274
HIV와 HAART 요법과 관련된 대사합병증: 개요 및 임상증례보고
최은주
1*·Kathleen K. Graham
21조선대학교 약학대학 & 임상약학대학원,2Children's Diagnostic & Treatment Center, FL, USA (2012년 8월 24일 접수·2012년 9월 14일 수정·2012년 9월 17일 승인)
Metabolic Complications Associated with HIV and Highly Active Antiretroviral Therapy : Overview & A Clinical Case Report
Eun Joo Choi
1* and Kathleen K. Graham
21College of Pharmacy & Graduate School of Clinical Pharmacy, Chosun University, Gwangju 501-759, Korea
2Children’s Diagnostic & Treatment Center, Ft. Lauderdale, FL, USA (Received August 24, 2012·Revised September 14, 2012·Accepted September 17, 2012)
현재 HIV(human immunodeficiency virus) 감염에 대하여 보다 많은 효과적인 약물치료법이 가능하다. Highly active antiretroviral therapy (HAART) 로 언급되는 이 치료법은 항 HIV치료제의 다양한 병용법으로 구성된다. 그러나, 최근에 이렇게 치료된 환자들에게 중요한 독성들(toxicities)로서 빈번하게 상당한 지질이상과 혈중당의 항상성 조절장애와 연관 된 몸의 지방 분포 비정상으로서 나타나는, 광범위한 대사성 합병증(metabolic complications)이 출현해왔다. 이러한 합 병증의 관리는 표준적인 치료 중재(interventions)와 연관하여 지질과 당 대사와 관련된 항 HIV치료제의 특성 있는 효 과를 이해하면서, 항 HIV 약물들을 조절하는 것을 포함한다. 본 증례는 항HIV 약물요법과정에서 나타난 상당한 지질 이상, 매우 높은 LDL 수치와 높은 TG수치에 따르는 후속 약물요법을 보여주며, 개별화된 항 HIV 약물요법을 수행 하면서, 대사성 합병증에 관련된 수치의 검사와 주기적인 약물치료과정의 모니터링을 권하여 HIV에 감염된 환자들의 효과적인 치료를 향상시키기 위한 것이다.
□ Key words - HIV, Metabolic complications, dyslipidemia, HAART
INTRODUCTION
Antiretroviral therapy (ART) for the treatments of human immunodeficiency virus (HIV) infection has pro- moted consistently since the appearance of effective combination therapy in 1995.
1-2)The extensive applica- tion of combination ART has led to a remarkable and continuous reduction in the morbidity and mortality in HIV-infected patients and has converted a HIV-infected condition into a chronic state.
3-5)The therapies, known as highly active antiretroviral therapy (HAART), consist of diverse combinations of anti-HIV drugs from differ- ent drug groups.
1-2,4)The worldwide use of HAART has
led to frequent occurrence related to metabolic abnor- malities.
2,6)Metabolic complications such as frequently profound dyslipidemia and glucose homeostasis dysreg- ulation have appeared as significant toxicities in HIV- treated patients.
2)Especially, the long-term implications of altered lipids in HIV-infected persons is still under study, but it is potential that cardiovascular health will be imperiled, with the possibility for increased cardiac mortality.
7-9,12)Dyslipidemia has commomly been related to the use of Protease Inhibitor (PI)-based regimens in HAART, and ritonavir-containing regimens have spe- cially been associated with enhanced incidence of dys- lipidemia.
10-12)Prevention and management of Metabolic complications have issued as major challenges to health- care professionals for the care of HIV-infected per- sons.
