1가톨릭대학교 의과대학 서울성모병원 신경외과학교실, 2가톨릭대학교 의과대학 서울성모병원 이비인후과학교실
이민기
1, 박재성
1, 김도현
2, 김성원
2, 전신수
1, 홍용길
11Departments of Neurosugery, Seoul St. Mary’s Hospital, The Catholic University of Korea, Seoul, Korea
2Departments of Otorhinolaryngology-Head and Neck Surgery, Seoul St. Mary’s Hospital, The Catholic University of Korea, Seoul, Korea
Min-Gi Lee
1, Jae-Sung Park
1, Do Hyun Kim
2, Sung Won Kim
2, Sin Soo Jeun
1, Yong-Kil Hong
1내시경을 이용한 경접형동 접근 수술 중에 시행한 비강내 세균 배양 검사 및 그에 대한 항생제 감수성 결과 분석과 3세대 세팔로스포린의 예방적 항생제로서의
임상적 효과에 대한 분석
J Korean Skull Base Society 13권 2호 : 18~27, 2018
종설1 종설2 원저1
증례1 원저2
증례2 증례3 증례4 증례5
Background : We analyzed the distribution of identified micro-organisms from the nasal cavity during EETS and their antibiotic susceptibility testing (AST) results. In addition, we evaluated the clinical outcomes of antibiotic prophylaxis with third-generation cephalosporins for endoscopic transsphenoidal surgery.
Methods : From November 2014 to October 2017, a total of 225 EETS cases with available nasal cavity culture results were reviewed to identify the clinical data relevant to CNS infection.
Ceftriaxone was used for antibiotic prophylaxis, and the patients were divided into subgroups according to the AST results.
Results : Gram-positive cocci were the most commonly identified micro-organisms. The patient population was divided into the following three groups: prophylaxis-appropriate, prophylaxis-inappropriate, and Undetermined group, each amounting to 132 (59.5%), 34 (15.3%), and 56 (25.2%) cases, respectively. CNS infection was observed in 2 (0.9%) cases.
But, statistical analyses did not show significant differences in the occurrence of CNS infection among the studied groups.
Conclusions : Antibiotic prophylaxis with third-generation cephalosporins showed that most (85%) patients received appropriate prophylaxis, and the clinical outcomes regarding the CNS infection were also comparable to other previous reports. Future larger-scale studies are mandatory to establish the relationship between prophylaxis-appropriateness and the occurrence of CNS infection.
Analysis of intraoperative nasal cavity culture with the antibiotics susceptibility test and clinical outcomes of antibiotic prophylaxis with third-generation
cephalosporins for endoscopic transsphenoidal surgery
논문 접수일 : 2018년 8월 5일 논문 완료일 : 2018년 8월 30일
주소 : Department of Neurosurgery, Seoul St.
Mary’s Hospital, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea
Tel : +82-2-2258-6777 Fax : +82-2-594-4248 E-mail : [email protected]
Jae-Sung Park
교신저자
Endoscopy, Antibiotic prophylaxis, Nasal cavity, Ceftriaxone Key Words
▒ INTRODUCTION
Transsphenoidal surgery is a safe and effective route of surgery for most parasellar lesions. In addition, by the benefit of recent advances in surgical skills and instruments.[1,2]
endoscopic endonasal transsphenoidal surgery (EETS) has become an alternative popular surgery route as well. Regarding the outcomes of microscopic and endoscopic surgeries, most recent studies report no difference between the two surgical modalities.[3,4] However, some reports suggested that endoscopic approaches are associated with a higher incidence of postoperative complications than microscopic approaches.[1]
This difference in outcomes can be attributed to the fact that, owing to recent advances of endoscopic surgical techniques,[5]
they enabled the skull base surgery to be more extensive.[6] In this context, it is necessary to elaborate adequate management strategies to prevent complications before and after surgery.
Appropriate use of antibiotic prophylaxis is a crucial measure to minimize the infectious complications. However, with regard to functional endoscopic sinus surgeries, there is no concrete evidence that intravenous (IV) antibiotic prophylaxis is necessary,[7] and this is considered to be the common belief among rhinology surgeons.[8] As demonstrated in a recent report, the patients with culture-inappropriate postoperative antibiotic therapy had a significantly less quality of life improvement as compared to the patients with culture-
appropriate therapy following endoscopic sinus surgery for chronic rhinosinusitis.[9] On the other hand, while the necessity of perioperative antibiotics is recognized in the endoscopic skull base surgeries;[10,11] there is no widely accepted ideal antibiotic chemoprophylaxis regimen. In this respect, the use of third-generation cephalosporins with or without aminoglycoside was reported to be associated with a very low rate of infectious complications.[10]
In the present study, we examined the culture findings extracted from the intraoperative field and the clinical outcomes of antibiotic prophylaxis with third-generation cephalosporins for endoscopic transsphenoidal surgeries.
