Decreased Bone Mineral density of Spine in Patients with Invasive Cervical Cancer
Hoon Choi, Min Hyung Jung1, Yong il Ji2, Hyeok Jung3, Ji Young Lee4, Won Jun Choi5, Ari Kim6, Jong Soon Choi7, Young Lim Oh8, Heung Yeol Kim8
Department of Obstetrics and Gynecology, School of Medicine, Sanggye Paik Hospital, Inje University, Seoul, Department of Obstetrics and Gynecology1, Kyung Hee Medical Center, Kyung Hee University, Seoul,
Department of Obstetrics and Gynecology2, Haeundae Paik Hospital, Inje University, Busan, Department of Obstetrics and Gynecology3, College of Medicine, Chosun University, Gwangju,
Department of Obstetrics and Gynecology4, School of Medicine, Konkuk University, Seoul, Department of Obstetrics and Gynecology5, School of Medicine, Gyeongsang National University, Jinju,
Department of Obstetrics and Gynecology6, College of Medicine, Wonkwang University, Gunpo, Department of Family Medicine7, Department of Obstetrics and Gynecology8, Kosin University, Busan, Korea
Objectives: To investigate the spinal bone mineral density (BMD) in patients with invasive cervical cancer without bone metastases.
Methods: We measured spinal bone mineral densities by dual-photon absorptiometry in 119 patients with invasive uterine cervical cancer and compared them with measurements from 135 control women.
Results: When adjusted for age, mean bone mineral density in patients with uterine cervical cancer was 13.9% lower (P=0.0003) and age-matched percentiles were 9.2% lower (P=0.0003) than in control women.
The deficits in bone mineral density and age-matched percentiles were confined to the uterine cervical cancer patients in their fifties.
Conclusions: Our study results suggest that patients with invasive cervical cancer have a lower spinal BMD, resulting in an increased risk of osteoporosis.
Key Words: Bone mineral density, Cervical cancer, Osteoporosis
Received: January 18, 2011 Revised: January, 2011 Accepted: February 17, 2011
Corresponding Author: Heung Yeol Kim, Department of Obstetrics
& Gynecology, College of Medicine, Kosin University, 34 Amnam-dong, Seo-gu, Busan 602-702, Korea
Tel: +82-51-990-6226, Fax: +82-51-990-3300 E-mail: [email protected]
Osteoporosis, basically defined as a decrease in bone mass, is a chronic disorder leading to enhanced bone fragility and a consequent increase in the risk of fractures even with little or no trauma.
The most debilitating osteoporotic fracture is hip fracture and the mortality rate is very high.1,2 As with other public health problems, it is important to identify
risk factors in order to prevent the disorder. It has been reported that a variety of neoplasms without bone metastasis produce circulating osteolytic factors that lead to bone destruction. However, only hypercalcemia and osteolytic bone metastasis have been regarded as the principal clinical consequences of increased bone resorption in these patients.3 There has been only one densitometric study of bone mineral density (BMD) by dual-photon absorptiometry (DPA) in patinets with cervical cancer.4
However, in recent decades, bone densitometry with dual-energy X-ray absorptiometry (DXA) has been
Table 1. Characteristics of the study subjects
Characteristic Control (N=135) Cervical cancer (N=119) P value
Age (year) Weight (kg) BMI
Menopause duration (day) Serum clacium (mg/dL) Serum phosphate (mg/dL)
53.0±11.3 56.1±8.3 23.0±4.1 7.3±7.3 9.9±1.7 5.4±1.1
52.6±11.1 57.2±9.1 24.4±4.3 6.9±6.2 9.1±1.7 5.3±1.7
P>0.05 P>0.05 P>0.05 P>0.05 P>0.05 P>0.05 BMI: body mass index
found to be more accurate than DPA, and it has been extensively developed to replace DPA and used to evaluate BMD.5 In the present study, we investigated the possibility that spinal bone mineral density of patients with uterine cervical cancer is reduced compared with that in control women.