13-15)Potential contributing factors are associated with host characteristics, HIV viral parameters and spe- cific effects of anti-HIV drugs on adipose-tissue biology
Correspondence to : Eun Joo Choi
College of Pharmacy & Graduate School of Pharmacy, Chosun University, 309 Pilmundaero, Dong-gu, Gwangju 501-759, Korea
Tel: +82-62-230-6382, Fax: +82-62-222-5414 E-mail: [email protected]
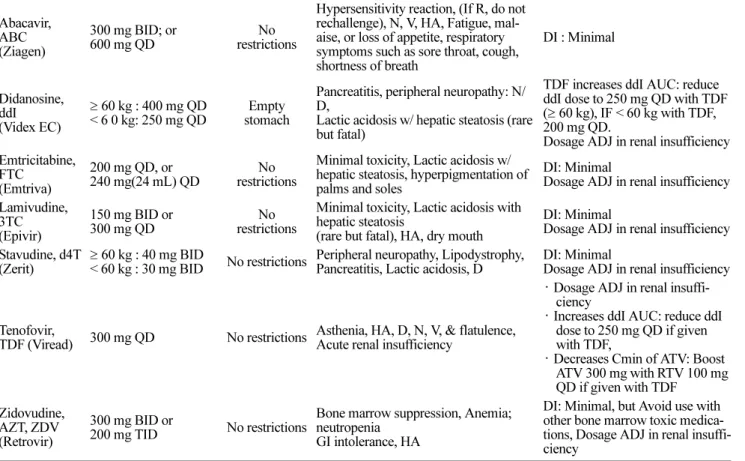
Table 1. ANTIRETROVIRALS (ARVs) Generic Name,
Abbreviation (Trade Name)
Adult Dosing Food Effect Adverse Events NOTE
Nucleoside Reverse Transcriptase Inhibitors (NRTIs): Lactic acidosis/hepatic steatosis; pancreatitis (severe mitochondrial toxicities);
hepatotoxicity, body fat redistribution Abacavir,
ABC (Ziagen)
300 mg BID; or 600 mg QD
No restrictions
Hypersensitivity reaction, (If R, do not rechallenge), N, V, HA, Fatigue, mal- aise, or loss of appetite, respiratory symptoms such as sore throat, cough, shortness of breath
DI : Minimal
Didanosine, ddI
(Videx EC)
≥ 60 kg : 400 mg QD
< 6 0 kg: 250 mg QD
Empty stomach
Pancreatitis, peripheral neuropathy: N/
D,
Lactic acidosis w/ hepatic steatosis (rare but fatal)
TDF increases ddI AUC: reduce ddI dose to 250 mg QD with TDF (≥ 60 kg), IF < 60 kg with TDF, 200 mg QD.
Dosage ADJ in renal insufficiency Emtricitabine,
FTC (Emtriva)
200 mg QD, or 240 mg(24 mL) QD
No restrictions
Minimal toxicity, Lactic acidosis w/
hepatic steatosis, hyperpigmentation of palms and soles
DI: Minimal
Dosage ADJ in renal insufficiency Lamivudine,
3TC (Epivir)
150 mg BID or 300 mg QD
No restrictions
Minimal toxicity, Lactic acidosis with hepatic steatosis
(rare but fatal), HA, dry mouth
DI: Minimal
Dosage ADJ in renal insufficiency Stavudine, d4T
(Zerit) ≥ 60 kg : 40 mg BID
< 60 kg : 30 mg BID No restrictions Peripheral neuropathy, Lipodystrophy, Pancreatitis, Lactic acidosis, D
DI: Minimal
Dosage ADJ in renal insufficiency
Tenofovir,
TDF (Viread) 300 mg QD No restrictions Asthenia, HA, D, N, V, & flatulence, Acute renal insufficiency
· Dosage ADJ in renal insuffi- ciency
· Increases ddI AUC: reduce ddI dose to 250 mg QD if given with TDF,
· Decreases Cmin of ATV: Boost ATV 300 mg with RTV 100 mg QD if given with TDF
Zidovudine, AZT, ZDV (Retrovir)
300 mg BID or
200 mg TID No restrictions
Bone marrow suppression, Anemia;
neutropenia GI intolerance, HA
DI: Minimal, but Avoid use with other bone marrow toxic medica- tions, Dosage ADJ in renal insuffi- ciency
Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs): Rash including Steven’s Johnson Syndrome (SJS)/Toxic epidermal necrosis;
hepatotoxicity Delavirdine, DLV (Rescriptor)
400 mg TID No restrictions R, Increased transaminase levels, HA, Fatigue; N/D
Substrate and Inhibitor of liver enzymes
Efavirenz, EFV (Sustiva)
600 mg QD
Empty stom- ach , at or before bedtime
R, CNS symptioms( dizziness, somno- lence, insomnia, abnormal dreams), Ter- atogenic
Inducer, Inhibitor, and Substrate of liver enzymes
Etravirine, ETV (Intelence)
200 mg BID With food N, R
· ETV is a substrate(3A4, 2C9, 2C19), Inducer (3A4) & Inhibi- tor (2C19) of liver enzymes
· Do not co-administer with TPV/
r, f-APV/r, ATV/r, non-RTV- boosted PIs, and other NNRTIs Nevirapine,
NVP (Viramune)
200 mg QD for 14 days;
then, 200 mg by mouth BID
No restrictions R, Symptomatic hepatitis including fatal hepatic necrosis
Substrate and Inducer of liver enzymes
Fusion Inhibitor Enfuvirtide, T- 20
(Fuzeon)
90 mg(1 mL) SC, BID Not applicable Local Injection site reactions, Increased bacterial pneumonia
DI: Minimal, Storage : Room Temperature, Reconstituted solu- tion should be stored under refrig- eration and used within 24 hrs.
