Korean Clinical Imaging Guidelines for Diagnosis of Headache Based
on the 2017 Evidence-Based Clinical Imaging Guidelines
2017년 근거기반 임상영상 가이드라인에서 연구된 두통 환자 진단을 위한 한국형 영상 검사 권고안
Jo Sung Jung, MD1 , Se Won Oh, MD1* , Jinhee Jang, MD2, Chi-Hoon Choi, MD3, Soo Chin Kim, MD4, Won-Jin Moon, MD5, Miyoung Choi, RN6, Seung Eun Jung, MD2
1Department of Radiology, Soonchunhyang University Cheonan Hospital, Cheonan, Korea
2Department of Radiology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Department of Radiology, Chungbuk National University Hospital, Cheongju, Korea
4Department of Radiology, GangnamCenter, Seoul National University Hospital Healthcare System, Seoul, Korea
5Department of Radiology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
6Division for Healthcare Technology Assessment Research, National Evidence-Based Healthcare Collaborating Agency, Seoul, Korea
Headache is the most common cause of neurological disorders. The usefulness of imaging tests may vary depending on the patient's clinical situation. The Korean Society of Radiology and National Evidence-Based Healthcare Collaborating Agency have decided to develop evi- dence-based guidelines for the imaging tests necessary for diagnosing patients with selected, frequently encountered types of headache. Development, working, and advisory committees were formed. Recommendation statements were derived from the adaptive development methods provided by the existing guidelines. Non-contrast head CT is recommended in pa- tients with acute thunderclap headache due to possible subarachnoid hemorrhage (SAH), and CT angiography is recommended to confirm aneurysmal SAH. In patients with non-acute head- ache and normal neurological findings, radiological examination is not recommended, but head MRI is recommended to investigate the cause of secondary headache. Non-contrast head MRI is recommended for new-onset headache with neurologic abnormalities in pregnant women.
Index terms Headache; Subarachnoid Hemorrhage, Magnetic Resonance Imaging
Received November 13, 2018 Revised March 15, 2019 Accepted April 5, 2019
*Corresponding author Se Won Oh, MD Department of Radiology, Soonchunhyang University Cheonan Hospital, 30 Suncheonhyang 6-gil, Dongnam-gu, Cheonan 31151, Korea.
Tel 82-41-570-3513 Fax 82-41-589-6731 E-mail [email protected] This is an Open Access article distributed under the terms of the Creative Commons Attribu- tion Non-Commercial License (https://creativecommons.org/
licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduc- tion in any medium, provided the original work is properly cited.
ORCID iDs Se Won Oh https://
orcid.org/0000-0003-1336-4498 Jo Sung Jung
https://
orcid.org/0000-0002-3331-3199
가이드라인 개발 배경
두통은 신경학적 문제를 일으키는 가장 흔한 질환으로 환자의 임상적 증상에 따라 1차성과 2차 성 두통으로 나뉜다(1). 1차성 두통은 긴장성 두통, 편두통 그리고 군집성 두통으로 분류할 수 있 는데 한국 성인을 대상으로 한 연구에서 두통의 1년 유병률은 61.4%였고 이 중 긴장성 두통은 30.8%, 편두통은 6.1%로 보고되었다(2). 2차성 두통은 출혈, 종양, 감염 등 다양한 기저 질환에 기 인하여 발생하는 두통을 말하는데(3), 급성벼락두통을 호소하는 환자의 많은 수에서 지주막 출혈 이 확인된다. 지주막 출혈은 10만 명당 9~23명의 발생률을 보이는 드문 질환이지만(4) 높은 사망 률을 보이는 질환이기 때문에 급성벼락두통을 보인 환자들에게는 빠르고 정확한 진단이 요구된 다. 또한 두통은 임산부에서도 매우 흔하게 관찰되며 다양한 기질적 원인의 동반이 확인되고 있다 (5, 6). 따라서 두통이 있는 임산부는 정확한 진단을 위해 영상 검사가 필요할 수 있으나 영상 검사 과정에서 방사선 피폭이나 조영제가 임산부나 태아에게 영향을 줄 수 있어 신중히 고려되어야 한 다(7-9). 이처럼 두통은 다양한 상황에서 다양한 원인에 의해 발생할 수 있는데 진단과정에서 환자 의 임상양상과 상황, 영상 검사의 종류에 따라 유용성이 다를 수 있다. 본 연구의 목적은 두통 환자 를 진단하는 데 있어 의사의 임상적 결정에 도움을 주고, 불필요한 방사선 노출을 피하고 한정된 의료자원을 효율적으로 사용하기 위한 통일된 근거기반 가이드라인 개발에 있다. 본 가이드라인 의 대상 집단은 지주막하 출혈이 의심되는 급성벼락두통 환자, 신경학적 진찰이 정상인 비급성두 통 환자, 새로 생긴 두통이 있는 임산부이며, 대상 독자층은 두통 환자의 진단과 치료를 담당하는 다양한 과의 임상의사 및 영상의학과의사이다. 이를 위해 개발위원회, 실무위원회 그리고 자문위 원회를 구성하여 국외에 이미 개발된 임상영상 가이드라인을 국내 의료상황에 맞도록 수용개작 (adaptation) 하는 방법으로 가이드라인을 개발하였다.