MATERIALS AND METHODS
We studied 119 patients with uterine cervical cancer and 135 control women. Cases were selected from among all uterine cervical cancer patients admitted to the department of obstetrics and gynecology of Sanggye Paik Hospital, Kosin and Kyunghee University Hospital from March 2007 to October 2009, and had previously untreated (chemotherapy, radiotherapy, radical hysterec- tomy, and bilateral salpingooophorectomy) invasive cervical cancer. According to the International Fede- ration of Gynecology and Obstetrics (FIGO) staging classification, the numbers of patients in stages I, II and III were 39, 44, 36. Cervical cancer was diagnosed by histologic confimation.
Control volunteer subjects were recruited from women who visited the Sanggye Paik Hospital, Kosin and Kyunghee University Hospital for Papanicolaou smear screening during the same time period. Those with cervical intraepithelial neoplasia were excluded.
Based on screening by medical history and physical examination, all subjects were free of disease and were not using drugs known to influence bone and calcium metabolism. We excluded women with premature
menopause and postmenopausal women who were not on estrogen replacement therapy. Height and weight were measured and body mass index (kg/m2) was calculated on the scanning day; all subjects under 40 kg and over 105kg were excluded.
Measurements of serum calcium, phosphate, alkaline phosphatase, and creatinine were performed on all patients and control women on the scanning day.
Menopause duration could be calculated from only 40 patients with uterine cervical cancer and 65 control women who remembered their menopause date exactly.
All patients had dual-photon absorptiometry of the lumbar spine (Lunar DP4, Madison, WI). The results were expressed as bone mineral density and as percentiles of controls matched for age, sex, weight, and ethnic background. Bone mineral density was measured by one observer without knowledge of the patient's condition. The bone scanner used was properly calibrated according to the three-chamber standard provided with the instrument. Measurements on this standard phantom gave values within 1% of those expected. In eight control subjects, the variation between two separate scans at a 2-week interval was 2.4%. A gadolinium 153 source was changed annually.
Although the gadolinium source was changed once during the study period, the patients and controls were measured at the same time.
Statistical tests included Student t test, analysis of variance, and analysis of covariance, as appropriate.
Bone mineral density in both groups was compared by analysis of covariance before and after adjusting for
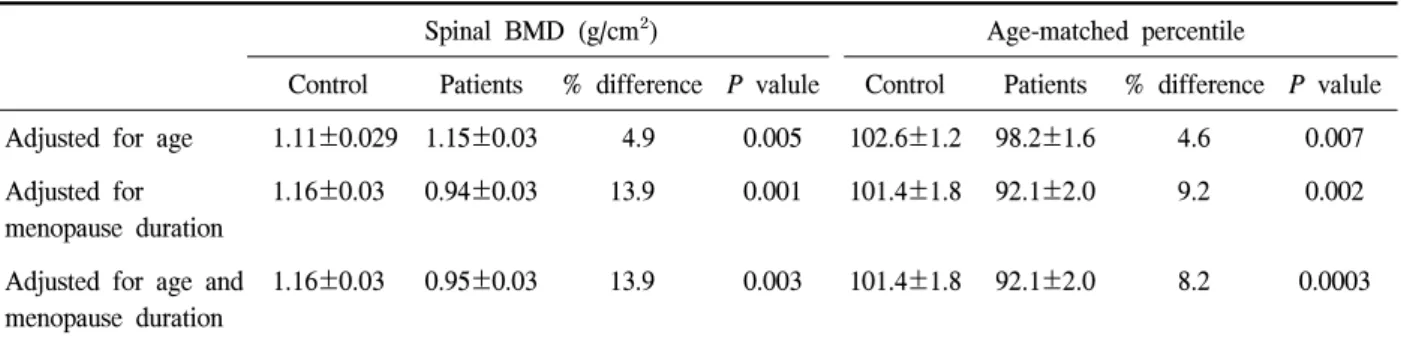
Table 2. Spinal BMD and age-matched percentiles adjusted for age and menopause duration
Spinal BMD (g/cm²) Age-matched percentile
Control Patients % difference P valule Control Patients % difference P valule Adjusted for age 1.11±0.029 1.15±0.03 4.9 0.005 102.6±1.2 98.2±1.6 4.6 0.007 Adjusted for
menopause duration
1.16±0.03 0.94±0.03 13.9 0.001 101.4±1.8 92.1±2.0 9.2 0.002
Adjusted for age and menopause duration
1.16±0.03 0.95±0.03 13.9 0.003 101.4±1.8 92.1±2.0 8.2 0.0003
BMD: bone mineral density; Data are presented as Mean±Standard deviation
Table 3. Spinal BMD and age-matched percentiles by age in decade
Number BMD (g/cm²) Age-matched percentile
Age (year) Control Patients Control Patients Control Patients
30~39 40~49
*50~59 60~69
23 (0) 30 (14) 46 (44) 36 (37)
19 (1) 26 15
42 (27) 32 (22)
1.28 1.17 1.09 0.89
1.22±0.03 1.11±0.03 0.98±0.02 0.79±0.03
107.6±3.7 105.6±2.0 104.9±1.8 92.5±2.2
