대한소화기학회지 2005;46:32-38
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 접수: 2004년 9월 24일, 승인: 2005년 5월 9일
연락처: 김남근, 463-712, 경기도 성남시 분당구 야탑동 351 포천중문의과대학교 임상의학연구소
Tel: (031) 780-5762, Fax: (031) 780-5766 E-mail: [email protected], [email protected]
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Correspondence to: Nam Keun Kim, Ph.D.
Institute for Clinical Research, Pochon CHA University College of Medicine, 351 Yatap-dong, Bundang-gu, Seongnam 463-712, Korea Tel: +82-31-780-5762, Fax: +82-31-780-5766
E-mail: [email protected], [email protected]
한국인 위암 환자에서 Thymidylate Synthase와 Methylenetetrahydrofolate Reductase
유전자 다형성의 임상 의의
포천중문의과대학교 임상의학연구소*, 분당차병원 내과학교실†, 외과학교실‡, 예방의학교실§
이 준*
,†․정철권
†․홍성표
†․정소영
†․오도연*
,†․황성규*
,†․안대호
‡․김세현
§․한진희*․김남근*
Clinical Significance of Thymidylate Synthase and Methylenetetrahydrofolate Reductase Gene Polymorphism in
Korean Patients with Gastric Cancer
Jun Lee, M.D.*,†, Cheol Kweon Jeong, M.D.†, Sung Pyo Hong, M.D.†, So Young Chong, M.D.†, Doyeun Oh, M.D.*,†, Seong Gyu Hwang, M.D.*,†,
Dae Ho Ahn, M.D.‡, Sehyun Kim, Ph.D.§, Jin Hee Han, M.S.*, and Nam Keun Kim, Ph.D.*
Institute for Clinical Research*, Departments of Internal Medicine†, General Surgery‡, and Preventive Medicine§, Pochon CHA University College of Medicine, Seongnam, Korea
Background/Aims: Thymidylate synthase (TS) is a target enzyme of 5-fluorouracil (5-FU) and has a polymorphic 28 bp tandem repeated sequence. TS enhancer region (TSER) polymorphism has been associated with the efficacy of 5-FU-based chemotherapy in colon cancer. Methylenetetrahydrofolate reductase (MTHFR) plays a central role in converting folate to methyl donor for DNA methylation. The aim of this study was to determine the clinical value of TSER and MTHFR polymorphism in gastric cancer. Methods: From October, 1995 to February, 2002, 40 gastric cancer patients underwent operation and 25 patients among those patients have received postoperative 5-FU-based chemotherapy (5-FU (+) group). Peripherial blood were sampled for TSER and MTHFR genotype analysis by PCR amplification of genomic DNA. The survival of patients according to TSER and MTHFR polymorphism were compared. Results: We observed a longer survival in stage II than stage III of the patients (p=0.0037). However, the TSER and MTHFR C677T polymorphisms were not associated with better survival of gastric cancer patients as well as combined TSER and MTHFR genotypes with 5-FU chemotherapy. Conclusions:
The TSER and MTHFR genotypes are not effective markers for tumor sensitivity to 5-FU-based chemotherapy in Korean gastric cancer patients after curative resection. These results may suggest further large-scale study about TSER and MTHFR polymorphism for the prediction of efficacy of 5-FU-based chemotherapy in gastric cancer in Korea. (Korean J Gastroenterol 2005;46:32-38)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: 5-fluoropyrimidine; Thymidylate synthase; Methylenetetrahydrofolate reductase; Gastric cancer
이 준 외 9인. 한국인 위암 환자에서 TS와 MTHFR 유전자 다형성의 임상 의의 33
서 론
5-fluorouracil (5-FU)는 항대사물질 계열의 항암제로 de- oxyuridylate monophosphate (dUMP)를 deoxythymidylate mono- phosphate (dTMP)로 메틸화시키는 효소인 thymidylate syn- thase (TS)를 차단하여 항암효과를 나타낸다.1 종양조직의 TS 발현은 종양마다 다양하고, 5-FU를 기초로 한 항암치료 에 대한 반응 민감도는 종양 내 TS 단백질 발현량과 관련이 있다.2-4 현재까지 임상연구 결과 5-FU 투여 후 TS에 대한 불충분한 억제가 5-FU에 대한 약제내성의 주요 기전이다.5-7 TS enhancer region (TSER)의 28 bp가 2회 반복된 것을 2R, 3회 반복된 것을 3R로 표기하며, 반복횟수가 높을수록 TS mRNA 및 단백질 발현율이 높다.8,9 위암 환자에서 TS 발현 율이 높을수록 5-FU에 의한 항암치료 효과가 감소하며, 따 라서 생존율도 낮아진다.10-12 위암에서 TSER 유전자형과 TS mRNA량은 관련이 없는 반면, TS 단백질량은 TSER 유전자 형에 의해 조절되지만,13 TSER 유전자형이 위암 환자에서 어떤 의의를 갖는지에 대해서는 아직까지 논란이 많다.7,14-16 5,10-methylenetetrahydrofolate reductase (MTHFR)는 meth- ylene THF을 methyl THF로 전환시키는 효소이며, 이때 사용 되는 methylene THF는 dUMP를 dTMP로 전환시키는 효소인 TS에 대한 cofactor로도 이용되기 때문에, TS 활성도 변화에 따라 MTHFR 활성도에도 영향을 준다. MTHFR 기능은 엽 산이 부족하거나 MTHFR 유전자에 돌연변이가 생기면 감 소한다. 따라서 MTHFR 유전자 돌연변이를 가진 사람은 정 상인 사람과 동일한 양의 엽산 섭취에도 불구하고 엽산대사 에 영향을 주어 위암 발병 가능성이 높다.17,18 MTHFR 유전 자 돌연변이는 C677T와 A1298C의 두 종류로, 모든 MTHFR 돌연변이에서 효소활성이 감소되어 혈중 엽산 농도를 떨어 뜨리는 동시에 호모시스테인의 농도를 증가시킨다.