▒ METHODS
1. Treatment protocols
A standardized critical pathway (CP) for the patients requiring EETS cases was developed and has been applied since November 2014. Routine imaging study, hormonal status evaluation, as well as ophthalmologic and rhinologic assessment were performed preoperatively. The intraoperative swab culture procedure from the nasal cavity was included during the nasal phase, whereby the culture was taken from the middle turbinate or the nasal septum mucosa. Thereafter, bacterial culture was performed along with antibiotic susceptibility testing (AST).
Table 1. Patient subgroups according to the identified micro-organisms and their antibiotic susceptibility testing results to ceftriaxone
Group Definition Corresponding Bacterial Species
Prophylaxis- Appropriate
One of the following criteria is satisfied for all the identified micro- organisms:
1) No identified bacterial organism,
2) ceftriaxone-susceptible isolates confirmed with AST results, or 3) identified organism usually known as ceftriaxone-susceptible
GPCs - MSCoNS, MSSA, ceftriaxone-susceptible S.
pneumoniae, viridans group Streptococcia) (S. Viridans, alpha-hem, S. parasanguinis)
GNBs - ESBL negative Enterobacteriaceae (E. Coli, E.
aerogenes), ceftriaxone-susceptible H. influenzae Prophylaxis-
Inappropriate At least 1 identified organism is confirmed resistant to ceftriaxone GPCs (MRCoNS, MRSA), GPBs (Corynebacterium sp., Bacillus sp.), NFBs (P. aeruginosa), anaerobes
Undetermined
None of the identified organism is confirmed resistant to ceftriaxone, and at least 1 identified organism does not have available AST results
GPCs (CoNS, S. aureus, S. pneumoniae), GNBs (E.
aerogenes); without AST results
AST: antibiotic susceptibility testing, GPC: gram-positive cocci, MSCoNS: methicillin-susceptible coagulase-negative Staphylococcus, MSSA: methicillin- sensitive Staphylococcus aureus, GNB: gram-negative bacilli, ESBL: extended-spectrum beta-lactamase, MRCoNS: methicillin-resistant coagulase-negative Staphylococcus, MRSA: methicillin-resistant Staphylococcus aureus, GPB: gram-positive bacilli, NFB: non-fermenting gram-negative bacilli, CoNS: coagulase- negative Staphylococcus.
a)Viridans group streptococci are usually known as ceftriaxone-susceptible, even without AST results.
The cultures were collected with an ESwab Collection and Transport System (Copan Italia, Brescia, Italy). For aerobes, sheep blood (5%), chocolate, and MacConkey agar plates were inoculated at 37°C aerobically (MacConkey) and under 5%
carbon dioxide (blood and chocolate) and then examined at 24 and 48 hours.[12] For anaerobes, the samples were plated on a Brucella agar supplemented with 5% sheep blood, vitamin K, and hemin. The plates were then incubated anaerobically for 4 days and examined after 24 hours, 48 hours, and 4 days.[13] If bacterial growth was observed, aero tolerance testing was conducted. To identify aerobes and anaerobes, standard methods were used, and AST was performed based on the performance standards of the Clinical and Laboratory Standards Institute.[14]
The antibiotic prophylaxis already in use was maintained unless the patient had clinical signs of central nervous system (CNS) infection confirmed by laboratory results. The ceftriaxone was used as a primary antibiotic prophylaxis.
For the patients with an adverse reaction to ceftriaxone, ceftazidime was used. Antibiotic prophylaxis was administered IV (2 g daily) during the patients’ hospital stay and then replaced by oral 3rd generation cephalosporin agents (Cefditoren 300 mg daily) for additional 7 to 10 days until the next hospital visit. According to our EETS CP, the duration of hospital stay varied by the usage of the nasoseptal flap. The duration of hospital stay was 6 days for the patients who did not apply the nasoseptal flap and 8 days for those who applied it.