가이드라인 개발을 위한 위원회 구성
가이드라인 개발을 위하여 개발위원회와 실무위원회 그리고 외부협력을 위한 자문위원회를 구 성하였다. 개발위원회는 영상의학 전문의, 연구방법론 전문가, 진료지침 관련 전문가 등으로 구성 하였다. 개발위원회는 가이드라인 개발을 위한 프로토콜을 제안하고, 가이드라인 개발에 필요한 국내외 문헌 수집 정리, 개발 기술 지원 및 프로토콜 교육을 담당하였다. 실무위원회는 대한신경 두경부영상의학회에서 추천한 영상의학 전문의 5명으로 구성하였다. 실무위원회는 연구를 총괄 하며 가이드라인 개발 실무를 담당하였다. 자문위원회는 개발된 진료지침의 최종 사용자로 예상 되는 유관학회(대한신경과학회, 대한신경외과학회, 대한산부인과학회)에서 추천하고 승인한 임 상전문가들로 구성하였으며, 실제 진료지침 개발에는 참여하지 않았지만 진료지침의 핵심질문 선 정과 도출된 권고문에 대한 합의가 이루어지는 단계에서 참여하였다.
가이드라인 개발 과정
가이드라인의 개발은 수용개작 개발방법을 선택하였다. 수용개작 개발방법은 기존 진료지침을 가장 중요한 근거원으로 하여 개발하는 방법으로, 개발위원회에서 개발한 “근거기반 임상영상 가 이드라인 개발 방법론, version 2”에 근거하여 수행되었다(10).
핵심질문 선정
실무위원회와 개발위원회의 논의를 통하여 문장형 핵심질문을 선정하였다. 이후 개발위원회에 서 권고 개발 가능성을 검토하였고 유관 전문학회에 자문을 실시하여 의견을 개발과정에서 반영 하였다. 최종적으로 확정된 핵심질문은 다음과 같다.
1) Subarachnoid hemorrhage (이하 SAH)가 의심되는 급성벼락두통(thunderclap head- ache) 환자에서 어떤 영상 검사를 권장하는가?
2) 신경학적 진찰이 정상인 비급성두통의 경우 어떤 검사를 권장하는가?
3) 임산부에게 새로 생긴 두통의 경우 어떤 검사를 권장하는가?
진료지침 검색
진료지침 검색은 검색의 민감도를 높이는 전략으로 수행하였다. 진료지침 검색은 국내외 데이 터베이스를 활용하여 수행되었는데, 국외 데이터베이스(Ovid-Medline, Ovid-Embase, National Guideline Clearinghouse, Guideline International Network)와 국내 데이터베이스(Kore- aMed, KMbase, KoMGI, KGC)를 모두 검색하였다(Supplementary Tables 1~6 in the online- only Data Supplement). 이후 실무위원회에서 검색 전략 및 결과를 검토하였고 수기 검색을 통 해 누락된 주요 가이드라인을 보완하였다.
검색 진료지침 선별
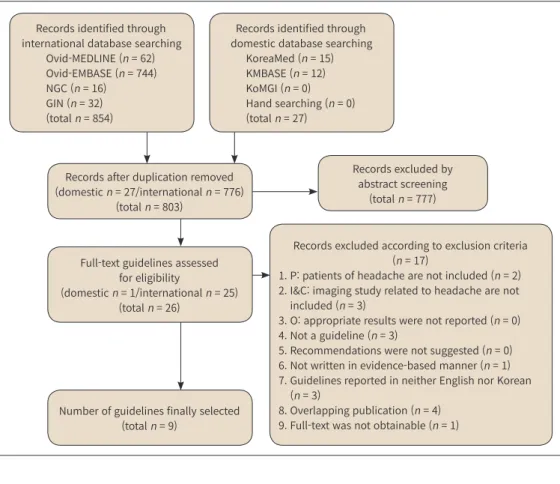
검색된 진료지침의 선별과정은 실무위원회가 수행하였다. 검색된 지침 수는 중복제거 후 803건 (국내 27, 국외 776)이었고, 문헌의 제목 및 초록을 검토하여 1차로 26건이 선별되었다. 2차 선별은 1차로 선택된 문헌의 원문을 검토한 후 이루어졌고 총 9건이 최종 선택되었다. 선별과정은 2인 이 수행하였고 검토자 간 이견이 있을 경우 합의 과정을 거쳤다(Fig. 1).
진료지침 평가
2차 선별과정을 통해 선택된 문헌 중 진료지침 형태만을 대상으로 질평가를 수행하였다. 개발 위원회와 실무위원회가 평가를 담당하였고 Korean Appraisal of Guideline for Research &
Evaluation II를 이용하였다(11). 평가결과 영역별 점수 중 ‘개발의 엄격성’이 50점 이상인 진료지 침을 권고 및 근거정리 대상 진료지침으로 정하였다.
권고 및 근거정리, 권고문 초안 작성
실무위원회에서 평가가 완료된 진료지침의 권고 및 근거를 정리하고(Tables 1-3), 권고문 초안 을 작성하였다. 권고정리 시 핵심질문별 권고의 내용과 Korean Clinical Imaging Guideline (이 하 KCIG)에 따른 등급을(Supplementary Table 7 in the online-only Data Supplement) 정리하 였고 국내 상황에서 실제 적용할 수 있는가를 검토하기 위해 진료지침의 최신성, 수용성, 적용성 을 평가하였다. 근거정리는 핵심질문별로 권고와 관련된 개별 문헌을 검토하여 KCIG에 따른 근거 수준을(Supplementary Table 8 in the online-only Data Supplement) 부여하였다. 핵심질문에 대한 권고문 초안은 권고문, 근거 요약, 권고 고려사항, 참고문헌으로 구성하였다.
권고문 합의 및 권고등급 결정
실무위원회가 작성한 권고문 초안에 대해 개발위원회와의 논의를 거쳐 각 권고문에 대한 권고 등급과 근거수준을 결정하였다.