MTHFR 유전자 돌연변이는 677번째 염기가 cytosine에서 thymine으로 바뀌어(677C→T) 226번째 아미노산인 alanine 이 valine으로 대체되어 발생하며, 677CC, CT, TT형의 세 종 류가 있다. 정상형인 677CC가 100%의 효소활성을 갖는다 면, 동형접합 변이인 677TT는 약 30%, 이형접합 변이인 677CT는 약 65%의 활성도를 갖는다. 두 번째 변이는 1298 염기가 adenine에서 cytosine으로 전환되어(1298A→C), 아미 노산이 glutamate에서 alanine으로 대체되어 발생하며, C677T 의 변이에 비해 A1298C 변이는 MTHFR 효소 활성도에 미 치는 영향이 상대적으로 적다.
MTHFR 유전자형과 5-FU 투여효과에 대한 연구는 대장 암에서 보고된 예가 있으나 아직까지 위암에서는 거의 보고 된 바 없다.19 최근 들어 TS와 MTHFR의 특정 유전자와 위 암의 발병과의 관련성에 대한 연구 결과들이 있다.15,16,20-22
그러므로 이번 연구에서는 아직까지 TSER과 MTHFR 유전
자의 위암 환자에서의 역할이 명확하게 규명되어 있지 않으 므로 수술 후 항암제 투여에 대한 반응 등의 임상 의의를 알아보고자 하였다.
대상 및 방법
1. 대상
1995년 10월부터 2002년 2월까지 분당차병원에서 위암수 술을 받은 환자 중 병기 II, III인 환자 40명을 대상으로 2003 년 11월 1일을 기준으로 사망여부를 조사하여 생존율을 관 찰하였다. 이들은 남자 19명, 여자 21명이었으며, 평균 나이 는 58.0세(범위 32-77세)였다. 항암치료를 시행한 환자를 5-FU (+)군, 치료하지 않은 환자를 5-FU (-)군으로 구분하 였으며, 총 40명 중 5-FU (+)군 25명(62.5%)과 5-FU (-)군 15명(37.5%)이었다. 5-FU (+)군의 병기 구성은 병기 II 8명 (32.0%), 병기 III 17명(68.0%), 5-FU (-)군의 병기 구성은 병 기 II 8명(53.3%), 병기 III 7명(46.7%)이었다.
2. 방법
1) 항암치료
수술 후 보조항암 화학요법은 총 40명 중 25명에서 시행하 였으며, 항암치료 약제는 5-FU를 기초로 하여 ELF (5-FU 500 mg/m2, etoposide 100 mg/m2, leucovorin 20 mg/m2, D1-5), FP (5-FU 750 mg/m2, D1-5, CDDP 100 mg/m2, D1)를 4주에 한 번씩, 6주기 정맥주사 하였다.
2) TSER과 MTHFR 유전자 다형성분석
DNA 분리는 DNA 추출 키트(extraction column, QIAmp blood kit, Qiagen)를 이용하였고 제조자의 지침에 따라서 환 자의 혈액에서 추출한 백혈구로부터 분리하였다.
