Since Campbell and Boyd first developed a mold hemi- arthroplasty in 1940, the procedure for a total knee arthro- plasty has advanced greatly with the development of new materials and the increasing understanding of the knee joint biomechanics. Along with the advances in the prosthetic hardware, the recent development of the computer and navi- gation systems has led to the introduction of robotic surgery and computer-assisted surgery1,5,9,11,19). The long-term sur- vival rate of a total knee arthroplasty after a 10-year follow up was reported to be 80% to 95%7,14,17). Various factors affect this long-term survival, the most closely related factor being the physiologic recovery of the leg alignment8,16). Upon a follow-up study of more than 8 years, the loosening rate
was only 3% in those patients with a correctly recovered leg alignment, but was 24% in those with an incomplete recovery of the leg alignment4). There are limits on improv- ing the alignment accuracy using a conventional total knee arthroplasty19). Therefore, this study evaluated the effective- ness of a total knee arthroplasty using a computer-assisted navigation system and compared the accuracy of the leg alignment and component position using this navigation system with those using the manual alignment system.
MATERIALS AND METHODS
We examined 56 patients (76 cases) who underwent a total knee arthroplasty from January to June 2003. There were 7 men and 69 women, and the mean age of the patients was 68 years (range: 51-85 years). The procedure was to treat the primary osteoarthritis in all 76 cases. Group A includ- ed 40 cases operated on with the manual technique using an intramedullary femoral and extra- medullary tibial alignment
566 566
The Accuracy of Lower Extremity Alignment in a Total Knee Arthroplasty Using Computer-Assisted Navigation System
Jong Keun Seon, M.D., and Eun Kyoo Song, M.D.
Center for Joint Disease, Chonnam National University Hwasun Hospital, Jeonnam, Korea
566 566 Address reprint requests to
Eun Kyoo Song, M.D.
Center for Joint Disease, Chonnam National University Hwasun Hospital 160 Ilsim-ri, Hwasun-eup, Hwasun-gun 519-809, Korea
Tel: +82.61-379-7676, Fax: +82.61-379-7681 E-mail: [email protected]
Purpose: This study assessed the accuracy of the alignment of the lower extremity and the position of the components in a total knee arthroplasty (TKA), which was performed using a computer-assisted navi- gation system.
Materials and Methods: This study reviewed 40 TKA using a manual alignment system (group A) and 36 TKA using the Orthopilot��4.0 navigation system (group B). The radiographs taken 2 months after surgery were used to measure the femoro-tibial angle, the mechanical axis deviation, and the inclination of the femoral and tibial component. A value within the optimum±±3° was defined as an ‘acceptable’ and a value over the optimum±±3° was befined as an ‘outlier’.
Results: The coronal inclination of the femoral component to the anatomical femoral axis showed out- liers in 13 knees in group A and 1 knee in group B. The coronal inclination of the femoral component to the mechanical axis revealed 17 and 2 outliers in each group, respectively. The coronal inclination of the tibial component and sagittal inclination of femoral component showed no significant differences between two groups, but the sagittal inclination of tibial component showed 16 and no outlier in each group, respec- tively. Concerning the femoro-tibial angle, there were 9 outliers in group A and 2 outliers in group B. The mechanical axis deviation showed 9 and 2 outliers in groups A and B, respectively.
Conclusion: The navigation system helped to produce more ‘acceptable’ and less ‘outlier’ results than the manual alignment system. The alignment of the lower extremity after a TKA can be achieved more accurately using the navigation system.
Key Words: TKA, Navigation system, Alignment of lower extremity
system. Group B included 36 cases operated on with a navi- gation system (Orthopilot�, version 4.0). In both groups, the posterior cruciate ligament was retained and the patel- lar was not resurfaced. All the prostheses used for TKA were e-motion (Aesculap, Tuttligen, Germany) and were cemented.
The preoperative femoro-tibial angle (FTA) was 1.1±6.6° varus in group A and 2.5±2.5°varus in group B, showing no significant difference between the two groups (p=0.821).
For the TKA using the navigation system, the knee joint was exposed through the midvastus approach after incising the skin by approximately 10 cm in length. Subsequently, the femoral and tibial screws for transmitter attachment were placed. The femoral screw for the attachment of the transmitter was inserted into the medial cortex approximately 10 cm proximal to the knee joint, and the tibial screw was inserted into the antero-medial cortex approximately 8 cm distal to the tibial plateau. The transmitter used to monitor the ultraviolet camera of the main computer was attached to the proximal tibial region and the distal femur region.