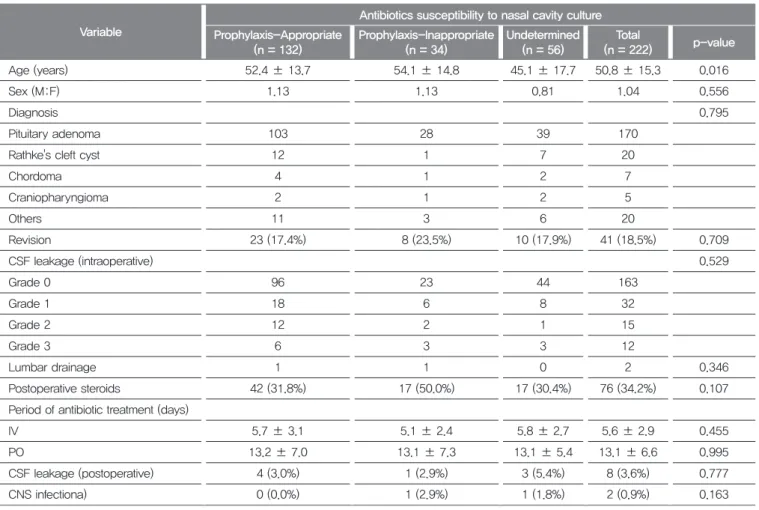
Table 2. Relationship of patient variables between antibiotics coverage groups
Variable
Antibiotics susceptibility to nasal cavity culture Prophylaxis-Appropriate
(n = 132)
Prophylaxis-Inappropriate (n = 34)
Undetermined (n = 56)
Total
(n = 222) p-value
Age (years) 52.4 ± 13.7 54.1 ± 14.8 45.1 ± 17.7 50.8 ± 15.3 0.016
Sex (M:F) 1.13 1.13 0.81 1.04 0.556
Diagnosis 0.795
Pituitary adenoma 103 28 39 170
Rathke's cleft cyst 12 1 7 20
Chordoma 4 1 2 7
Craniopharyngioma 2 1 2 5
Others 11 3 6 20
Revision 23 (17.4%) 8 (23.5%) 10 (17.9%) 41 (18.5%) 0.709
CSF leakage (intraoperative) 0.529
Grade 0 96 23 44 163
Grade 1 18 6 8 32
Grade 2 12 2 1 15
Grade 3 6 3 3 12
Lumbar drainage 1 1 0 2 0.346
Postoperative steroids 42 (31.8%) 17 (50.0%) 17 (30.4%) 76 (34.2%) 0.107
Period of antibiotic treatment (days)
IV 5.7 ± 3.1 5.1 ± 2.4 5.8 ± 2.7 5.6 ± 2.9 0.455
PO 13.2 ± 7.0 13.1 ± 7.3 13.1 ± 5.4 13.1 ± 6.6 0.995
CSF leakage (postoperative) 4 (3.0%) 1 (2.9%) 3 (5.4%) 8 (3.6%) 0.777
CNS infectiona) 0 (0.0%) 1 (2.9%) 1 (1.8%) 2 (0.9%) 0.163
The data is presented as mean ± standard deviation or n (%).
M: male, F: female, CSF: cerebrospinal fluid, IV: intravenous, PO: per os, CNS: central nervous system.
a)Only cases with confirmative CSF results were included.
The surgical procedure was addressed as a purely endoscopic endonasal approach via the binostrils 3 or 4 hands technique.
The rhinology surgeon performed surgery in the nasal and sphenoid stage. In the beginning of the surgery, a modified
“rescue” flap was prepared for the nasoseptal mucosa and harvested when needed for sellar floor reconstruction.[15]
Thereafter, the neurosurgeon took over the next procedure from the sellar stage to removal of the mass. Sellar floor reconstruction was performed by both surgeons. The graded repair technique was used according to the degree of intraoperative cerebrospinal fluid (CSF) leakage, as reported in detail in our previous report.[16] The absence of intraoperative CSF leakage was confirmed under Valsalva maneuver after the reconstruction.
2. Study design
The present study was approved by the Institutional Review Board of our institution (KC18RESI0309), and the requirement for informed consent was waived given the retrospective nature of our research. From November 2014 to October 2017, the culture results from the nasal cavity among a total of 225 cases were obtained. A retrospective medical chart review was performed to identify patient demographics (age and sex), pathologic diagnoses, usage of the perioperative antibiotics, nasal cavity culture results, previous medical history, duration of IV and per os (PO) antibiotics, insertion of lumbar drain, use of post-operative steroids, intraoperative CSF leakage grades, presence of postoperative CSF leakage, and CSF- confirmed CNS infection. The intraoperative CSF leakage was graded by the method suggested by Esposito et al. [17] (Grade 0, no leak observed; Grade 1, small leak without obvious diaphragmatic defect; Grade 2, moderate leak; or Grade 3, large diaphragmatic/dural defect), and the CNS infection was described only on the basis of a positive CSF study. The cases associated with a predisposing CNS infection were excluded from the present study (3 cases).