*N/V/D = nausea/vomiting/diarrhea; GI = gastrointestinal; HA = headache; R = rash; QD = once daily; BID = twice daily; TID = three times daily;
ADJ = adjustment; DI = Drug Interactions
- Adapted and summarized from reference 1 and 16.
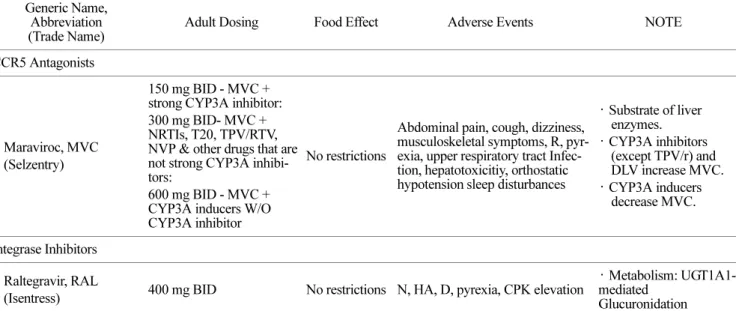
Table 1. ANTIRETROVIRALS (ARVs) (continued) Generic Name,
Abbreviation (Trade Name)
Adult Dosing Food Effect Adverse Events NOTE
CCR5 Antagonists
Maraviroc, MVC (Selzentry)
150 mg BID - MVC + strong CYP3A inhibitor:
300 mg BID- MVC + NRTIs, T20, TPV/RTV, NVP & other drugs that are not strong CYP3A inhibi- tors:
600 mg BID - MVC + CYP3A inducers W/O CYP3A inhibitor
No restrictions
Abdominal pain, cough, dizziness, musculoskeletal symptoms, R, pyr- exia, upper respiratory tract Infec- tion, hepatotoxicitiy, orthostatic hypotension sleep disturbances
· Substrate of liver enzymes.
· CYP3A inhibitors (except TPV/r) and DLV increase MVC.
· CYP3A inducers decrease MVC.
Integrase Inhibitors Raltegravir, RAL
(Isentress) 400 mg BID No restrictions N, HA, D, pyrexia, CPK elevation · Metabolism: UGT1A1- mediated
Glucuronidation Protease Inhibitors(PIs): Metabolic abnormalities including dyslipidemia, hyperglycemia, insulin resistance, and lipodystrophy (Ataza- navir is less likely to cause dyslipidemia) Osteonecrosis and hepatotoxicity, increased the risk of bleeding in hemophiliacs, or significant interactions with other drugs.
Atazanavir, ATV (Reyataz)
400 mg QD
* If taken w/ EFV or TDF:
300 mg QD + RTV 100 mg QD
With food Avoid taking
with antacids.,
Hyperbilirubinemia, Prolonged PR interval, hyperglycimia, Nephroli- thiasis
Substrate and Inhibitor of liver enzymes.
Boost with RTV when given with TDF.