권고문 최종안 도출
영상의학 분야 전문가(3명), 유관학회(대한신경과학회 1명, 대한신경외과학회 1명, 대한산부인 과학회 1명), 연구방법론 전문가(2명)로 컨센서스 그룹을 구성하여 권고문에 대한 동의 정도를 조
Records identified through international database searching
Ovid-MEDLINE (n = 62) Ovid-EMBASE (n = 744) NGC (n = 16) GIN (n = 32) (total n = 854)
Records identified through domestic database searching
KoreaMed (n = 15) KMBASE (n = 12) KoMGI (n = 0) Hand searching (n = 0) (total n = 27)
Records excluded by abstract screening
(total n = 777)
Records excluded according to exclusion criteria (n = 17)
1. P: patients of headache are not included (n = 2) 2. I&C: imaging study related to headache are not
included (n = 3)
3. O: appropriate results were not reported (n = 0) 4. Not a guideline (n = 3)
5. Recommendations were not suggested (n = 0) 6. Not written in evidence-based manner (n = 1) 7. Guidelines reported in neither English nor Korean
(n = 3)
8. Overlapping publication (n = 4) 9. Full-text was not obtainable (n = 1) Records after duplication removed
(domestic n = 27/international n = 776) (total n = 803)
Full-text guidelines assessed for eligibility
(domestic n = 1/international n = 25) (total n = 26)
Number of guidelines finally selected (total n = 9)
Fig. 1. Flow diagram of guideline selection (Key Questions 1, 2, and 3).
C = comparator, GIN = Guideline International Network, I = intervention, KoMGI = Korean Medical Guideline Information Center, NGC = National Guideline Clearinghouse, O = outcome, P = population
Table 1. Recommendation Matrices of the Existing Guidelines (Key Question 1) Guidelines (Publication Year)Clinical Practice Guideline for the Management of Intracranial Aneurysms (2014) (23)
Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Eepartment with Acute Headache. American College of Emergency Physicians (2008) (42) Guideline for Primary Care Management of Headache in Adults. Institute of Health Economics (2012) (24)
ACR Appropriateness Criteria: Headache (2013) (21) Diagnosis and Management of Headache in Adults (2008) (3)
Clinical Guidelines for the Emergency Eepartment Evaluation of Subarachnoid Hemorrhage (2016) (43) AGREE II227869698539 Recommendation1) Acute diagnostic workup should include noncontrast head CT, which, if nondiagnostic, should be followed by lumbar puncture 2) MRI (FLAIR, proton density, DWI, and gradient echo sequences) may be reasonable for the diagnosis of SAH in patients with a nondiagnostic CT scan, although a negative result does not obviate the need for CSF analysis 3) CTA may be considered in the workup of SAH. If an aneurysm is detected by CTA, this study may help guide the decision for the type of aneurysm repair, but if CTA is inconclusive, DSA is still recommended (except possibly in the instance of classic perimesencephalic SAH) 4) DSA with 3D rotational angiography is indicated for detection of an aneurysm in patients with SAH (except when the aneurysm was previously diagnosed by a noninvasive angiogram) and for planning treatment
Patients presenting with new sudden-onset severe headache should undergo an emergent head CT
Patients presenting with severe headache of sudden onset (thunderclap headache) should be sent to an emergency department with urgent CT capability for immediate investigation to exclude SAH. If SAH is not present on head CT scanning, other investigations (e.g., lumbar puncture) may be necessary 1) CT head without IV contrast 2) CTA head with IV contrast 3) MRA head without and with IV contrast 4) MRA head without IV contrast 5) Arteriography cervicocerebral 6) MRI head without IV contrast In patients with thunderclap headache, unenhanced CT of the brain should be performed as soon as possible and preferably within 12 hours of onset
1) Patients presenting with headache symptoms concerning for SAH can be evaluated safely with NCCT, followed by LP (if CT is negative) 2) CTA is a reasonable strategy to consider for excluding aneurysmal SAH in select patients (in hospitals where CTA is available). It may be an appropriate alternative in those patients at higher risk for SAH after a negative NCCT and in those situations where a diagnostic LP is either refused by the patient or the results of the LP are equivocal 3) There is insufficient evidence at this time to support the use of NCCT alone in the evaluation of SAH, even if the NCCT is performed within the first 6 hours
Table 1. Recommendation Matrices of the Existing Guidelines (Key Question 1) (Continued) Guidelines (Publication Year)Clinical Practice Guideline for the Management of Intracranial Aneurysms (2014) (23)
Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Eepartment with Acute Headache. American College of Emergency Physi- cians (2008) (42) Guideline for Primary Care Management of Headache in Adults. Institute of Health Economics (2012) (24)
ACR Appropriateness Criteria: Headache (2013) (21) Diagnosis and Management of Headache in Adults (2008) (3)