After attaching the transmitter, the hip joint, ankle joint and knee joint were flexed for the Orthopilot�program to identify the midpoint of each joint. Using the probe, the locations of the medial and lateral joint surface of the prox- imal tibia, tibial spine, distal and posterior part of both femoral condyles, ankle center and medial and lateral malle- olus were registered. After the medial release in the proxi- mal tibia had been performed, the osteophyte, meniscus and anterior cruciate ligament were removed. After placing the
tibia cutting guide attached to a transmitter on the proxi- mal tibia, the suitable proximal tibia resection height, the anterior and posterior inclination were determined, and the cutting was then carried out after fixation with pins whilst observing the Orthopilot�screen. The extension gap and flexion gap were measured using a tensioner after the prox- imal tibial resection. Based on the measured values, the distal and posterior femur was then resected so that the two gap would form the same rectangle. The stability was confirmed after a trial insertion to determine the size of the meniscal component, and then the actual component was then inserted.
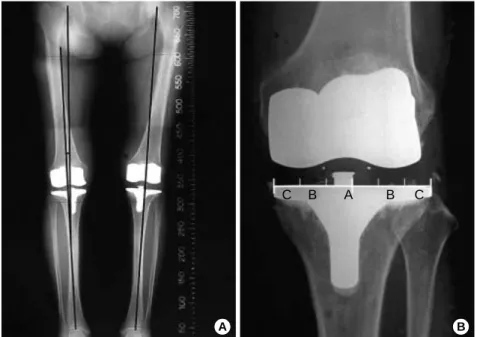
The radiographic indices with regard to the femoro-tib- ial angle, mechanical axis deviation and the inclination of the femoral and tibial component were evaluated at post- operative 2 months using the anteroposterior and lateral radiographs and the anteroposterior full-length weight bear- ing scanographs2)by two independent observers (Fig. 1, 2A).
The deviation in the mechanical axis from the center of the knee joint was also evaluated. After the joint surface had been divided into 3 sections (A, B and C) from the center,
‘‘A’’ was defined when the mechanical axis passed through the paracentral 1/3, ‘‘B’’ when the mechanical axis passed through the middle 1/3, and ‘‘C’’ when the mechanical axis passed out of the B region (Fig. 2B).
The outcome was defined ‘‘acceptable’’ when it was within the optimum value±3°and an ‘‘outlier’’ when it was over the optimum value±3°12).
Statistical analysis was performed to compare the differ-
A B C
Fig. 1.Diagrams showing the measure- ments of the inclination angle. (A) : The inclination angle of the femoral compo- nent is formed with the anatomical axis of the femur. : the inclination angle of the tibial component is formed with the mechanical axis of the tibia. (B) : Anoth- er inclination angle of the femoral compo- nent is formed with the mechanical axis of the femur. (C) : Angle of the femoral component is formed between the ana- tomical axis of the femur and is perpen- dicular line to prosthesis. : The angle of the tibial component is formed with the mechanical axis of the tibia.
ences between the two groups. An independent Student t- test was performed using SPSS for Windows Release 11.0 (SPSS, Chicago, Illinois). The confidence interval was 95%.
RESULTS
When the coronal inclination of the femoral component was measured on the anteroposterior radiographs, the angle ( , optimum=6°) formed with the anatomical axis of the femur showed 13 outliers (32.5%) in group A and 2 out- liers (2.8%) in group B. The mean value of this angle was 94.1±2.4°and 95.4±1.4°in groups A and B, respective- ly (p=0.001). The angle ( , optimum=90°) formed with the mechanical axis of the femur showed 17 outliers (42.5%) and 2 cases (5.6%) in groups A and B, respectively and the mean value of this angle was 87.1±2.4°and 88.7±1.7°, respectively in each group (p=0.006). In group A, the coro- nal inclination of the tibial component ( , optimum=90°) on the anteroposterior radiographs showed no outliers. The mean value was 90.4±1.1°and 90.7±0.8°in groups A and B, respectively (p=0.068). In group A, the femoro-tib- ial angle (optimum=7°) was 1.1±6.6°varus prior to surgery and 5.9±2.4°valgus after surgery. In group B, it was 2.5± 2.5°varus prior to surgery and 6.9±1.4°valgus after surgery.
