantinou EA, Brady JM, Soultati A, Mitsos A, Mamoura K, Mariolis TS, et al. Intraoperative use of cell saver on patients un- dergoing open abdominal aortic aneurysm surgical repair: a Greek hospital experience. J Perianesth Nurs 2011;26:225-30.
31. Gilbert JB, Malkowicz SB, Wein AJ. Cell saver and radical ret- ropubic prostatectomy: analysis of cost-effectiveness. Urology 1995;46:542-4.
32. Kumar N, Chen Y, Zaw AS, Nayak D, Ahmed Q, Soong R, et al. Use of intraoperative cell-salvage for autologous blood transfusions in metastatic spine tumour surgery: a systematic review. Lancet Oncol 2014;15:e33-e41.
33. ÉLias D, Billard V, Lapierre V. Use of the cell saver in oncologic sur- gery. Transfusion Alternatives in Transfusion Medicine 2001;3:25- 8.
34. Prieto MA, Guash S, Mendez JC, Munoz C, Planas A, Reyes G.
Does use of cell saver decrease the inflammatory response in car- diac surgery? Asian Cardiovasc Thorac Ann 2013;21:37-42.
35. Davies L, Brown T, Haynes S, Payne K, Elliott R, McCollum C.
cost-effectiveness fo cell salvage and alternative methods of mini- mising perioperative allogenic blood transfusion_a systematic review and economic model.pdf. Health Technol Assess 2006;10.
36. Solomon L, von Rahden RP, Allorto NL. Intra-operative cell salvage in South Africa: feasible, beneficial and economical. S Afr Med J 2013;103:754-7.
37. Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma:
the PROPPR randomized clinical trial. Jama 2015;313:471-82.
38. Luedi MM, Doll D, Boggs SD, Stueber F. Reduced blood viscosity plays minor role in regional blood flow increases during acute nor- movolemic hemodilution. Anesth Analg 2017;124:1738-9.
39. Guo JR, Jin XJ, Yu J, Xu F, Zhang YW, Shen HC, et al. Acute nor- movolemic hemodilution effects on perioperative coagulation in elderly patients undergoing hepatic carcinectomy. Asian Pac J Can-
cer Prev 2013;14:4529-32.
40. Perez-Ferrer A, Gredilla-Díaz E, de Vicente-Sánchez J, Navarro- Suay R, Gilsanz-Rodríguez F. Vancomycin added to the wash solu- tion of the cell-saver. Effect on bacterial contamination. Revista Española de Anestesiología y Reanimación (English Edition) 2017;64:185-91.
41. Meybohm P, Choorapoikayil S, Wessels A, Herrmann E, Zacha- rowski K, Spahn DR. Washed cell salvage in surgical patients: a review and meta-analysis of prospective randomized trials under PRISMA. Medicine (Baltimore) 2016;95:e4490.
42. Catling S, Williams S, Freites O, Rees M, Davies C, Hopkins L. Use of a leucocyte filter to remove tumour cells from intra-operative cell salvage blood. Anaesthesia 2008;63:1332-8.
43. Sullivan I, Faulds J, Ralph C. Contamination of salvaged maternal blood by amniotic fluid and fetal red cells during elective Caesar- ean section. Br J Anaesth 2008;101:225-9.
44. Araujo RL, Pantanali CA, Haddad L, Rocha Filho JA, D’Albu- querque LA, Andraus W. Does autologous blood transfusion dur- ing liver transplantation for hepatocellular carcinoma increase risk of recurrence? World J Gastrointest Surg 2016;8:161-8.
45. Al-Riyami AZ, Al-Khabori M, Baskaran B, Siddiqi M, Al-Sabti H.
Intra-operative cell salvage in cardiac surgery may increase platelet transfusion requirements: a cohort study. Vox Sang 2015;109:280-6.
46. Qureshi R, Puvanesarajah V, Jain A, Hassanzadeh H. Perioperative Management of Blood Loss in Spine Surgery. Clin Spine Surg 2017.
47. van den Goor JM, Nieuwland R, van Oeveren W, Rutten PM, Tijs- sen JG, Hau CM, et al. Cell Saver device efficiently removes cell- derived microparticles during cardiac surgery. J Thorac Cardiovasc Surg 2007;134:798-9.
48. Gum JL, Carreon LY, Kelly MP, Hostin R, Robinson C, Burton DC, et al. Cell saver for adult spinal deformity surgery reduces cost.
Spine Deform 2017;5:272-6.
49. Miao YL, Ma HS, Guo WZ, Wu JG, Liu Y, Shi WZ, et al. The effica- cy and cost-effectiveness of cell saver use in instrumented posterior correction and fusion surgery for scoliosis in school-aged children and adolescents. PLoS One 2014;9:e92997.
50. Stone N, Sardana V, Missiuna P. Indications and outcomes of cell saver in adolescent scoliosis correction surgery: a systematic re- view. Spine (Phila Pa 1976) 2017;42:E363-70.
51. Bilgili MG, Ercin E, Peker G, Kural C, Basaran SH, Duramaz A, et al. Efficiency and cost analysis of cell saver auto transfusion system in total knee arthroplasty. Balkan Med J 2014;31:149-53.
52. Dusik CJ, Hutchison C, Langelier D. The merits of cell salvage in arthroplasty surgery: an overview. Can J Surg 2014;57:61-6.
53. Lyon TD, Ferroni MC, Turner R, 2nd, Jones C, Jacobs BL, Davies
BJ. Short-term outcomes of intraoperative cell saver transfusion during open partial nephrectomy. Urology 2015;86:1153-8.
54. Elmalky M, Yasin N, Rodrigues-Pinto R, Stephenson J, Carroll C,
Smurthwaite G, et al. The safety, efficacy, and cost-effectiveness of intraoperative cell salvage in metastatic spine tumor surgery. Spine J 2017;17:977-82.