Clinical Guidelines for the Emergency Eepartment Evaluation of Subarachnoid Hemorrhage (2016) (43) (to determine whether an aneurysm is amenable to coiling or to expedite microsurgery) 5) DSA of all cerebral arteries should be performed, if a bleeding source was not found on CTA and the patient has a typical basal SAH pattern on CT 6) If no aneurysm was found, CTA or DSA should be repeated as described below: SAH without aneurysm Grading of recommendationNot availablelevel B [Recommendations for patient management that may identify a particular strategy or range of management strategies that reflect moderate clinical certainty (ie, based on strength of evidence Class II studies that directly address the issue, decision analysis that directly addresses the issue, or strong consensus of strength of evidence Class III studies)]
Do (The GDG accepted the original recommendation, which provided a prescriptive direction to perform the action or used the term “effective” to describe it. The GDG supplemented a recommendation or created a new one, based on their collective professional opinion, and/or systematic reviews which supported the action) 1) 9 2) 8 3–6) 7 (7, 8 ,9: usually appropriate )
Evidence level 3 or 4; or extrapolated evidence from studies rated as 2+
1–2) B 3D = 3-dimensional, ACR = American College of Radiology, AGREE = Appraisal of Guidelines for Research & Evaluation, CSF = cerebrospinal fluid, CTA = CT angiography, DSA = digital subtraction angiography, DWI = diffusion-weighted imaging, FLAIR = fluid-attenuated inversion recovery, IV = intravenous, LP = lumbar puncture, MRA = magnetic resonance angiograph, NCCT = non-contrast CT, SAH = subarachnoid hemorrhage
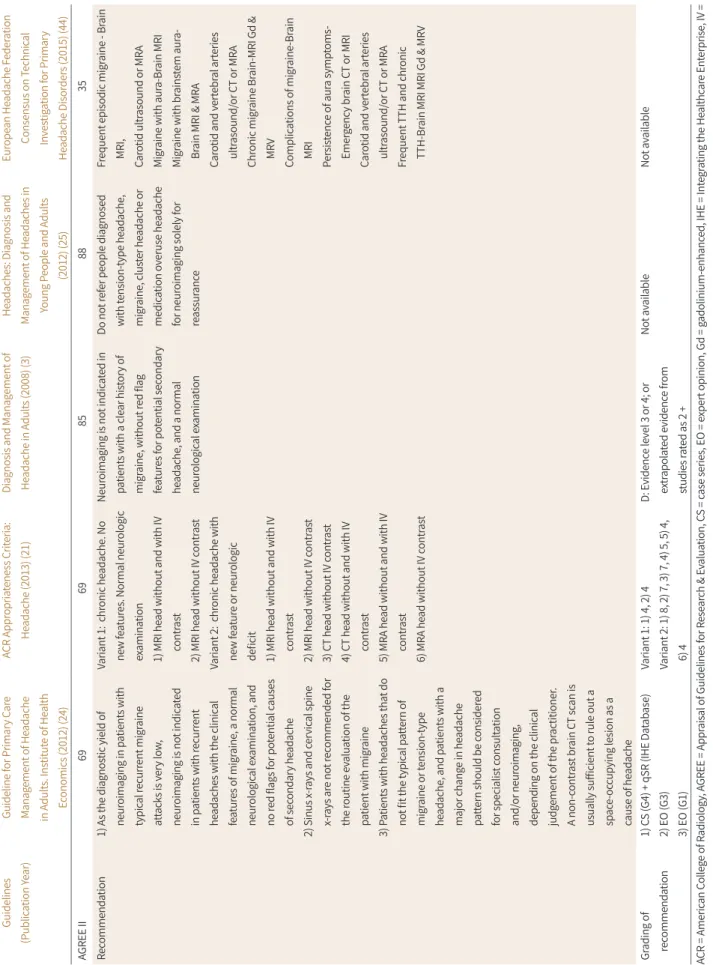
Table 2. Recommendation Matrices of the Existing Guidelines (Key Question 2) Guidelines (Publication Year)Guideline for Primary Care Management of Headache in Adults. Institute of Health Economics (2012) (24) ACR Appropriateness Criteria: Headache (2013) (21)Diagnosis and Management of Headache in Adults (2008) (3)Headaches: Diagnosis and Management of Headaches in Young People and Adults (2012) (25)
European Headache Federation Consensus on Technical Investigation for Primary Headache Disorders (2015) (44) AGREE II6969858835 Recommendation1) As the diagnostic yield of neuroimaging in patients with typical recurrent migraine attacks is very low, neuroimaging is not indicated in patients with recurrent headaches with the clinical features of migraine, a normal neurological examination, and no red flags for potential causes of secondary headache 2) Sinus x-rays and cervical spine x-rays are not recommended for the routine evaluation of the patient with migraine 3) Patients with headaches that do not fit the typical pattern of migraine or tension-type headache, and patients with a major change in headache pattern should be considered for specialist consultation and/or neuroimaging, depending on the clinical judgement of the practitioner. A non-contrast brain CT scan is usually sufficient to rule out a space-occupying lesion as a cause of headache
Variant 1: chronic headache. No new features. Normal neurologic examination 1) MRI head without and with IV contrast 2) MRI head without IV contrast Variant 2: chronic headache with new feature or neurologic deficit 1) MRI head without and with IV contrast 2) MRI head without IV contrast 3) CT head without IV contrast 4) CT head without and with IV contrast 5) MRA head without and with IV contrast 6) MRA head without IV contrast Neuroimaging is not indicated in patients with a clear history of migraine, without red flag features for potential secondary headache, and a normal neurological examination
Do not refer people diagnosed with tension-type headache, migraine, cluster headache or medication overuse headache for neuroimaging solely for reassurance
Frequent episodic migraine - Brain MRI, Carotid ultrasound or MRA Migraine with aura-Brain MRI Migraine with brainstem aura- Brain MRI & MRA Carotid and vertebral arteries ultrasound/or CT or MRA Chronic migraine Brain-MRI Gd & MRV Complications of migraine-Brain MRI Persistence of aura symptoms- Emergency brain CT or MRI Carotid and vertebral arteries ultrasound/or CT or MRA Frequent TTH and chronic TTH-Brain MRI MRI Gd & MRV Grading of recommendation1) CS (G4) + qSR (IHE Database) 2) EO (G3) 3) EO (G1)
Variant 1: 1) 4, 2) 4 Variant 2: 1) 8, 2) 7, 3) 7, 4) 5, 5) 4, 6) 4 D: Evidence level 3 or 4; or extrapolated evidence from studies rated as 2 + Not availableNot available ACR = American College of Radiology, AGREE = Appraisal of Guidelines for Research & Evaluation, CS = case series, EO = expert opinion, Gd = gadolinium-enhanced, IHE = Integrating the Healthcare Enterprise, IV = intravenous, MRA = magnetic resonance angiograph, MRV = magnetic resonance venogram, TTH = tension type headache
사하였다. 권고문에 대한 동의 정도는 델파이 기법을 차용하여 조사하였는데 동의 점수의 평균을 사용하였다. 동의 정도는 1~3점(동의하지 않음), 4~6점(모르겠음), 7~9점(동의함)으로 나누어 정의 하였고, 응답 평균점수가 6점 미만일 때 동의도가 낮다고 보아 2차 조사를 시행하기로 하였다. 권 고문별 동의 정도 확인을 위하여 변이계수(coefficient variation; 이하 CV)를 산출하였는데 변이 계수가 작을수록 동의 정도가 일치한다고 보았기 때문에, 변이계수가 0.5 미만은 2차 조사 불필요, 0.5~0.8은 안정적이나 2차 조사 여부는 논의 후 결정, 0.8 초과는 추가 설문이 필요한 것으로 사전 에 정의하였다. 총 10명의 전문가로부터 권고문에 대한 동의 정도를 조사하였는데 핵심질문 1에 대한 동의 정도는 권고 1-1은 평균(표준편차) 8.2 (1.1), 권고 1-2는 7.2 (0.8), 권고 1-3은 6.8 (1.2) 였 으며 핵심질문 2에 대한 동의 정도는 권고 2-1은 7.8 (0.8), 권고 2-2는 7.7 (0.7) 였고 핵심질문 3에 대한 동의 정도는 권고 3-1은 7.6 (1.0), 권고 3-2는 7.5 (1.0)이었다. CV 점수는 모든 항목에서 0.5 미 만으로 나타나 2차 조사는 시행하지 않았다. 델파이 조사 시 기타의견도 함께 취합을 하였는데 총 7건의 의견이 제시되었다. 실무위원회에서 추가적인 논의를 거쳐 제시된 7건의 의견을 모두 반영 하여 권고문을 수정하였다.