According to the identified micro-organisms and their AST results, the surgical cases were divided into three groups (Table 1). The classification was based on the classification proposed
by Zhang et al.[9] which was modified to better reflect our results. The final classification was adjusted and confirmed by our Division of Infectious Diseases, Department of Internal Medicine.
3. Statistical analyses
For numeric variables such as age and period of antibiotic usage (IV and PO), one-way ANOVA was performed. For categorical data, Pearson’s χ2 test (Fisher’s exact test) was performed. Logistic regression analysis was performed to investigate the risk factors for developing CNS infection. All p values of less than 0.05 were considered to indicate statistical significance.
All statistical analyses were conducted using the PASW 18.0 software (SPSS Inc., Chicago, IL, USA).
▒ RESULTS
1. Analysis of identified microbial species and antibiotics susceptibility
While 92 (41.7%) cases showed a negative growth from the nasal cavity, more than 2 micro-organisms were identified in 45 (20.4%) cases (Fig. 1A). Among the identified micro- organisms, gram-positive cocci (GPC) were most commonly found, followed by gram-negative bacilli (GNB) and gram- positive bacilli (GPB) (Fig. 1B).
The composition of the GPC, GNB, and GPB groups is shown in Fig. 1C. For GPCs, Staphylococcus species were most commonly identified; methicillin-resistant strains were recognized as well. For GNBs, Enterobacter aerogenes (E. aerogenes) were most commonly found.
Interestingly, these species were susceptible to ceftriaxone, but resistant to second-generation cephalosporins. For GPBs, Corynebacterium species, which are known to be resistant to ceftriaxone, were most commonly found.
The distribution of micro-organisms was schematized in the order of identified counts (Fig. 2A). Coagulase- negative Staphylococci (CoNS) including Staphylococcus epidermidis were most common, followed by Corynebacterium
species, E. aerogenes, methicillin-sensitive Staphylococcus aureus, methicillin-resistant Staphylococcus epidermidis (MRSE), Streptococcus viridans, and methicillin-resistant Staphylococcus aureus (MRSA). Methicillin-resistant strains amounted to 9% of the identified micro-organisms.
Distribution according to the AST results is shown in Fig. 2B. The identified counts for prophylaxis-appropriate (PA) group, prophylaxis-inappropriate (PI) group, and Undetermined group were 132 (59.5%), 34 (15.3%), and 56 (25.2%) cases, respectively.
2. Clinical outcomes of antibiotic prophylaxis with third- generation cephalosporins, including the occurrence of CNS infection
In the present study, total postoperative CSF leakage rate was 3.6% (8 cases), and CNS infection rate was 0.9% (2 cases).
With a similar rate of postoperative CSF leakage in PA (3.0%) and PI (2.9%) groups, CNS infection occurred only in the PI group. However, this finding was statistically insignificant (p=0.163) (Table 2).
In order to determine whether the prophylaxis- appropriateness affects the clinical outcomes, including the occurrence of CNS infection, we analyzed the relationship of patient variables among the three groups. The patients’
age was the only factor which was significantly lower in the undetermined group than in the PA or PI groups. Other variables did not yield statistically significant differences among the groups.
The results of a logistic regression analysis for the variables attributed for CNS infection showed that none of the variables showed clinical relevance to CNS infection in univariate analysis.
3. Case summary of the CNS infection cases
Since our analysis did not show inter-group difference in the occurrence of CNS infection, 2 cases with CNS infection are presented in detail, and some of their common features are discussed.
A 31 year-old male with a prior treatment history
of transcranial approach and adjuvant radiation (5,400 cGy/30 Fx) to the surgical field (Fig. 3A) for the unveiled craniopharyngioma was admitted to our hospital. Due to hypopituitarism from the previous surgery, the patient was taking hydrocortisone. In the perioperative period, the steroid dosage was temporarily increased and then gradually tapered to the physiologic dosage. The patient’s culture results from the nasal cavity revealed the growth of CoNS without available AST results (Undetermined group). Probably due to the patient’s prior history of transcranial approach, which rendered an adhesion in the sellar space, Grade 3 intraoperative CSF leakage occurred during EETS. After total mass removal, the sellar floor reconstruction was performed according to our graded repair protocol [16] using artificial dura. Lumbar drainage was not installed after surgery.