(1) TSER 유전자 다형성분석
Genomic DNA는 10 mM Tris/1 mM EDTA pH 8.0에 보관 되어 있는 것으로 sense primer (5'-GTG GCT CCT GCG TTT CCC CC-3')와 antisense primer (5'-GCT CCG AGC CCG GCC ACA GGC ATG GCG CGG-3’)를 이용하여 GeneAmp PCR machine (Perkin Elmer 2400, Norwalk, CT, USA)으로 분 석하였다. 94oC에서 40초 동안 변성(denaturation), 62oC에서 1분간 아닐링(annealing), 72oC에서 40초 동안 연장반응 과정 을 35주기 반복하고 72oC에서 5분간 반응시켰다. 증폭된 DNA 조각은 3.5% 아가로스 젤에 전기영동 후 ethidium bro- mide로 염색하여 변이상태를 관찰하였다. 동형접합체이며 double repeat인 2R/2R은 214 bp에서, 이형접합체인 2R/3R은 214 bp와 242 bp에서, 동형접합체이며 triple repeat인 3R/3R 은 242 bp에서 각각 밴드를 생성하였다(Fig. 1A). TSER 유전
34 The Korean Journal of Gastroenterology: Vol. 46, No. 1, 2005
자는 동형접합인 2R/2R과 3R/3R, 이형접합인 2R/3R 유전자 로 구분하였다.
(2) MTHFR C677T 유전자 다형성분석
분리한 DNA는 MTHFR 677번 염기를 포함하는 부분을 증 폭하기 위해 sense primer (5'-TGA AGG AGA AGG TGT CTG CGG GA-3')와 antisense primer (5'-AGG ACG GTG CGG TGA GAG TC-3')를 각각 사용하였다. 198 bp 생성물 을 증폭시키기 위해 95oC에서 60초 동안 변성, 61oC에서 60 초 동안 시발체를 아닐닝, 72oC에서 120초 동안 연장반응 과정을 35주기 반복하였다. 증폭된 단편들에서 MTHFR C677T를 인식할 수 있는 제한효소 HinfI으로 37oC에서 3-4 시간 동안 분해하였다. 이후 HinfI으로 처리한 단편들은 2.5% 아가로스 젤로 전기영동 후 염색하여 변이상태를 확 인하였다. MTHFR C677T 부위의 변이형은 PCR-based RFLP
방법으로 분석한 결과 세 가지였는데, 677CC 야생형은 HinfI에 분해되지 않아 단지 198 bp의 절편만이 보였고, 677CT인 이형 접합 변이는 198 bp, 175 bp, 23 bp 절편이 보 였고, 그리고 677TT 동형 접합 변이는 175 bp와 23 bp 절편 이 각각 관찰되었다(Fig. 1B).
(3) 통계분석
통계분석은 수술 받은 위암환자의 TSER 대립유전자 2R 과 3R 비율의 차이검증과 이들 중 병기 II와 III 각각에서 TSER 대립유전자 2R과 3R 비율의 차이를 검정하기 위하여 Chi-square test for equal proportions를 이용하였다. 나이 차이 는 two-sample independent t-test로 검정하였고, 성별과 항암 요법 유무의 차이는 Chi-square 검정 방법을 이용하였다. 생 존율의 차이 검정은 log-rank test를 이용하였으며, 모든 검정 방법에서 유의 수준은 0.05로 정하였다.
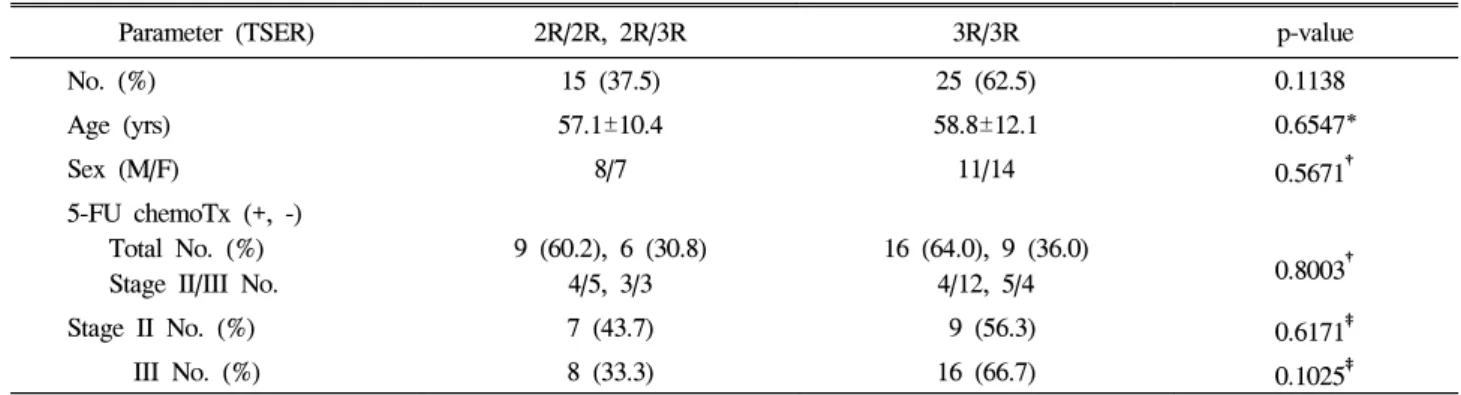
Table 1. Characteristics of Patients according to TSER Genotype
Parameter (TSER) 2R/2R, 2R/3R 3R/3R p-value
No. (%) 15 (37.5) 25 (62.5) 0.1138
Age (yrs) 57.1±10.4 58.8±12.1 0.6547*
Sex (M/F) 8/7 11/14 0.5671†
5-FU chemoTx (+, -) Total No. (%) Stage II/III No.