Dosage adjustment in hepatic insufficiency recommanded Darunavir, DRV
(Prezista)
(DRV 600 mg + RTV
100 mg) BID With food R, D, N, HA, Hyperlipidemia,Tran- saminase elevation
Substrate and Inhibitor of liver enzymes (CYP450 3A4)
Fosamprenavir, FPV
(Lexiva)
ARV naïve pt:
-FPV 1400 mg BID or -(FPV1400 mg QD + RTV 200 mg) QD or
- (FPV 700 mg + RTV 100 mg) BID
-(FPV 1400 mg + RTV 100 mg) QD
PI-experienced pts (QD not recommended):
(FPV 700 mg + RTV 100 mg) BID
Coadministration w/ EFV (FPV boosted only):
(FPV 700 mg + RTV 100 mg) BID or (FPV 1,400 mg + RTV 300 mg) QD
No restrictions
R, D, N, V, HA, Hyperglycemia, Hyperlipidemia
Transaminase elevation, oral paresthesias
Substrate and inhibitor of liver enzymes;
Consider DI
Dosage adjustment in hepatic insufficiency recommanded
N/V/D = nausea/vomiting/diarrhea; GI = gastrointestinal; HA = headache; R = rash; QD = once daily; BID = twice daily; TID = three times daily;
ADJ = adjustment; DI = Drug Interaction ***COMBINATION DRUGs: 1. Zidovudine / Lamivudine, AZT + 3TC (Combivir)-One BID 2.
Lamivudine / Abacavir, 3TC + ABC (Epzicom)-One QD 3. Zidovudine, Lamivudine, Abacavir, AZT + 3TC + ABC (Trizivir)-One BID 4.
Tenofovir, Emtricitabine, TDF + FTC (Truvada)-One QD 5. Efavirenz / emtricitabine / tenofovir, EFV + FTC + TDF (Atripla)-One QD - Adapted and summarized from reference 1 and 16.
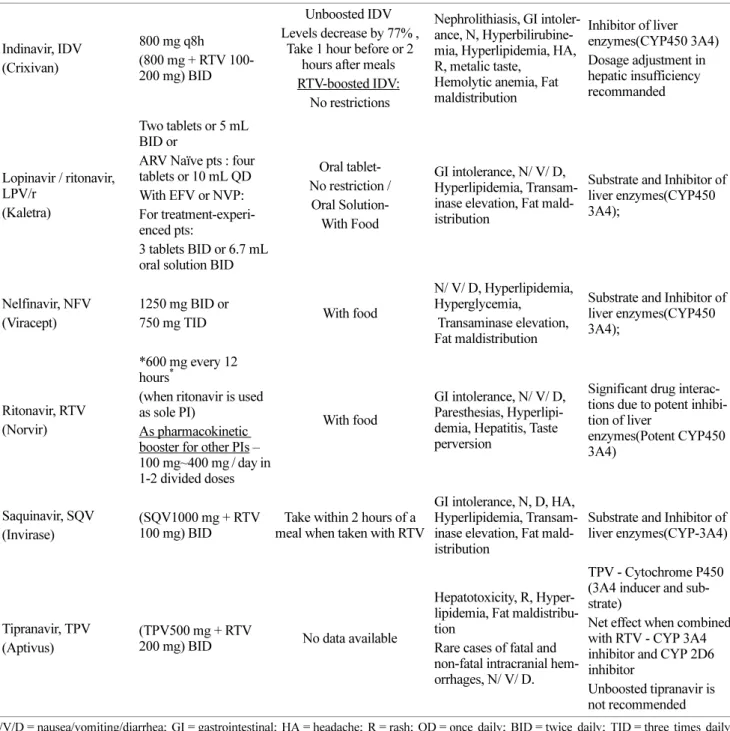
Table 1. ANTIRETROVIRALS (ARVs) (continued) Generic Name,
Abbreviation (Trade Name)
Adult Dosing Food Effect Adverse Events NOTE
(continued) Protease Inhibitors(PIs): Metabolic abnormalities including dyslipidemia, hyperglycemia, insulin resistance, and lipodystro- phy (Atazanavir is less likely to cause dyslipidemia) Osteonecrosis and hepatotoxicity, increased the risk of bleeding in hemophiliacs, or significant interactions with other drugs.