104.1±3.2 109.1±3.0 90.8±2.4 88.2±3.8 BMD: bone mineral density; Data are presented as Mean±Standard deviation; Numbers in parentheses indicate post- menopausal women, including those who did not remember their menopause date exactly; *P=0.0005 by Student t test.
age and menopause duration. Data were considered statistically significant at P<0.05.
RESULTS
Age, weight, body mass index, menopause duration, and serum calcium and phosphate were not significantly different between controls and uterine cervical cancer patients (Table 1). All patients and control women had normal values for serum calcium, phosphate, creatinine, and alkaline phosphatase.
Mean bone mineral density and age-matched percen- tiles adjusted for age and menopause duration were, respectively, 13.9 and 9.2% lower in uterine cervical cancer patients than in control women (Table 2). When analyzed by age in decades (Table 3), spinal bone mineral density in uterine cervical cancer patients younger than 50 was not significantly decreased, but it was for patients in their fifties. Age-matched percentiles
were also significantly decreased only in these patients compared with controls.
Age-matched percentiles in uterine cervical cancer patients with stages I, II, and III disease were 100.9±2.8, 98.3±2.6, and 94.1±2.3. By analysis of variance, no significant differences were found accor- ding to the stage of disease. This may be due in part to the limited number of cases in each stage.
DISCUSSION
Cervical cancer is a major world health problem for women. It is the third most common cancer in women worldwide. In Korea, it comprises 9.1% of cancer in women and is the fifth most common cancer in women. The yearly incidence in Korea for 2004 was 3148.1 Relatively high remission and long-term survival rates can now be achieved. Quality of life is increa- singly important to long-term survivors of cervical
cancer and one of the major quality-of-life issues is osteoporosis.
An association between cervical cancer and reduced BMD has been observed previously in only one study by DPA.4 Our preliminary results indicated that patients with cervical cancer without bone metastases showed significantly lower BMD than control women.
It is possible that the initial menopausal loss was greater in patients with cervical cancer. Several studies have shown that accelerated bone loss occurs in the first few years after menopause and cervical cancer may increase this loss.1,6,7 However, in our study, no patient with premature menopause was found in both groups.
Why should patients with cervical cancer have decreased BMD before menopause? Human cancer cell lines can secrete a bone resorption stimulatory pep- tide.8,9 Several factors, including prostaglandins, trans- forming growth factor, osteoclast activating factor and parathyroid hormone-like peptide, have been causally implicated in the activation of osteoclasts by tumor cells.8-10 In addition, quantitative histochemical studies of the bone revealed a reduction in the volume of trabecular bone, greater osteoclastic activity and mar- kedly reduced osteoblastic surface in patients with malignancy.11,12 Therefore, most previous studies focused on bone resorption-associated hypercalcemia in malig- nancy combined with bone metastases.3 If the reduced BMD observed in our study had resulted from the production of bone resorption substances, than we would have expected patients to show hypercalcemia, but no hypercalcemia was seen in our patients with cervical cancer without bone metastases. It is possible that calcium reflux from bone is not abnormal, but the derangement may have been too subtle to be detected.