9 (60.2), 6 (30.8) 4/5, 3/3
16 (64.0), 9 (36.0)
4/12, 5/4 0.8003†
Stage II No. (%) 7 (43.7) 9 (56.3) 0.6171‡
III No. (%) 8 (33.3) 16 (66.7) 0.1025‡
TSER, thymidylate synthase enhancer region; 5-FU, 5-fluorouracil; chemoTx, chemotherapy.
Value, mean±SD.
* Two-sample independent t-test.
†Chi-square test.
‡Chi-square test for equal proportions.
Fig. 1. (A) The TSER polymor- phism of the tandem repeat in gas- tric cancer. PCR assay for deter- mination of the TSER genotype reveals that 214 and 242 bp frag- ments represent the 2- and 3-re- peat sequences, respectively. The genotypes are classified into 2R/2R, 3R/3R, 2R/3R. (B) The MTHFR C677T polymorphism in gastric cancer. Analysis by PCR-RFLP methods reveals that the 677CC type is identified by the presence of only a 198 bp fragment, and 677CT type by 198, 175 and 23 bp fragments, and 677TT type by 175 and 23 bp fragments.
TSER, thymidylate synthase en- hancer region; MTHFR, methyl- enetetrahydrofolate reductase.
400 bp
A
TSER MTHFR300 bp 200 bp
242 bp 214 bp
200 bp
100 bp
198 bp 175 bp
M 2R/2R 2R/3R 3R/3R M CC CT TT
B
Lee J, et al. Clinical Significance of TS and MTHFR Gene Polymorphism in Korean Patients with Gastric Cancer 35
결 과
1. TSER과 MTHFR 유전자 분포
TSER 반복연쇄에 따른 위암 환자 구성은 총 40명 중 2 명(5.0%)은 동형접합 2R/2R, 13명(32.5%)은 이형접합 2R/
3R이었고, 25명(62.5%)은 동형접합 3R/3R이었다. 항암치 료 유무에 따른 TSER 반복연쇄 분포는 5-FU (+)군 25명 중 동형접합 2R/2R 1명, 이형접합 2R/3R 8명, 동형접합 3R/3R 16명이었고, 5-FU (-)군 15명 중 동형접합 2R/2R은 1명, 이형접합 2R/3R 5명, 동형접합 3R/3R 9명이었다.
항암치료 여부에 따른 병기별 TSER 28 bp 반복서열 분포 는 5-FU (+)군에서 병기 II (8명)는 동형접합 2R/2R 1명 (12.5%), 이형접합 2R/3R 3명(37.5%), 동형접합 3R/3R 4명 (50.0%)이었고, 병기 III (17명)는 동형접합 2R/2R은 없었고, 이형접합 2R/3R 5명(29.4%), 동형접합 3R/3R 12명(70.6%)이 었다. 5-FU (-) 군에서 병기 II (8명)는 동형접합 2R/2R은 없 었고, 이형접합 2R/3R 3명(37.5%), 동형접합 3R/3R 5명(62.5%) 이었고, 병기 III (7명)는 동형접합 2R/2R 1명(14.3%), 이형접 합 2R/3R 2명(28.6%), 동형접합 3R/3R 4명(57.1%)이었다.
3가지 TSER 유전자형과 나이, 성별, 개체수, 항암치료, 병기와 유의한 차이는 없었다(Table 1).
MTHFR 변이에 따른 위암 환자 구성은 총 40명 중 MTHFR 677CC 12명(30.0%), 677CT 23명(57.5%), 677TT 5명 (12.5%)로 CT형이 많았다. 항암치료 여부에 따른 MTHFR 변이 분포는 5-FU (+)군 25명은 MTHFR 677CC 7명, 677CT 15명, 677TT 3명, 5-FU (-)군 15명은 MTHFR 677CC 5명, 677CT 8명, 677TT 2명이었다.