외부검토 및 임상진료지침 승인
최종 권고문에 대한 검토와 의견 수렴을 위하여 임상의사, 시민, 환자단체, 언론, 유관학회, 질병 관리본부 등을 초청하여 2017년 10월 24일 공개 발표회(총 43명이 참여)를 진행하였다. 공개 발표 회에서 신경두경부 분과의 권고문에 대한 의견은 나오지 않았다. 이후 대한내과학회의 외부 검토 를 시행한 후 대한의학회의 임상진료지침 승인을 받았다.
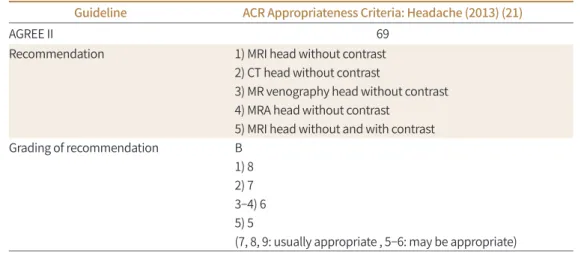
Table 3. Recommendation Matrices of the Existing Guidelines (Key Question 3)
Guideline ACR Appropriateness Criteria: Headache (2013) (21)
AGREE II 69
Recommendation 1) MRI head without contrast
2) CT head without contrast
3) MR venography head without contrast 4) MRA head without contrast
5) MRI head without and with contrast
Grading of recommendation B
1) 8 2) 7 3–4) 6 5) 5
(7, 8, 9: usually appropriate , 5–6: may be appropriate)
ACR = American College of Radiology, AGREE = Appraisal of Guidelines for Research & Evaluation, MRA = magnetic resonance angiograph
권고안
핵심질문 1. SAH가 의심되는 급성벼락두통(Thunderclap Headache) 환자에서 어떤 영상 검사를 권장하는가?
권고 1-1. 급성벼락두통을 주 호소로 내원하여 SAH가 의심되는 환자에서 영상 검사로 신속한 비조영 두부 CT 검사를 시행하여야 한다(권고등급A, 근거수준 III).
권고 1-2. 급성벼락 두통을 주 호소로 내원하여 SAH가 의심되는 환자에서, 동맥류성 출혈을 확 인하기 위해 CT 두부 혈관조영 검사는 권장된다(권고등급B, 근거수준 III).
권고 1-3. 급성벼락 두통을 주 호소로 내원하여 SAH가 의심되는 환자에서, 이전에 coil이나 stent로 시술받은 경우나 비조영 두부 CT가 이상소견이 없지만 지주막하출혈이 의심되는 경우 등 에 MRI 두부혈관 검사(조영 또는 비조영), 두부 MRI 검사 혹은 혈관조영술은 고려될 수 있다 (권 고등급B, 근거수준 IV).
근거요약
급성으로 갑작스럽게 생긴 심한(보통 인생에서 가장 심한 또는 극심한) 두통은 급성벼락두통으 로 지칭되기도 하며, 수 초 또는 수 분 이내에 통증의 최대 강도에 이르는 양상으로, 편두통이나 여 타의 두통과 구분된다. Harling 등(12)이 보고한 전향적 논문에 의하면, 급성벼락두통을 호소한 49명의 환자 중 35명에게서 지주막하 출혈이 보고되었으며, 마찬가지로 급성벼락두통을 호소한 환자에 대한 3개의 study를 종합하였을 때, 총 350명의 환자 중 165명의 환자(47%)에서 지주막하 출혈이 확인되었다(13-15). 따라서 급성벼락두통을 호소하는 환자에서 영상 검사는 신속하게 지 주막하 출혈의 유무를 확인하는 것을 주목적으로 하며, 일반적으로 비조영 두부 CT 검사가 그 기 본이 된다. 12시간 이내 촬영된 두부 CT의 경우 지주막하 출혈에 대한 민감도가 98%에 이르며 촬 영시간이 24시간으로 지연된 경우 민감도가 93%로 감소하게 된다(16). 또한 오진이 된 case의 73%에서 두부 CT 촬영에 실패했기 때문이라는 보고도 있다(17). 두부 CT 영상에서 이상이 없는 경우 지주막하 출혈의 확인을 위해 요추 천자가 추가로 시행되어야 한다(14, 15). CT 두부 혈관조 영 검사는 비침습적이며 뇌동맥류 발견에 있어 혈관조영검사와 비견되는 민감도, 특이도를 보이 고 있어 지주막하 출혈이 발견된 환자에서 추가적으로 자주 시행되고 있는 검사이다(18). 또한 McCormack과 Hutson (19)은 지주막하 출혈의 pretest probability가 15%인 경우 비조영 두부 CT와 CT 두부 혈관 조영 검사에서 모두 이상소견이 없는 경우 지주막하 출혈이 있을 확률은 1%
이하로 보고하였으며(19), Rana 등(20)은 CT 두부 혈관조영 검사에서 이상소견이 없는 경우, 요추 천자에서 출혈이 의심되는 경우라 할지라도 고식적 혈관조영 검사를 통해 동맥류성 출혈을 발견 할 추가적인 이득이 없는 것으로 보고하고 있다.