Indinavir, IDV (Crixivan)
800 mg q8h (800 mg + RTV 100- 200 mg) BID
Unboosted IDV Levels decrease by 77% ,
Take 1 hour before or 2 hours after meals RTV-boosted IDV:
No restrictions
Nephrolithiasis, GI intoler- ance, N, Hyperbilirubine- mia, Hyperlipidemia, HA, R, metalic taste,
Hemolytic anemia, Fat maldistribution
Inhibitor of liver enzymes(CYP450 3A4) Dosage adjustment in hepatic insufficiency recommanded
Lopinavir / ritonavir, LPV/r
(Kaletra)
Two tablets or 5 mL BID or
ARV Naïve pts : four tablets or 10 mL QD With EFV or NVP:
For treatment-experi- enced pts:
3 tablets BID or 6.7 mL oral solution BID
Oral tablet- No restriction /
Oral Solution- With Food
GI intolerance, N/ V/ D, Hyperlipidemia, Transam- inase elevation, Fat mald- istribution
Substrate and Inhibitor of liver enzymes(CYP450 3A4);
Nelfinavir, NFV (Viracept)
1250 mg BID or
750 mg TID With food
N/ V/ D, Hyperlipidemia, Hyperglycemia,
Transaminase elevation, Fat maldistribution
Substrate and Inhibitor of liver enzymes(CYP450 3A4);
Ritonavir, RTV (Norvir)
*600 mg every 12 hours
*(when ritonavir is used as sole PI)
As pharmacokinetic booster for other PIs – 100 mg~400 mg / day in 1-2 divided doses
With food
GI intolerance, N/ V/ D, Paresthesias, Hyperlipi- demia, Hepatitis, Taste perversion
Significant drug interac- tions due to potent inhibi- tion of liver
enzymes(Potent CYP450 3A4)
Saquinavir, SQV (Invirase)
(SQV1000 mg + RTV 100 mg) BID
Take within 2 hours of a meal when taken with RTV
GI intolerance, N, D, HA, Hyperlipidemia, Transam- inase elevation, Fat mald- istribution
Substrate and Inhibitor of liver enzymes(CYP-3A4)
Tipranavir, TPV (Aptivus)
(TPV500 mg + RTV
200 mg) BID No data available
Hepatotoxicity, R, Hyper- lipidemia, Fat maldistribu- tion
Rare cases of fatal and non-fatal intracranial hem- orrhages, N/ V/ D.
TPV - Cytochrome P450 (3A4 inducer and sub- strate)
Net effect when combined with RTV - CYP 3A4 inhibitor and CYP 2D6 inhibitor
Unboosted tipranavir is not recommended
N/V/D = nausea/vomiting/diarrhea; GI = gastrointestinal; HA = headache; R = rash; QD = once daily; BID = twice daily; TID = three times daily;ADJ = adjustment; DI = Drug Interaction ***COMBINATION DRUGs: 1. Zidovudine / Lamivudine, AZT + 3TC (Combivir)-One BID 2.
Lamivudine / Abacavir, 3TC + ABC (Epzicom)-One QD 3. Zidovudine, Lamivudine, Abacavir, AZT + 3TC + ABC (Trizivir)-One BID 4.
Tenofovir, Emtricitabine, TDF + FTC (Truvada)-One QD 5. Efavirenz / emtricitabine / tenofovir, EFV + FTC + TDF (Atripla)-One QD - Adapted and summarized from reference 1 and 16.
and metabolism.
1-4)Management of the metabolic compli- cations include manipulation of the anti-HIV drugs with a knowledge of their specific effects on lipid and glucose metabolism, related to established therapeutic interven- tions (Table 1).
1-2,15-16)Additionally, lifestyle interventions as smoking cessation, a healthy diet and excercise play a pivotal role in reducing dyslipidemia in HIV-infected persons.
15)This article is to report an unusual case that very high level of low-density lipoprotein (LDL) and high level of triglyceride (TG) were measured in the process of anti-HIV pharmacotherapy, suggesting regu- lar monitoring of labs for the optimal individualized treatment in HIV-infected persons to prevent and man- age metabolic complications.