The outlier outcome was present in 9 cases (22.5%) and 2 cases (5.6%) in groups A and B, respectively (p=0.001).
The mechanical axis (optimum=0°) on the weight bear- ing anteroposterior radiographs was 2.3±3.0°varus and
0.1±1.9°valgus in groups A and B, respectively. The out- come was 9 (22.5%) and 2 outliers (5.6%) in groups A and B, respectively (p=0.031). When the degree of the deviation in the mechanical axis was evaluated from the knee joint center the deviation was within the paracentral 1/3 in 34 cases (94.4%) in the navigation group and 22 (55%) in the manual group (p=0.001). No significant differences in the sagittal inclination of the femoral component ( ) from the lateral view were found between the two groups (p=0.161).
The lateral radiographs showed that there was an outlier in the inclination of the tibial component ( , optimum=90°) in 16 cases (40%) and 0 case in groups A and B, respectively.
The mean value was 87.8±2.1°and 90.0±0.9°in groups A and B, respectively (p<0.001).
The post-operative femoro-tibial angle (FTA), the mechani- cal axis deviation, the coronal inclination of the femoral component ( , ) and the sagittal inclination of the tibial component ( ) showed significant differences between the navigation and the manual group (Table 1, 2).
On the other hand, the coronal inclination of the tibial component on the anteroposterior radiographs and the sagit- tal inclination of the femoral component radiographs showed no significant difference between the two groups (Table 1, 2).
No infection or deep vein thrombosis was encountered as a complication. One case in the manual alignment group had a superficial wound infection at the incision site, which healed spontaneously.
Fig. 2.Diagrams showing mechanical axis deviations. (A) angle is formed between the mechanical axis of the femur and tibia.
(B) Deviation of the mechanical axis on the joint surface is divided into 3 sections.
‘‘A’’ was defined when the mechanical axis passed through the center 1/3, ‘‘B’’ when the mechanical axis passed through the middle 1/3, and ‘‘C’’ when the mechanical axis passed out of the B region.
A B
C B A B C
DISCUSSION
The long-term survival rate after a TKA after a 10-year follow-up was reported to range from 80 to 90%7,14,17). How- ever, various factors affect this survival rate, particularly the postoperative recovery of the proper leg alignment7,16).
Rand and Coventry15)reported a 10-year survival rate of 90% when the leg alignment was between 0°to 4°valgus, but it was 71% and 73% when it was higher than the 4° valgus and varus alignment, respectively. Jeffery et al.4) re- ported a 24% rate of prosthetic loosening when the mechan- ical axis was over ±3°deviation. The acceptable range for the postoperative leg alignment in a TKA is still controver- sial. However, a postoperative limb axis within a range of
±3°varus or valgus was found to be associated with a lower rate of aseptic component loosening in many studies4,15,16). Although an improvement in the mechanical alignment system can beachieved, the conventional implantation tech- nique fails to restore the mechanical limb axis within the range of ±3°of the varus or valgus in up to 30% of cases10,13). The potential errors in alignment result from the variations in the bony anatomy, a visual misjudgment by the surgeon and the general technical limitations.
Therefore, a computer-assisted navigation system was recently introduced in a TKA to improve the accuracy of the component position. The Orthopilot�, navigation system used in this study was easy to use and is currently approved by the Food and Drug Administration (FDA) after many
clinical studies in actual clinical settings. Mielke et al.10)ana- lyzed the results of the navigation assisted TKA compared with those of the conventional technique. They reported a tendency for a better leg alignment in the navigation TKA.
In the multicenter study6)on 555 TKAs, a significanty bet- ter postoperative leg alignment was performed the in navi- gation group than in the conventional group. The outlier rate (over ±3°) in the navigation group was 12% in the align- ment of the leg axis while it was 28% in the conventional group. This study found a similar outcome with regard to the femoro-tibial angle and mechanical axis deviation in that the outlier rate was 22.5% in the conventional group and 5.6% in the navigation group. These results were compara- ble to Han and Ha’s3)outlier results of 24% in the extrame- dullary and 28% in the intramedullary alignment system.
The data on the coronal femoral inclination ( , ) in conven- tional group had more outliers than in other reports 18,20). However, the reported outlier results in these inclinations vary widely. Laskin8)reported a 76% acceptable range in the intramedullary system and a 97% acceptable range in the extramedullary system.