Ceftazidime was administered (due to hypersensitivity to ceftriaxone) for IV antibiotics, which was maintained for 7 days. Afterwards, PO antibiotics were administered for 9 days. However, 24 days after surgery, the patient visited our emergency room complaining of headache, fever, and CSF rhinorrhea, which subsequently required a revision surgery.
Vancomycin and cefepime were prescribed and maintained for four weeks. Although the CSF culture for the growth of any micro-organisms was negative, the cell count of the CSF showed increased white blood cell (WBC) levels with elevated protein and decreased glucose level, implying bacterial meningitis. A strain of MRSE was incubated from the mucosa of the patient’s nasal cavity during the revisional surgery.
And the next case was a 28 year-old female patient with a craniopharyngioma whose presenting symptom was depression (Fig. 3B). On magnetic resonance imaging, the mass which resided in the sellar and suprasellar area was disclosed. It was inevitable to resect the pituitary stalk, which the tumor was based on, thus she required a hormonal replacement medication after surgery. Her nasal cavity culture result showed the growth of MRSA (PI group). Since most lesions were located in the suprasellar area, Grade 3 intraoperative CSF leakage occurred after tumor removal. Sellar floor reconstruction was performed according to our graded repair
protocol,[16] and the patient’s fascia lata was used as a dural substitute. Lumbar drainage was performed as an adjunctive to cease the leakage of CSF and maintained for 7 days. On day 11 after surgery, the patient developed fever; therefore, following the instructions of the Division of Infectious Disease, the IV antibiotics regime was replaced by vancomycin and cefepime. However, CSF rhinorrhea developed several days later, requiring a revision surgery. The additional IV antibiotic treatment was necessary for approximately four weeks. The CSF findings were similar to those of the first patient. The WBC count increased with elevated protein and decreased glucose level; however, the CSF culture did not show any
micro-organisms. An additional nasal cavity culture was not performed in the revision surgery.
▒ DISCUSSION
1. Analysis of the nasal cavity culture results
In the results, 58% of the patients showed positive culture findings. Most of the identified species were susceptible to ceftriaxone. However, the methicillin-resistant Staphylococcus species and GPBs (Corynebacterium species and Bacillus species), were not responsive to the ceftriaxone. The growth of these micro-organisms was identified in 15.3% of the study
Fig. 1
A B
C
Characteristics of identified micro-organisms. (A) Identified number of colonized micro-organisms in each patient.
Approximately 60% of the patients showed positive culture results, while 20% showed 2 or more identified micro-organisms. (B) Distribution of colonized micro- organisms according to the groups. Gram-positive cocci (GPC) was the most commonly identified micro-organism, followed by gram-negative bacilli (GNB), gram-positive bacilli (GPB), and anaerobes. (C) Composition of the most common groups. In the GPC group, coagulase- negative Staphylococcus (CoNS)* and methicillin- sensitive Staphylococcus epidermidis (MSSE) were the most common micro-organisms. In the GNB group, E.
aerogenes was the most common micro-organism, followed by Klebsiella sp. and E.coli. In the GPB group, Corynebacterium sp. was most common. MSSA:
methicillin-sensitive Staphylococcus aureus, MRSE:
methicillin-resistant Staphylococcus epidermidis, MRSA:
methicillin-resistant Staphylococcus aureus. *CoNS without antibiotic susceptibility testing results.
Fig. 2
A B Identified microbial species and subgroup distribution.
(A) Micro-organisms in the order of identified counts.
Coagulase-negative Staphylococcus (CoNS)* and methicillin-sensitive Staphylococcus epidermidis (MSSE) were the most commonly identified micro-organisms.
(B) Subgroup distribution of identified micro-organisms according to the antibiotic susceptibility testing results to ceftriaxone. MSSA: methicillin-sensitive Staphylococcus aureus, MRSE: methicillin-resistant Staphylococcus epidermidis, MRSA: methicillin-resistant Staphylococcus aureus. *CoNS without antibiotic susceptibility testing results.
population. In the present study, AST was not performed by our microbiologists for most CoNS isolates, as this microbe is a component of the normal flora in the nasal cavity and has a lower pathological potency. However, this suggests that the potential number of methicillin-resistant CoNS could have been overlooked.
Our results demonstrated that the proportion of revision cases was slightly higher in the PI group than in the PA group (23.5% vs. 17.4%), although the difference was not statistically significant. Additionally, geographic differences and medical environment of South Korea could also have contributed to the presence of methicillin-resistant strains.