항암치료 여부와 병기에 따른 MTHFR 변이 분포는 5-FU
(+)군에서 병기 II (8명)에서 MTHFR 677CC 3명, 677CT 3 명, 677TT 2명, 병기 III (17명)에서 MTHFR 677CC 4명, 677CT 12명, 677TT 1명이었다. 5-FU (-)군에서 병기 II (8 명)에서 MTHFR 677CC 3명, 677CT 5명, 677TT 0명, 병기 III (7명)에서 MTHFR 677CC 2명, 677CT 3명, 677TT 2명이 었다.
항암치료 군에서 병기 III 중 MTHFR 677CT 개체수가 많 았다(p=0.0076). 나이와 성별, 항암치료, 병기 등의 구성에서 차이는 없었다(Table 2).
2. 병기 및 항암치료에 따른 생존율
병기 II 16명, 병기 III 24명의 수술 후 생존율을 비교하였 다(Fig. 2). 병기 II 환자의 생존기간이 병기 III보다 의미 있
Table 2. Characteristics of Patients according to MTHFR Genotype
Parameter (MTHFR) CC CT TT p-value
No. (%) 12 (30.0) 23 (57.5) 5 (12.5) 0.0021
Age (yrs) 59.8±9.6 55.4±12.2 67.0±6.4 0.0954*
Sex (M/F) 6/6 11/12 2/3 0.9306†
5-FU (+, -) Total No. (%) Stage II/III No.
7 (59.3), 5 (40.7) 3/4, 3/2
15 (65.2), 8 (34.8) 3/12, 5/3
3 (60), 2 (40)
2/1, 0/2 0.9164† Stage II No. (%) 6 (37.5) 8 (50.0) 2 (12.5) 0.1738‡ III No. (%) 6 (25.0) 15 (62.5) 3 (12.5) 0.0076‡ MTHFR, methylenetetrahydrofolate reductase; 5-FU, 5-fluorouracil.
Value, mean±SD.
* Two-sample independent t-test.
†Chi-square test.
‡Chi-square test for equal proportions.
Fig. 2. The survival curves by stage II and III of gastric cancer.
The overall survival of stage II is superior to that of stage III (p=0.0037) (Stage II-solid line, Stage III-dotted line).
36 대한소화기학회지: 제46권 제1호, 2005
게 길었다(p=0.0037). 그러나 병기에 따른 5-FU 치료 생존율 을 비교하였을 때, 병기 II와 병기 III에서 두 군 간에 생존 율의 차이가 없었다. 병기별 추적기간(중앙값)을 보면, 병기 II가 75개월, 병기 III는 34개월이었다. 그리고 병기별 재발 률은 병기 II가 18.8% (3/16), 병기 III가 37.5% (9/24)였다 (p=0.2049). 또한, 병기별 전체 생존기간(중앙값)을 보면, 병 기 III는 46개월이었으며, 병기 II에서는 16명 중 2명만이 사 망하여 중앙값에 도달하지 않았다.
3. TSER과 MTHFR 유전자형에 따른 생존율
TSER 유전자형에 따른 생존율은 의미 있는 차이가 없었 다(Fig. 3). 또한 TSER 유전자형별로 항암치료 유무에 따른 TSER 유전자형과 생존율은 의미 있는 차이가 없었다.
MTHFR 변이형에 따른 생존율 역시 의미 있는 차이는 없 었다(Fig. 4). MTHFR 변이에 따라 항암치료의 유무에 따른 MTHFR 변이형의 생존율도 의미 있는 차이가 없었다.
TSER과 MTHFR의 각각의 변수에 관해서 조합하여 각각 의 조합에서 항암치료 유무에 따른 생존율을 비교해 보았다 (Table 3). 개체수는 TSER 2R/2R+2R/3R & MTHFR 677CC (6명), TSER 2R/2R+2R/3R & MTHFR 677CT (8명), TSER 2R/2R+2R/3R & MTHFR 677TT (1명), TSER 3R/3R &
MTHFR 677CC (6명), TSER 3R/3R & MTHFR 677CT (15명), TSER 3R/3R & MTHFR 677TT (4명)의 생존율을 항암치료 유무에 따라 비교해 보았으나 모두 의미 있는 차이를 보이 지 않았다(p=0.0718).