A better alignment axis in the navigation group with regard to the femoro-tibial angle, the mechanical axis devi- ation and the coronal inclination of femoral component of this study was similar to the results of the other TKA per- formed with the navigation system6,10,18,19). On the other hand, the coronal inclination of the tibial component and the sagittal inclination of the femoral component, which showed no significant difference between the two groups were quite different from the other TKA performed with the navigation system6,10,18,19).
Even in the group treated with the computer-assisted navigation system, there were 2 outliers for the some radio- graphic parameters such as the femoro-tibial angle (FTA), the mechanical axis deviation, and the inclination of the femoral component. The factors that can induce inaccura- cies in a TKA using the image-free navigation system are
+, valgus; -, varus.
Radiological measurement Group A Group B p-value Femoro-tibial angle (°) +5.9±2.4 +6.9±1.4 0.005 Mechanical axis deviation (°) -2.3±3.0 +0.1±1.9 0.031 Mechanical axis deviation (No/%)
Central 1/3 22/55 34/94.4
Middle 1/3 8/20 2/5.6
Outer 1/3 10/25 0/0
Table 2.Radiological measurements of the leg alignment on the postoperative 2 months radiographs
Radiological measurement Group A (°) Group B (°) p-value
The coronal inclination of
Femoral component to anatomical axis ( ) 94.1±2.4 95.4±1.4 0.001
Femoral component to mechanical axis ( ) 87.1±2.4 88.7±1.7 0.011
Inclination of tibial component in coronal plane ( ) 90.4±1.1 90.7±0.8 0.068
Inclinination of tibial component in sagittal axis ( ) 87.8±2.1 90.0±0.9 0.000 Table 1.Radiological measurements of the prosthesis inclination on the postoperative 2 months radiographs
the many steps in the surgical technique. Among them, the most important factor appears to be the technical error in registration. Therefore, surgeons need make an effort to register the precise anatomical landmark in order to avoid a misalignment in the leg axis.
However, the follow-up of the navigated operation was too short to determine if the clinical outcome or survival rate had really improved. A longer follow-up will be need- ed to determine if this improvement in the accuracy of the alignment in the lower extremity and the navigation oper- ation lead to an increased long-term survival rate.
CONCLUSION
Compared with the manual alignment system, the navi- gation system helped to produce more ‘acceptable’ results and less ‘outlier’ results. The alignment of the lower extremity after a TKA can be more accurately achieved using the navi- gation system. Therefore, it is believed that an improvement in the lower extremity alignment will improve the long-term survival of the prosthesis.
REFERENCE
1. Delp SL, Stulberg SD, Davies BL, Picard F and Leitner F:
Computer assisted knee replacement. Clin Orthop, 354: 49-56, 1998.
2. Ewald FC: The knee society total knee arthroplasty Roentgenograph- ic evaluation and scoring system. Clin Orthop, 238: 9-12, 1989.
3. Han CD and Ha JW: Extremedullary versus intramedullary alignment guide systems in total knee arthroplasty. J of Korean Orthop Assoc, 32: 302-308, 1997.
4. Jeffery RS, Morris RW and Denham RA: Coronal alignment after total knee replacement. J Bone Joint Surg, 73-B: 709-714, 1991.
5. Jenny JY and Boeri C: Navigated implantation of total knee endo- prostheses-a comparative study with conventional instrumentation.
Z Orthop Ihre Grenzgeb, 139: 117-119, 2001.
6. Jenny JY, Mielke RK, Kohler S, et al: Total knee prosthesis implantation with a non-image-based navigation system-multicen- tric analysis. Proceedings 70th Annual Meeting AAOS: 96, 2003.
7. Knutson K, Lindstrand A and Lidgren L: Survival of knee arthroplasties, a nation-wide multicenter investigation of 8,000 cases.
J Bone Joint Surg, 68-B: 795-803, 1986.
8. Laskin RS: Alignment of total knee components. Orthopedics, 7:
62, 1984.
9. Matsen III FA , Garbini JL, Sidles JA, Pratt B, Baumgarten D and Kaiura R:Robotic assistance in orthopaedic surgery, A proof of principle using distal femoral arthroplasty. Clin Orthop, 296: 178-186, 1993.
10. Mielke RK, Clemens U, Jens JH and Kershally S: Naviga- tion in knee endoprosthesis implantation-preliminary experiences and prospective comparative study with conventional implantation technique. Z Orthop Ihre Grenzgeb, 139: 106-116, 2001.