In a recent epidemiology study, the MRSA was found to account for 64% of the nosocomial S. aureus isolates in the Republic of Korea.[18]
We have performed the swab culture procedure in the nasal phase, mainly from the middle turbinate mucosa or septal mucosa. The nasal cavity was prepared with povidone-iodine soaked cottonoids before introducing the endoscope. Regarding the location where the swab culture performed, a previous report has demonstrated that the compositions of bacterial flora in the nasal cavity and sphenoid sinus were different.
[19] Furthermore, another recent study has reported that sinusitis in the sphenoid sinus can be a predisposing factor for postoperative CNS infection.[20] In another report regarding pituitary abscess following transsphenoidal surgery,[21]
retrograde infection from the sphenoid sinus has been suggested to be a vital mechanism. Taken together, these findings suggest a possibility that, as compared to culture results from the nasal cavity, the swab culture results from the sphenoid sinus could more accurately determine the clinical impact on the occurrence of CNS infection.
2. Evaluating the clinical outcome of antibiotic prophylaxis with third-generation cephalosporins including the occurrence of CNS infection
In the present study, postoperative CSF leakage occurred in 3.6% of the patients, while bacterial meningitis developed in 0.9%. These findings are comparable or even better than those reported in a study with antibiotic prophylaxis regimen of third-generation cephalosporins with aminoglycoside.
[10] In a larger-scale study using cefuroxime as an antibiotic prophylaxis, the authors reported 0.8% occurrence of meningitis.[22] However, in the aforementioned study, only culture-positive cases were classified as meningitis. By contrast, in our study, the presented CNS infection cases did not show positive results from the CSF culture, but the CSF findings were consistent with bacterial meningitis (low glucose level and presence of WBC in the CSF). Therefore, the rate of CNS infection could have been underestimated in the study by Jin et al. [22].
In a study on the previous history of surgical procedure, Fig. 6
A B
Pre and postoperative images of central nervous system infection cases. (A) The coronal section of preoperative gadolinium-enhanced T1 image (left panel) shows an 8.4 mm-sized nodular mass located in the suprasellar region. The mass was totally removed in the postoperative gadolinium-enhanced T1 image (right panel), accompanying with postoperative changes. (B) The sagittal section of the patient’s preoperative gadolinium-enhanced T1 image (left panel) reveals a 5.4×4.4 cm-sized cystic and solid mass with thin rim enhancement at the sellar and suprasellar region. The mass was expanding into the third ventricle and displacing the hypothalamus to the superior and posterior direction. The postoperative gadolinium-enhanced T1 image (right panel) shows total removal of the tumor, and the vascularized nasoseptal flap is visible covering the sellar floor. The nasal septum is not visible, since, after the first surgery, the nasoseptal mucosa of the other side was removed due to infection.
major complications following primary transsphenoidal pituitary surgery were reported in 8.39% cases.[23] CSF leakage or bacterial meningitis rate amounted to 3.58%. This rate of complication nearly doubled in revision cases (6.25%
vs. 3.58%); however, the difference was not statistically significant. In the present study, the presence of a previous surgical treatment did not show significant differences among the three groups, and no significant differences were observed in the occurrence of the CNS infection.
We did not routinely perform lumbar drainage in most cases, even in the patients with postoperative CSF leakages,[16]
focusing more on the reconstructive method itself. When postoperative CSF leakage was suspected and appeared to be definitive after several days of close observation, a revision surgery for exploration was preferred over lumbar drainage. Only in 2 cases, lumbar drainage was applied as an adjunctive after sellar floor reconstruction: one being the craniopharyngioma case mentioned above, and the other being a chordoma case. Both patients needed sellar floor reconstruction for Grade 3 intraoperative CSF leakage and a large sized dural defect. One of them eventually developed CNS infection, but the result was insignificant. Although an increased duration of lumbar drainage is known to elevate the CNS infection rate,[24] appropriate use of lumbar drainage has not been reported to increase the rate of CNS infection, and can even lower the incidence of postoperative meningitis.[25]
The mean period of antibiotic treatment was 5.6 days IV, and 13.1 days PO. The period of the IV antibiotic treatment was somewhat shorter in the PI group, but the difference did not reach statistical significance. Upon discharge, the patients received PO antibiotics until the next hospital visiting day, and additional PO antibiotics were prescribed by the rhinology surgeon based on the endoscopic findings of the nasal cavity.