급성 지주막하 출혈이 발견된 환자에서 동맥류를 포함한 혈관 이상을 확인하기 위해 MRI 두부 혈관 검사와 혈관조영술을 시행할 수 있으며(21), 이때 조영 MRI 두부혈관 검사는 이전에 coil이 나 stent로 시술받은 경우, 포함된 금속으로 인해 생긴 왜곡으로 인한 영향을 줄일 수 있다(22).
Fluid-attenuated inversion recovery (이하 FLAIR), proton density, diffusion weighted imag-
ing, gradient echo (이하 GRE) 등을 포함한 두부 MRI 영상 검사의 경우, 비조영 두부 CT가 이상 소견이 없는 경우에 요추 천자 검사 등을 피하기 위해 추가적으로 고려해 볼 수 있다(23).
권고 고려사항 이득과 위해
급성벼락두통을 주 호소로 내원하여 SAH가 의심되는 환자의 1차 진단 영상 검사로 비조영 두 부 CT 검사를 사용하는 경우 방사선 피폭의 단점이 있으나, 비조영 두부 CT 검사를 통해 오진의 가능성을 줄이고, 치명률이 높은 지주막하 출혈을 배제함으로써 환자가 얻는 이득이 훨씬 크다고 판단된다.
국내 수용성과 적용성
진료지침의 국내 수용성과 적용성은 평가결과 큰 무리가 없는 것으로 판단되었다.
검사별 방사선량
(Supplementary Table 9 in the online-only Data Supplement) 비조영 두부 CTCT 두부 혈관조영 검사 MRI 두부혈관 검사 0 두부 혈관조영술
핵심질문 2. 신경학적 진찰이 정상인 비급성 두통의 경우 어떤 검사를 권장하는가?
권고 2-1. 신경학적 진찰이 정상인 비급성 두통 환자의 임상적 진찰에서 편두통이나 긴장성 두 통에 합당한 경우 영상의학적인 검사는 권장되지 않는다(권고등급 C, 근거수준 III).
권고 2-2. 2차성 두통의 원인 질환을 조사하기 위해 두부 MRI 검사를 우선 권장하며, 두부 CT는 MRI 장비의 가용성 및 방사선 노출 고려하에 제한적으로 사용하는 것을 권장한다(권고등급 B, 근 거수준 III).
근거요약
해당 핵심질문과 관련하여 4개의 관련 가이드라인이 검토되었다(5, 21, 24, 25). 신경학적 진찰 이 정상인 비급성 두통의 경우 대부분은 편두통이나 긴장성 두통으로 대표되는 1차성 두통으로 알려져 있다(26). 비특이적인 두통에서도 두부 영상 검사에서 기저 질환이 발견될 확률은 매우 낮 은 것으로 알려져 있으며(27-32) 신경학적 진찰이 정상인 비급성 두통 환자에서 CT나 MRI를 이용 한 검사상 관련성이 있는 병변이 발견될 확률은 더욱 낮은 것으로 보고되고 있다(0.2~1.4%) (26, 30, 33-37). 반면에 두부 MRI를 이용한 코호트 연구에서 증상을 유발하지 않는 우연한 병변이 발 견된 비율이 13.5%까지 보고되었으며(38) 이러한 우연한 발견이 환자의 불안감이나 의료비용을 변화시킬 수 있다는 점이 고려되어야 한다. 이러한 관점에서 모든 가이드라인은 편두통이나 긴장
성 두통의 전형적인 임상양상을 보이면서 신경학적 진찰이 정상인 비급성 두통의 경우에 CT나 MRI를 이용한 검사는 권장되지 않았으며 하나의 가이드라인에서는 부비동이나 경추의 X-선 검 사마저도 하지 않는 것을 권장하였다(24).
그러나 뇌종양으로 발생한 2차적인 두통의 경우에도 긴장형 두통이나 편두통으로 나타나는 경 우가 많듯이 뇌실질 병변에 의한 2차적 두통을 배제하는 것도 중요할 것으로 생각되며 이러한 이 차성 두통은 일반적으로 신경학적 이상소견을 동반하거나 이전과 다른 패턴을 보일 수 있으므로 (39) 신경학적 진찰에서 특이소견을 보이지 않는 비급성의 두통이라 할지라도 이전과 다른 양상의 두통으로 내원하였다면 영상 검사를 이용하여 2차성 두통의 원인 질환을 조사하는 것이 적절한 것으로 권장되었다(21, 24). CT와 비교하여 MRI는 뇌실질 병변의 진단에 있어 CT보다 우월한 민 감도를 보여 가장 권장되는 검사방법이나(21, 40, 41) 두통과 연관된 병변의 진단에는 CT와 유의 한 차이가 없다고 판단된 경우도 있어(41) 비용과 접근성 및 MRI 금기증에 해당하는 경우에는 CT 도 좋은 검사수단으로 권장될 수 있다.