CASE REPORT
The patient, ES was a 35-year-old Caucasian female (Height: 5’8”(172.7 cm), Weight: 200 lbs(91 kg)) who pre- sented to HIV Clinic. She reported that she didn’t want to take her HIV medications due to severe nausea &
vomiting and also stopped these meds 3 days ago. In addition, she reported that she thought her HIV meds made her sick. She mentioned that she took her HIV medications(meds) on empty stomach and with no breakfast every morning until 3 days ago. Her current
antiretrovirals (ARVs) were needed to change because of her severe nausea & vomiting. The patient had been HIV positive since 1999. She was on ARVs. She visited the HIV meds on Mar.4, 2008 due to diarrhea for a cou- ple of days. She took Immodium, and continued with her current meds. Her lab was ordered. Her return to clinic was scheduled to Mar 21, 2008. Previously, she had severe diarrhea on viracept and rash on viramune on 2000.
17-18)Her recent antiretroviral therapy (ART) which was PI-based is truvada 1 tablet once daily, kaletra 2 tab- lets twice a day.
19-20)Her previous and current medica- tion lists shows Table 2.
Table 2. Patient's Medication List
Previous Meds :
03/04/08 Immodium 2 mg, 1 capsule BID PRN for diarrhea
02/04/08 Flagyl 500 mg 1 tab po twice daily for seven days.
01/04/08 FeSO
41 tab po 3 times a day Truvada 1 tab po daily
Kaletra 400/100 mg 2 tab po daily (D/C Viracept due to diarrhea) Procrit 40,000 units/ml Inject 1 ml (one ml)
-Once weekly dispense,1 month supply(*4)
10/10/07 Truvada 1 tab once daily Viracept 625 mg, 2 tabs twice daily
Previous ARVs :
Emtricitabine(FTC), Tenofovir(TDF), Nelfi- navir(NFV)
Current Meds: Truvada 1 daily, Kaletra 2 tablets twice a day Vit B12, Iron pill
Meds: medications, BID: two times a day, PRN: as needed, PO: per oral
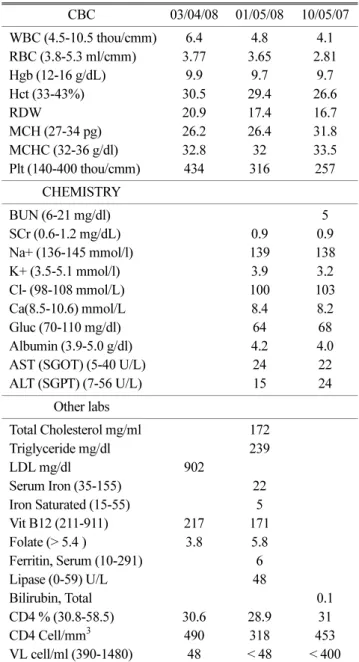
Table 3. The patient's lab data after HIV clinic visit
CBC 03/04/08 01/05/08 10/05/07
WBC (4.5-10.5 thou/cmm) 6.4 4.8 4.1
RBC (3.8-5.3 ml/cmm) 3.77 3.65 2.81
Hgb (12-16 g/dL) 9.9 9.7 9.7
Hct (33-43%) 30.5 29.4 26.6
RDW 20.9 17.4 16.7
MCH (27-34 pg) 26.2 26.4 31.8
MCHC (32-36 g/dl) 32.8 32 33.5
Plt (140-400 thou/cmm) 434 316 257
CHEMISTRY
BUN (6-21 mg/dl) 5
SCr (0.6-1.2 mg/dL) 0.9 0.9
Na+ (136-145 mmol/l) 139 138
K+ (3.5-5.1 mmol/l) 3.9 3.2
Cl- (98-108 mmol/L) 100 103
Ca(8.5-10.6) mmol/L 8.4 8.2
Gluc (70-110 mg/dl) 64 68
Albumin (3.9-5.0 g/dl) 4.2 4.0
AST (SGOT) (5-40 U/L) 24 22
ALT (SGPT) (7-56 U/L) 15 24
Other labs
Total Cholesterol mg/ml 172
Triglyceride mg/dl 239
LDL mg/dl 902
Serum Iron (35-155) 22
Iron Saturated (15-55) 5
Vit B12 (211-911) 217 171
Folate (> 5.4 ) 3.8 5.8
Ferritin, Serum (10-291) 6
Lipase (0-59) U/L 48
Bilirubin, Total 0.1
CD4 % (30.8-58.5) 30.6 28.9 31
CD4 Cell/mm
3490 318 453
VL cell/ml (390-1480) 48 < 48 < 400
Her family history was hypertension, diabetes, myo- cardiac infarction (MI) and cancer. She has no known drug allergy. Her husband died of acquired immune defi- ciency syndrome (AIDS) prior to transmitting it to her.