고 찰
TS는 18번 염색체 단완에 위치하며, dUMP를 dTMP로 전 환시키는데 꼭 필요한 효소이다. 그리고, 동형접합 3R/3R 유전자형은 동형접합 2R/2R 유전자형에 비해 3-4배 높은 mRNA 및 단백질 발현량을 보이며, 위암조직에서도 TSER 의 28 bp 반복횟수의 차이가 TS 단백질 발현량에 영향을 미 친다.15 또한, 위암환자에서 TS mRNA와 단백질 발현량이 많은 TSER 3R/3R에서 5-FU 항암제에 대한 저항성이 높아 서 생존율이 나쁘다.13 위암에서 5-FU에 기초한 항암치료에 대한 반응률의 예후예측 인자로서 TS 발현이 높은 군에서 항암제에 대한 반응이 좋지 않다.4 반면 TS 유전자 발현과 5-FU에 대한 반응과는 무관하다는 주장도 있으며, 세포 내 에서 TS 활성도가 높은 위암환자에서 5-FU에 대한 반응이 오히려 좋은 것을 보고하는 등 현재까지 5-FU에 대한 항암 효과의 예측지표 또는 종양의 예후인자로서의 TSER의 역
Table 3. Distribution of Patients according to TSER and MTHFR C677T Combined Genotypes
MTHFR 677CC (%) MTHFR 677CT (%) MTHFR 677TT (%)
TSER 2R/2R+2R/3R (%) 6 (15.0) 8 (20.0) 1 (2.5)
TSER 3R/3R (%) 6 (15.0) 15 (37.5) 4 (10.0)
TSER, thymidylate synthase enhancer region; MTHFR, methylenetetrahydrofolate reductase.
Fig. 3. The survival curves by TSER genotypes of gastric cancer.
The survival of 3R/3R TSER genotype is not superior to that of 2R/2R+2R/3R TSER genotype (p=0.8686) (2R/2R+2R/3R TSER genotype-solid line, 3R/3R TSER genotype-dotted line).
TSER, thymidylate synthase enhancer region.
Fig. 4. The survival curves by MTHFR C677T genotypes of gastric cancer. The survival of MTHFR 677CC, 677CT, 677TT don't show statistical significance (p=0.8977) (MTHFR 677CC- solid line, 677CT-small dotted line, 677TT-large dotted line).
MTHFR, methylenetetrahydrofolate reductase.
이 준 외 9인. 한국인 위암 환자에서 TS와 MTHFR 유전자 다형성의 임상 의의 37
할에 대해서는 아직 논란이 많다.23-25
대장암은 대부분 분화가 잘되어 종양 내 정상세포는 거의 없고, 종양세포만 가득 차 있어, TS 활성도를 판단하기 위 해서 TS mRNA나 TS 단백질의 정량화가 유용하다. 실제로 전이 대장암 환자의 종양조직에서 TS 효소의 활성이 TSER 3R/3R보다 2R/3R에서 훨씬 높게 나타나서 유전자형과는 일 치하지 않는 결과를 보였다.26 그러나 위암 환자에서는 종양 조직 내에도 정상세포가 많이 분포되어 있어서 TS mRNA 나 단백질의 정량화는 위양성 및 위음성의 가능성이 많기 때문에 TSER 유전자가 더 적은 오류를 보여 더 유용할 것 이다.
이번 연구에서는 TSER의 28 bp의 반복횟수에 따라 2R/
2R, 2R/3R, 3R/3R로 구분하였고, 총 40명의 대상 환자 중 2R/2R 형은 2명으로 수가 적어서 2R/2R과 2R/3R를 통합하 여 생존율과 항암치료의 반응을 비교하였다. 병기 II와 III만 을 분석한 이유는 같은 유전자에서 항암치료를 받은 군과 받지 않은 군을 비교하기 위해서 수술 불가능한 병기 IV와 항암치료를 하지 않는 병기 I은 제외하였다. 이번 연구에서 는 TSER의 28 bp 반복에 따른 유전자 간의 생존율에 유의 한 차이는 발견되지 않았다. 병기별로 수술 후 생존율을 비 교했을 때 병기 II가 더 오래 생존하였으나, 항암치료 여부 에 따른 TSER 유전자에 따른 생존율을 비교할 때 2R/2R과 2R/3R을 합한 군과 3R/3R군 사이에 유의한 차이는 없었다 (Fig. 3).