Another possibility is that some cases of malignany were associated with elevated bone resorption substances even in the absence of hypercalcemia, because of regulatory mechanisms that maintain normocalcemia.13 In agreement with our study, Lerner
and Ljungberg14 reported that fresh renal cell carcinoma tissue from normocalcemic patients also stimulates bone resorption in vitro. Therefore, the decreased BMD in our patients with cervical cancer without bone metastases is probably due to a variety of factors.1 The finding of bone loss in patients with cervical cancer is important, for it may imply that patients with cervical cancer have an increased risk of developing osteoporosis.
REFERENCES
1. Hung YC, Yeh LS, Chang WC, Lin CC, Kao CH.
Prospective study of decreased bone mineral den- sity in patients with cervical cancer without bone metastases: a preliminary report. Jpn J Clin Oncol 2002;32:422-4.
2. Lindsay R. Prevention of postmenopausal osteo- porosis. Obstet Gynecol Clin North Am 1987;14:
63-76.
3. Mundy GR, Ibbotson KJ, D'Souza SM, Simpson EL, Jacobs JW, Martin TJ. The hypercalcemia of cancer. Clinical implications and pathogenic mecha- nisms. N Engl J Med 1984;310:1718-27.
4. Cho SH, Lee JA, Moon H, Kim DS. Reduced spinal bone mass in patients with uterine cervical cancer. Obstet Gynecol 1991;78:689-92.
5. Sartoris DJ, Resnick D. Dual-energy radiographic absorptiometry for bone densitometry: current status and perspective. AJR Am J Roentgenol 1989;152:
241-6.
6. Nilas L, Christiansen C. Rates of bone loss in normal women: evidence of accelerated trabecular bone loss after the menopause. Eur J Clin Invest 1988;18:529-34.
7. Lee SH, Ku CH, Lee KB, Shin JW, Park CY.
Decreased bone mineral density of femur in patients with cervical cancer. J Obstet Gynaecol Res 2009;35:335-8.
8. Strewler GJ, Stern PH, Jacobs JW, Eveloff J, Klein
RF, Leung SC, et al. Parathyroid hormonelike protein from human renal carcinoma cells. Struc- tural and functional homology with parathyroid hormone. J Clin Invest 1987;80:1803-7.
9. Suva LJ, Winslow GA, Wettenhall RE, Hammonds RG, Moseley JM, Diefenbach-Jagger H, et al. A parathyroid hormone-related protein implicated in malignant hypercalcemia: cloning and expression.
Science 1987;237:893-6.
10. Moseley JM, Kubota M, Diefenbach-Jagger H, Wettenhall RE, Kemp BE, Suva LJ, et al. Para- thyroid hormone-related protein purified from a human lung cancer cell line. Proc Natl Acad Sci U S A 1987;84:5048-52.
11. Roodman GD. Mechanisms of bone lesions in multiple myeloma and lymphoma. Cancer 1997;
80:1557-63.
12. Troyer H, Sowers JR, Babich E. Leydig cell tumor
induced hypercalcemia in the Fischer rat: morpho- metric and histochemical evidence for a humoral factor that activates osteoclasts. Am J Pathol 1982;
108:284-90.
13. Henderson JE, Shustik C, Kremer R, Rabbani SA, Hendy GN, Goltzman D. Circulating concentrations of parathyroid hormone-like peptide in malignancy and in hyperparathyroidism. J Bone Miner Res 1990;5:105-13.
14. Lerner UH, Ljungberg B. Renal cell carcinoma in tissue culture secretes nondialyzable product that stimulates bone resorption in organ-cultured mouse calvaria. J Bone Miner Res 1989;4:365-77.
15. Dawson-Hughes B, Tosteson AN, Melton LJ, 3rd, Baim S, Favus MJ, Khosla S, et al. Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporos Int 2008;19:449-58.