She lived in an assisted living facility. She is not drug abuser. She smokes tobacco one pack per day. On March 13, 2008, her pulse was 106, respiratory rate was 20, body temperature was 98.9 F (37.2
oC) and blood pressure (BP) was 105/75 mmHg. On Jan 5, 2008, her lab data were red blood count (RBC) 3.65, hemoglobin (Hgb) 9.7, hematocrit (Hct) 29.4, triglyceride (TG) 239, serum iron 22, iron saturated 5, CD4% 30.6, CD4 cell/mm
3490, viral load (VL) 48. She had no hepatitis B and C. On Mar 5, 2008, her lab data were red blood count (RBC) 3.77, hemoglobin (Hgb) 9.9, hematocrit (Hct) 30.5, low-density lipoprotein (LDL) 902, folate 3.8 and serum HCG < 2. Her stool culture was negative (Table 3). She was not really symptomatic with her anemia unlike her lab data, specifi- cally no fatigue, lethargy or problem of natures. She is HIV positive. Her CD4 count (cell/mm
3) increased from
318 to 490, her viral load is still undetectable (< 50) based on her lab data. Her lab data shows Table 3. She is sched- uled to return to clinic (RTC) in 10 days for follow-up with HLAB*5701 test result and starting her new regimen including abacarvir and atazanavir based on guideline (preferred option).
1)DISCUSSION
This is the rare, unusual case of very highly elevated low-density lipoprotein (LDL) and elevated triglyceride (TG) level in the process of HIV pharmacotherapy. This case suggests that healthcare professionals need to moni- tor regularly patients’ labs in the middle of HIV-infected persons’ pharmacotherapy with ARVs for the optimal individualized treatment as well as prevention and man- agement of metabolic complications, while considering adverse reaction profile of each ARV. Higher LDL levels increase the risk of cardiovascular disease, and reduc- tion thereof reduces this risk.
15,21)Table 4. Therapeutic & Toxic effects with monitoring parameters for each drug lists
Drug's Name Therapeutic(+) Toxic (-)
EPZICOM (Abacarvir + lamivudine)
(+) No food restrictions QD dosing available, Preferred option by guidelines
(-) Hypersensitivity reaction and Dosage adjustment in patients(pts) with renal insufficiency
* Monitor BUN, Scr
* Not for patients with CrCl < 50 mL/min Abacarvir (+) No need for dosage adjustment in
patient with renal or hepatic Insufficiency, No food restriction
* Abacarvir for patients(pts) who test negative for
HLAB*5701 (inform pts of hypersensitivity reaction such as Fever, Rash, Malaise and Nausea which usually appear within the first 6 weeks of treatement, IF pts get the symptom, Just Discontinue and let Doctor know.
Test & Monitor HLAB*5701
* Do not rechallence.
Lamivudine (+) minimal drug interaction No food restriction
(-) lactic acidosis with hepatic steatosis, dry mouth, Headache Monitor BUN, Scr
* Dosage adjustment in renal Insufficiency
* Never can be used as monotherapy because resistance devel- ops rapidly
REYATAZE (Atazanavir)
(+) Less cause dyslipidemia Take with food
(-) Indirect hyperbilirubinemia, Prolonged PR interval, Neph- rolithiasis
*Avoid taking with antacids. *Should not be taken with PPIs / Should be dose adjustment needed if taken with H2 blockers.
No dosage adjustment for patients with renal dysfunction not requiring hemodialysis
* Monitor : LFTs * Dosage adjustment for patients with hepatic impairment (Child-Pugh Score (7-9) 300 mg QD, (> 9) Not recommended )
Adapted and summarized from reference 1,16, 23-25