MTHFR C677T와 MTHFR A1298C의 변이는 효소 활성을 20-30%로 떨어뜨린다. 위암 환자의 MTHFR 활성도 차이가 분문부 위암의 발병위험과 관련이 있다.21
이번 연구에서는 MTHFR의 677CC, CT, TT 각 변이에 따 라 생존율을 비교하여 보았으나 유의한 차이는 관찰되지 않 았다(Fig. 4). 또한, 병기별로 항암치료 유무에 따른 생존율 과 TSER과 MTHFR 유전자 조합들 간에 비교해 보았으나 마찬가지로 의미 있는 차이를 볼 수 없었다. 특히, MTHFR 677TT와 TSER 3R/3R이 MTHFR 677CC, TSER 2R/2R보다 생존율이 높은 경향에 대해서는 항암제 투여여부, 투여횟 수, 투여약제의 종류, 고혈압, 당뇨병 등 다른 질환 관련 등 에 대한 종합적인 분석이 요구된다. 결론적으로, TSER과 MTHFR 유전자 다형성을 항암치료에 대한 예측인자로 이 용하기 위해서는 앞으로 보다 많은 환자를 대상으로 한 체 계적인 연구와 TS 효소 활성도에 영향을 주는 다른 돌연변 이들에 대한 추가 연구가 이루어져야 할 것이다.
요 약
목적: 위암치료제로 널리 사용되는 5-fluoropyrimidine 계 열의 항암제는 thymidylate synthase 억제제로 유전자의 돌연
변이가 효능에 영향을 미친다. TSER 돌연변이는 이미 결장 직장암의 항암치료에 대한 반응 예측인자로 고려되고 있지 만 위암에서는 아직 불분명하다. 그러므로 이번 연구에서는 위암 환자를 대상으로 TSER과 MTHFR 유전자 돌연변이에 따른 전체 생존율과 임상 역할을 알아보고자 하였다. 대상 및 방법: 1995년 10월부터 2002년 2월까지 분당차병원에서 위암수술을 받은 환자들 중 병기 II, III기 환자 40명을 대상 으로 2003년 11월 1일을 기준으로 생존여부를 조사하였다.
TSER과 MTHFR 유전자 결정은 환자 혈액에서 DNA를 분 리하여 PCR-RFLP 방법으로 실시하였다. 5-FU를 포함하는 보조항암 화학요법을 시행한 환자를 5-FU (+)군, 치료하지 않는 환자를 5-FU (-)군으로 구분하였다. 결과: 병기별 생존 율 비교에서는 병기 II가 병기 III에 비하여 의미 있는 차이 로 생존기간이 길었다. 그러나 유전자 간 생존율 비교에서 는 MTHFR 677CC, CT, TT의 3가지 유전자와 TSER 2R/2R, 2R/3R, 3R/3R의 3가지 유전자 간에 유의한 차이를 발견할 수 없었다. 또한, MTHFR C677T와 TSER 유전자 조합에서 도 이러한 차이는 보이지 않았다. 결론: TSER과 MTHFR 유 전자는 위암수술 후 5-FU 항암치료의 효과를 예측하는 표 지인자로 효과적이지 못하였다. 그러나 이들 유전자와 항암 치료 효과의 관련성을 확립하기 위해 보다 많은 위암 환자 를 대상으로 한 연구가 요구된다.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 색인단어: 5-fluoropyrimidine, Thymidylate synthase, Methyle-
netetrahydrofolate reductase, 위암
참고문헌
1. Pinedo HM, Peters GF. Fluorouracil: biochemistry and phar- macology. J Clin Oncol 1988;6:1653-1664.
2. Nishimura R, Nagao K, Miyayama H, et al. Thymidylate syn- thase levels as a therapeutic and prognostic predictor in breast cancer. Anticancer Res 1999;19:5621-5626.
3. Salonga D, Danenberg KD, Johnson M, et al. Colorectal tu- mors responding to 5-fluorouracil have low gene expression levels of dihydropyrimidine dehydrogenase, thymidylate syn- thase, and thymidine phosphorylase. Clin Cancer Res 2000;6:
1322-1327.
4. Yeh KH, Shun CT, Chen CL, et al. High expression of thy- midylate synthase is associated with the drug resistance of gastric carcinoma to high dose 5-fluorouracil-based systemic chemotherapy. Cancer 1998;82:1626-1631.
5. Peters GJ, van der Wilt CL, van Groeningen CJ. Predictive value of thymidylate synthase and dihydropyrimidine dehy- drogenase. Eur J Cancer 1994;30:1408-1411.
6. Peters GJ, van der Wilt CL, van Triest B, et al. Thymidylate
38 The Korean Journal of Gastroenterology: Vol. 46, No. 1, 2005
synthase and drug resistance. Eur J Cancer 1995;31:1299- 1305.
7. Iacopetta B, Grieu F, Joseph D, Elsaleh H. A polymorphism in the enhancer region of the thymidylate synthase promoter influences the survival of colorectal cancer patients treated with 5-fluorouracil. Br J Cancer 2001;85:827-830.
8. Horie N, Aiba H, Oguro K, Hojo H, Takeishi K. Functional analysis and DNA polymorphism of the tandemly repeated sequences in the 5'-terminal regulatory region of the human gene for thymidylate synthase. Cell Struct Funct 1995;20:
191-197.