권고 고려사항 이득과 위해
1차성 두통이 강력히 의심되는 환자에서 진단율이 낮은 검사를 배제함으로써 불필요한 방사선 노출, 우연히 발견된 병변으로 인한 불안감, 불필요한 의료비 지출 등을 막을 수 있다. 드물게 긴장 성 두통이나 편두통으로만 보이는 2차성 두통의 원인 질환을 진단하지 못할 수 있겠으나 이러한 경우는 매우 낮은 것으로 보고되어 있다. 2차성 두통이 의심되는 환자에서 조영 및 비조영 두부 MRI를 시행함으로써 원인이 되는 두개내 병변을 조기에 발견할 수 있다. 두부 MRI의 경우 방사 선 피폭이 없어 안전하게 사용 가능하나 CT의 경우에는 방사선 피폭이 발생하므로 이에 대한 고 려가 필요하다.
국내 수용성과 적용성
진료지침의 국내 수용성과 적용성은 평가결과 큰 무리가 없는 것으로 판단되었다.
검사별 방사선량
(Supplementary Table 9 in the online-only Data Supplement) 두부 CT핵심질문 3. 임산부에게 새로 생긴 두통의 경우 어떤 검사를 권장하는가?
권고 3-1. 임산부에게 신경학적 이상을 동반한 새로운 두통의 경우 비조영 두부 MRI가 적절하 다(권고등급 A, 근거수준 III).
권고 3-2. 뇌출혈의 가능성이 매우 높거나(갑자기 발생한 강한 두통, 및 동반된 뇌출혈을 시사하 는 임상 양상) MRI를 시행할 수 없는 경우에 비조영 두부 CT도 적절하다(권고등급 A, 근거수준 III).
근거요약
임산부에게서 발생하는 두통은 기질적 원인이 더 흔하게 확인된다(21). 두통은 임산부에서 흔하 게 관찰되지만, 새롭게 발생하는 두통의 경우 임상적인 조치가 필요하다. 한 후향적 연구에서 보 고한 바에 따르면 두통으로 응급실에 방문한 임산부 63명의 환자 중 17명(27%)에서 원인이 확인 되었다(6). 임산부에서 흔하게 발생하는 (전)자간증의 경우 신경학적 증상과 더불어 두통을 동반 하며, 적절한 진단과 치료가 필요하다(7). 이외에도 (전)자간증과 유사한 증상을 보일 수 있는 다양 한 질환들–가역적 뇌혈관 연축 증후군(reversible cerebral vasoconstriction syndrome), 정맥혈 전증 등의 진단을 위해서 영상 검사가 필요할 수 있다(7, 11). 그러나 영상 검사 과정에서 발생할 수 있는 방사선 피폭 및 조영제의 경우 임산부 및 태아에게 미치는 영향이 있으므로 신중하게 고려 되어야 하며(9, 10) 우선 조영제를 사용하지 않는 MRI가 권고된다. 현재까지 자기공명영상의 태아 및 임산부에 대한 위해는 정확하게 보고된 바 없으며 임산부에서 발생할 수 있는 (전)자간증을 포 함한 여러 질환 진단에 도움을 준다(7, 11). 정맥 및 정맥동 혈전증이 의심될 경우에 역시 조영증강 하지 않은 자기공명정맥조영술 혹은 출혈을 민감하게 확인할 수 있는 기법(susceptibility weight- ed imaging, GRE, FLAIR)을 추가로 시행하는 것을 고려할 수 있다. 또한 조영제를 사용하지 않는 자기공명혈관조영술의 경우 뇌동맥류 및 혈관연축을 진단하는 것에 도움이 될 수 있다.
CT의 경우 전리방사선의 피폭 위험 때문에 임산부에서 우선 고려할 수 있는 영상 검사로 적합 하지 않다. 더불어 임산부에서 발생하는 주요 질환인 (전)자간증 및 혈관 연축 진단에 가치가 높지 않다(7). 그러나 MRI의 경우 자체적인 금기증(폐소공포증, 심박동기를 포함한 자기공명영상 기기 에 부적합한 인체 삽입물을 보유한 경우) (9)이 있거나 혹은 환자가 처한 상황에서 MRI의 사용이 불가할 경우 제한적으로 뇌출혈의 진단을 위하여 조영제를 사용하지 않은 두부 CT 검사를 고려할 수 있다.
권고 고려사항 이득과 위해
MRI의 경우 전리방사선 피폭이 없어 임산부에서 먼저 고려할 수 있는 영상 검사이다. 또한 MRI의 경우 현재까지 태아에 대한 어떠한 위험도 보고된 바가 없다(9). CT 영상의 경우 임신시기 에 따라 전리방사선 피폭에 의한 위해가 달라질 수 있으므로 이에 따른 고려가 필요하다(10). 특 히 임신 15주 이내의 경우 피폭에 의해 뇌신경계 발달에 영향을 미칠 수 있다. 그러나 15주 이후에 는 매우 다량의 피폭이 확정적 영향을 유발할 수 있다. 다만 두 경우 모두 확률적 영향인 악성 종 양 발생에 대한 위험도가 증가할 수 있다. 두부 CT 촬영의 경우 태아가 위치하는 복부/골반부에서 거리가 있고 또한 직접적인 피폭은 없고 산란선에 의한 피폭이 주를 이루므로 이에 대한 설명이 필요하다.
국내 수용성과 적용성
진료지침의 국내 수용성과 적용성은 평가결과 큰 무리가 없는 것으로 판단되었다.