The proportion of the study population that received additional PO antibiotics was 94/222 (42.3%), and the mean duration was 11.9 days (range, 7-30). Most commonly identified reasons for the additional prescription were mucoid/purulent discharge and crust formation in the nasal cavity. On a thorough review of medical reports, no documented side effects were reported
regarding the prolonged use of antibiotics.
3. Limitations and CNS infection case review
The present study has several limitations. First of all, the incidence of CNS infection was too low in our study for further analyses. We calculated the necessary sample size required to demonstrate the relationship between prophylaxis- appropriateness and the occurrence rate of CNS infection using the G*Power V.3.1.7 program (Franz Faul, Christian- Albrechts-Universit t zu Kiel, Kiel, Germany).[26] Given the occurrence rate in the PA and PI groups (0% and 2.9%) and the ratio of their sample sizes (132 cases vs. 34 cases), a total of 788 cases would have been necessary to prove the difference with the Fisher’s exact test. This finding can be used as an important reference for future trials, to which the present study can serve as a pilot study.
Second, although the nasal cavity culture was prospectively designed, a small portion of the treated population was not included due to the omission of the procedure, leaving the possibility of a selection bias. Furthermore, other clinical data were gained retrospectively, which might have compromised the quality of our data.
Third, considering that the surgeries were not performed by a single surgeon, the surgical skills may not have been uniform in all studied cases. However, being a single institution, we share the principles of treatment protocol, including the tumor removal principles, sellar floor reconstruction methods, and management of postoperative CSF leakage patients.
Regarding the clinical factors involved in the CNS infection cases discussed above, some common features should be noted. First, both were craniopharyngioma cases with Grade 3 intraoperative CSF leakage. They also required postoperative steroid replacement, and the nasal cavity culture results eventually revealed the growth of methicillin-resistant strains of Staphylococcus species. Following the CNS infection, a revision surgery for sellar floor reconstruction was necessary for postoperative CSF leakage in both cases. The patients eventually had to be treated with a combination of vancomycin and cefepime for approximately four weeks.
▒ CONCLUSION
The present study is the first report to describe the distribution of the micro-organisms during EETS in the South Korean population. Antibiotic prophylaxis with third- generation cephalosporins yielded appropriate prophylaxis in most (85%) of the patients, yielding comparable clinical outcomes (CNS infection occurrence rate of 0.9%). Although our results did not demonstrate the relationship between prophylaxis-appropriateness and the occurrence of CNS infection, our study is the first attempt to test the aforementioned hypothesis. Therefore, our findings can serve as a pilot study for future larger-scale well-controlled studies.
The common findings in our CNS infection cases may be the key factors that should be properly analyzed among other causative factors involved in CNS infection.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Asemota AO, Ishii M, Brem H, Gallia GL. Comparison of complications, trends, and costs in endoscopic vs microscopic pituitary surgery: Analysis from a US health claims database. Neurosurgery 2017;81:458-72.
2. Hansasuta A, Pokanan S, Punyawai P, Mahattanakul W. Evolution of technique in endoscopic transsphenoidal surgery for pituitary adenoma: A single institution experience from 220 procedures. Cureus 2018;10:e2010.
3. Gao Y, Zhong C, Wang Y, Xu S, Guo Y, Dai C, et al. Endoscopic versus microscopic transsphenoidal pituitary adenoma surgery: a meta-analysis.
World J Surg Oncol 2014;12:94.
4. Halvorsen H, Ramm-Pettersen J, Josefsen R, Rønning P, Reinlie S, Meling T, et al. Surgical complications after transsphenoidal microscopic and endoscopic surgery for pituitary adenoma: a consecutive series of 506 procedures. Acta Neurochir (Wien) 2014;156:441-9.
5. Kassam AB, Prevedello DM, Carrau RL, Snyderman CH, Thomas A, Gardner P, et al. Endoscopic endonasal skull base surgery: analysis of complications in the authors' initial 800 patients. J Neurosurg 2011;114:1544-68.
6. Dusick JR, Esposito F, Kelly DF, Cohan P, DeSalles A, Becker DP, et al. The extended direct endonasal transsphenoidal approach for nonadenomatous suprasellar tumors. J Neurosurg 2005;102:832-41.
7. Saleh AM, Torres KM, Murad MH, Erwin PJ, Driscoll CL. Prophylactic
perioperative antibiotic use in endoscopic sinus surgery: a systematic review and meta-analysis. Otolaryngol Head Neck Surg 2012;146:533-8.