9. Mandola MV, Stoehlmacher J, Muller-Weeks S, et al. A nov- el single nucleotide polymorphism within the 5' tandem repeat polymorphism of the thymidylate synthase gene abo- lishes USF-1 binding and alters transcriptional activity.
Cancer Res 2003;63:2898-2904.
10. Lenz HJ, Leichman CG, Danenberg KD, et al. Thymidylate synthase mRNA level in adenocarcinoma of the stomach: a predictor for primary tumor response and overall survival. J Clin Oncol 1996;14:176-182.
11. Suda Y, Kuwashima Y, Tanaka Y, et al. Expression of thy- midylate synthase and thymidine phosphorylase in recurrence and survival rates of advanced gastric cancer. Gastric Cancer 1999;2:165-172.
12. Tajima Y, Shimoda T, Nakanishi Y, et al. Association of gastric and intestinal phenotypic marker expression of gastric carcinomas with tumor thymidylate synthase expression and response to postoperative chemotherapy with 5-fluorouracil. J Cancer Res Clin Oncol 2003;129:683-690.
13. Ishida Y, Kawakami K, Tanaka Y, Kanehira E, Omura K, Watanabe G. Association of thymidylate synthase gene poly- morphism with its mRNA and protein expression and with prognosis in gastric cancer. Anticancer Res 2002;22:2805- 2809.
14. Graziano F, Kawakami K, Watanabe G, et al. Association of thymidylate synthase polymorphisms with gastric cancer sus- ceptibility. Int J Cancer 2004;112:1010-1014.
15. Kawakami K, Omura K, Kanehira E, Watanabe Y. Polymor- phic tandem repeats in the thymidylate synthase gene is as- sociated with its protein expression in human gastrointestinal cancers. Anticancer Res 1999;19:3249-3252.
16. Zhang J, Cui Y, Kuang G, et al. Association of the thymi- dylate synthase polymorphisms with esophageal squamous
cell carcinoma and gastric cardiac adenocarcinoma. Carcino- genesis 2004;25:2479-2485.
17. Gonzalez CA, Riboli E, Badosa J, et al. Nutritional factors and gastric cancer in Spain. Am J Epidemiol 1994;139:466- 473.
18. Zhang ZF, Kurtz RC, Yu GP, et al. Adenocarcinomas of the esophagus and gastric cardia: the role of diet. Nutr Cancer 1997;27:298-309.
19. Cohen V, Panet-Raymond V, Sabbaghian N, Morin I, Batist G, Rozen R. Methylenetetrahydrofolate reductase polymor- phism in advanced colorectal cancer: a novel genomic pre- dictor of clinical response to fluoropyrimidine-based chemo- therapy. Clin Cancer Res 2003;9:1611-1615.
20. Kim JK, Kim S, Kim NK, et al. Polymorphisms of 5,10- methylenetetrahydrofolate reductase and risk of stomach can- cer in a Korean population. Anticancer Res 2005;25 (accepted in press).
21. Miao X, Xing D, Tan W, Qi J, Lu W, Lin D. Susceptibility to gastric cardia adenocarcinoma and genetic polymorphisms in methylenetetrahydrofolate reductase in an at-risk Chinese population. Cancer Epidemiol Biomarkers Prev 2002;11:1454- 1458.
22. Shen H, Xu Y, Zheng Y, et al. Polymorphisms of 5,10- methylenetetrahydrofolate reductase and risk of gastric cancer in a Chinese population: a case-control study. Int J Cancer 2001;95:332-336.
23. Choi JH, Lim HY, Nam DK, et al. Expression of thymidylate synthase in gastric cancer patients treated with 5-fluorouracil and doxorubicin-based adjuvant chemotherapy after curative resection. Br J Cancer 2001;84:186-192.
24. Maehara Y, Kusumoto T, Kusumoto H, et al. 5-fluorouracil and UFT-sensitive gastric carcinoma has a high level of thy- midylate synthase. Cancer 1989;63:1693-1696.
25. Moran RG, Spears CP, Heidelberger C. Biochemical deter- minants of tumor sensitivity to 5-fluorouracil: ultrasensitive methods for the determination of 5-fluoro-2'-deoxyuridylate, 2'-deoxyuridylate, and thymidylate synthetase. Proc Natl Acad Sci USA 1979;76:1456-1460.
26. Etienne MC, Chazal M, Laurent-Puig P, et al. Prognostic val- ue of tumoral thymidylate synthase and p53 in metastatic colorectal cancer patients receiving fluorouracil-based chemo- therapy: phenotypic and genotypic analyses. J Clin Oncol 2002;20:2832-2843.