11. Palombara PF, Fadda M, Martelli S and Marcacci M: Mini- mally invasive 3 Data registration in computer robot assisted total knee arthroplasty. Med Biol Eng Comput, 35: 600-610, 1997.
12. Perlick L, Bathis H, Perlick C, Luring C, Tingart M and Grif- ka J:Revision total knee arthroplasty : a comparison of postopera- tive leg alignment after computer-assisted implantation versus the conventional technique. J Knee Surg, Sports Trauma, Arthroscopy, 8 (in press), 2004.
13. Petersen TL and Engh GA: Radiographic assessment of knee alignment after total knee arthroplasty. J Arthroplasty, 3: 67-72, 1988.
14. Ranawat CS, Flynn WF, Saddler S, Hansraj KH and Mayn- hard MJ:Long-term results of total condylar knee arthroplasty. A 12-years survivorship study. Clin Orthop, 286: 94-102, 1993.
15. Rand JA and Coventry MB: Ten-year evaluation of geometric total knee arthroplasty. Clin Orthop, 232: 168-173, 1988.
16. Ritter MA, Faris PM, Keating EM and Meding JB: Postop- erative alignment of total knee replacement of total knee replacement its effect on survival. Clin Orthop, 299: 153-156, 1994.
17. Scuderi GR, Insall JN, Windsor RE and Moran MC: Sur- vivorship analysis of cemented knee replacement. J Bone Joint Surg, 71-B: 798-809, 1989.
18. Sparmann M, Wolke B, Czupualla H, Banzer D and Zink A: Positioning of total knee arthroplasty with and without naviga- tion support. A prospective, randomized study. J Bone Joint Surg, 85-B: 830-835, 2003.
19. Stulberg SD, Laon P and Sarin V: Computer-assisted naviga- tion in total knee replacement: Results of an initial experience in thirty-five patients. J Bone Joint Surg, 84-A (Suppl 1): 90-98, 2002.
20. Tillet ED, Engh GA and Petersen T: A comparative study of extramedullary and intramedullary alignment systems in total knee arthroplasty. Clin Orthop, 230: 176-181, 1988.
목 적: Computer-assisted navigation system을 이용한 인공 슬관절 치환술의 하지 정열 및 내고정물 위치의 정확도를 평 가하고자 하였다.
대상 및 방법: 고식적 방식(manual alignment system)을 이용한 40예(A군)와 navigation system을 이용한 36예(B군)를 방사선학적으로 비교 분석하였다. 수술 후 2개월에 시행한 방사선 촬영에서 대퇴 경골각, 기계적인 축, 대퇴 및 경골 삽입 물의 경사도를 정면 및 측면 사진에서 측정하였다. 결과 평가는 적정위치±3° 이내를‘양호(acceptable)’, 적정위치±3°
초과를‘불량(outlier)’으로 하였다.
결 과: 관상면에서 대퇴 삽입물의 경사도 측정시, 대퇴골의 해부학적 축과 이루는 각은 A군에서 불량이 13예와 B군에서 1 예이었다. 대퇴골의 기계적인 축과 이루는 각은 A군에서 17예, B군에서 2예이었다. 관상면에서 경골 삽입물의 경사도와 시상면에서 대퇴 삽입물의 경사도는 두 군간의 차이가 없었다. 시상면에서 경골 삽입물의 경사도는 A군에서 16예, B군에 서 0예이었다. 대퇴 경골각의 불량은 두군에서 각각 9예, 2예이었다. 체중 부하 전후면 사진에서 기계적인 축의 변위에 있 어 불량은 각각 9예, 2예로 navigation군에서 적은 오차가 관찰되었다.
결 론: Navigation system을 이용한 인공 슬관절 치환술은 기존방식에 비해‘양호’결과가 훨씬 많았으며, 불량은 적었다.
따라서 navigation system을 이용한 인공 슬관절 치환술은 정확한 하지 정렬을 얻을 수 있었으며, 인공 슬관절 치환술에 유용한 것으로 사료된다.
색인 단어: 인공 슬관절 치환술, Navigation system, 하지 정렬
네비게이션 시스템을 이용한 인공 슬관절 전치환술의 하지 정열의 정확도
선종근ㆍ송은규
화순 전남대학교병원 정형외과학교실