8. Chandra RK, Conley DB, Kern RC. Prophylactic i.v. antibiotics in functional endoscopic sinus surgery: trends and attitudes of the American Rhinologic Society membership. Am J Rhinol Allergy 2009;23:448-50.
9. Zhang Z, Palmer JN, Morales KH, Howland TJ, Doghramji LJ, Adappa ND, et al. Culture-inappropriate antibiotic therapy decreases quality of life improvement after sinus surgery. Int Forum Allergy Rhinol 2014;4:403-10.
10. Orlando R, Cappabianca P, Tosone G, Esposito F, Piazza M, de Divitiis E.
Retrospective analysis of a new antibiotic chemoprophylaxis regimen in 170 patients undergoing endoscopic endonasal transsphenoidal surgery. Surg Neurol 2007;68:145-8.
11. Brown SM, Anand VK, Tabaee A, Schwartz TH. Role of perioperative antibiotics in endoscopic skull base surgery. Laryngoscope 2007;117:1528- 32.
12. Murray PR, Baron EJ, Jorgensen JH, Pfaller MA, Yolken RH. Manual of clinical microbiology. 8th ed. Washington, DC: American Society for Microbiology Press; 2003.
13. Summanen P, Baron EJ, Citron DM, Strong C, Wexler HM, Finegold SM.
Wadsworth anaerobic bacteriology manual. 5th ed. Belmont, CA: Star Publishing Co.; 1993.
14. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. 27th ed. Wayne, PA: Clinical and Laboratory Standards Institute; 2017.
15. Kim BY, Shin JH, Kang SG, Kim SW, Hong YK, Jeun SS, et al. Bilateral modified nasoseptal "rescue" flaps in the endoscopic endonasal transsphenoidal approach. Laryngoscope 2013;123:2605-9.
16. Park JH, Choi JH, Kim YI, Kim SW, Hong YK. Modified graded repair of cerebrospinal fluid leaks in endoscopic endonasal transsphenoidal surgery. J Korean Neurosurg Soc 2015;58:36-42.
17. Esposito F, Dusick JR, Fatemi N, Kelly DF. Graded repair of cranial base defects and cerebrospinal fluid leaks in transsphenoidal surgery.
Neurosurgery 2007;60:295-303.
18. Kim HB, Jang HC, Nam HJ, Lee YS, Kim BS, Park WB, et al. In vitro activities of 28 antimicrobial agents against Staphylococcus aureus isolates from tertiary-care hospitals in Korea: a nationwide survey. Antimicrob Agents Chemother 2004;48:1124-7.
19. Shibao S, Toda M, Tomita T, Ogawa K, Yoshida K. Analysis of the bacterial flora in the nasal cavity and the sphenoid sinus mucosa in patients operated on with an endoscopic endonasal transsphenoidal approach. Neurol Med Chir (Tokyo) 2014;54:1009-13.
20. Kim DH, Hong YK, Jeun SS, Park JS, Kim SW, Cho JH, et al. Is coincidental rhinosinusitis a predisposing factor for postoperative central nervous system infection after endoscopic endonasal transsphenoidal surgery? J Craniofac Surg 2018;29:e319-e22.
21. Wang L, Yao Y, Feng F, Deng K, Lian W, Li G, et al. Pituitary abscess following transsphenoidal surgery: the experience of 12 cases from a single institution. Clin Neurol Neurosurg 2014;124:66-71.
22. Jin Y, Liu X, Gao L, Guo X, Wang Q, Bao X, et al. Risk factors and microbiology of meningitis and/or bacteremia after transsphenoidal surgery for pituitary adenoma. World Neurosurg 2018;110:e851-e63.
23. Krings JG, Kallogjeri D, Wineland A, Nepple KG, Piccirillo JF, Getz AE.
Complications following primary and revision transsphenoidal surgeries for pituitary tumors. Laryngoscope 2015;125:311-7.
24. Ivan ME, Iorgulescu JB, El-Sayed I, McDermott MW, Parsa AT, Pletcher SD, et al. Risk factors for postoperative cerebrospinal fluid leak and meningitis after expanded endoscopic endonasal surgery. J Clin Neurosci 2015;22:48-54.
25. van Aken MO, Feelders RA, de Marie S, van de Berge JH, Dallenga AH, Delwel EJ, et al. Cerebrospinal fluid leakage during transsphenoidal surgery:
postoperative external lumbar drainage reduces the risk for meningitis.
Pituitary 2004;7:89-93.
26. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods 2009;41:1149-60.