검사별 방사선량
(Supplementary Table 9 in the online-only Data Supplement) 비조영 두부 CT비조영 두부 MRI 0
요약
이번에 개발된 권고안은 다양한 상황에서 마주칠 수 있는 두통에 대한 근거기반의 임상진료 권 고안으로 수용개작 방법을 통해 개발되었다. 본 권고안은 SAH가 의심되는 급성벼락두통 환자에 서 신속한 비조영 두부 CT를 권고하며 동맥류성 출혈 확인을 위한 CT 두부 혈관조영 검사도 권고 한다. 신경학적 진찰이 정상인 비급성 두통 환자에서는 영상의학적 검사를 권하지 않으나 2차성 두통의 원인을 조사하기 위해 두부 MR을 권장한다. 임산부에게 신경학적 이상을 동반한 두통이 새로 생긴 경우에는 비조영 두부 MR을 권고한다. 이번 권고안은 두통을 진료하는 임상의들이 진 단 방법에 대한 결정을 내리는 데 많은 도움이 될 것으로 기대된다.
Supplementary Materials
The online-only Data Supplement is available with this article at http://dx.doi.org/10.3348/
jksr.2019.80.5.880.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Acknowledgments
This work was supported by the Korean Federation of Science and Technology Societies (KOFST) grant funded by the Korean government.
REFERENCES
1. Carville S, Padhi S, Reason T, Underwood M; Guideline Development Group. Diagnosis and management of headaches in young people and adults: summary of NICE guidance. BMJ 2012;345:e5765
2. Kim BK, Chu MK, Lee TG, Kim JM, Chung CS, Lee KS. Prevalence and impact of migraine and tension-type headache in Korea. J Clin Neurol 2012;8:204-211
3. Duncan CW, Watson DP, Stein A; Guideline Development Group. Diagnosis and management of headache in adults: summary of SIGN guideline. BMJ 2008;337:a2329
4. Cho WS, Kim JE, Park SQ, Ko JK, Kim DW, Park JC, et al. Korean clinical practice guidelines for aneurysmal subarachnoid hemorrhage. J Korean Neurosurg Soc 2018;61:127-166
5. Edlow JA, Caplan LR, O'Brien K, Tibbles CD. Diagnosis of acute neurological emergencies in pregnant and post-partum women. Lancet Neurol 2013;12:175-185
6. Ramchandren S, Cross BJ, Liebeskind DS. Emergent headaches during pregnancy: correlation between neurologic examination and neuroimaging. AJNR Am J Neuroradiol 2007;28:1085-1087
7. Expert Panel on MR Safety, Kanal E, Barkovich AJ, Bell C, Borgstede JP, Bradley WG Jr, et al. ACR guidance document on MR safe practices: 2013. J Magn Reson Imaging 2013;37:501-530
8. American College of Radiology. ACR-SPR Practice parameter for imaging pregnant or potentially pregnant adolescents and women with ionizing radiation. Available at. https://www.acr.org/-/media/ACR/Files/Prac- tice-Parameters/Pregnant-Pts.pdf. Published 2018. Accessed Oct 17, 2018
9. Mortimer AM, Bradley MD, Likeman M, Stoodley NG, Renowden SA. Cranial neuroimaging in pregnancy and the post-partum period. Clin Radiol 2013;68:500-508
10. Korean Academy of Medical Sciences. Development of evidence-based clinical imaging guidelines II. Avail- able at. http://www.guideline.or.kr/guide/view.php?number=55&cate=B. Published 2016. Accessed Oct 17, 2018
11. Korean Academy of Medical Sciences. Korean appraisal of guideline for research & evaluation II. Available at. http://guideline.or.kr/evaluation/sub3.php. Published 2016. Accessed Oct 17, 2018
12. Harling DW, Peatfield RC, Van Hille PT, Abbott RJ. Thunderclap headache: is it migraine? Cephalalgia 1989;9:87-90
13. Linn FH, Wijdicks EF, Van der Graaf Y, Weerdesteyn-van Vliet FA, Bartelds AI, Van Gijn J. Prospective study of sentinel headache in aneurysmal subarachnoid haemorrhage. Lancet 1994;344:590-593
14. Lledo A, Calandre L, Martinez-Menendez B, Perez-Sempere A, Portera-Sanchez A. Acute headache of recent onset and subarachnoid hemorrhage: a prospective study. Headache 1994;34:172-174
15. Van der Wee N, Rinkel GJ, Hasan D, Van Gijn J. Detection of subarachnoid haemorrhage on early CT: is lum- bar puncture still needed after a negative scan? J Neurol Neurosurg Psychiatry 1995;58:357-359
16. Al-Shahi R, White PM, Davenport RJ, Lindsay KW. Subarachnoid haemorrhage. BMJ 2006;333:235-240 17. Suarez JI, Tarr RW, Selman WR. Aneurysmal subarachnoid hemorrhage. N Engl J Med 2006;354:387-396 18. Jayaraman MV, Mayo-Smith WW, Tung GA, Haas RA, Rogg JM, Mehta NR, et al. Detection of intracranial an-
eurysms: multi-detector row CT angiography compared with DSA. Radiology 2004;230:510-518
19. McCormack RF, Hutson A. Can computed tomography angiography of the brain replace lumbar puncture in the evaluation of acute-onset headache after a negative noncontrast cranial computed tomography scan?
Acad Emerg Med 2010;17:444-451
20. Rana AK, Turner HE, Deans KA. Likelihood of aneurysmal subarachnoid haemorrhage in patients with nor- mal unenhanced CT, CSF xanthochromia on spectrophotometry and negative CT angiography. J R Coll Physicians Edinb 2013;43:200-206
21. Douglas AC, Wippold FJ 2nd, Broderick DF, Aiken AH, Amin-Hanjani S, Brown DC, et al. ACR appropriateness criteria headache. J Am Coll Radiol 2014;11:657-667
22. Silbert PL, Mokri B, Schievink WI. Headache and neck pain in spontaneous internal carotid and vertebral ar- tery dissections. Neurology 1995;45:1517-1522
23. Jeong HW, Seo JH, Kim ST, Jung CK, Suh SI. Clinical practice guideline for the management of intracranial aneurysms. Neurointervention 2014;9:63-71
24. Becker WJ, Findlay T, Moga C, Scott NA, Harstall C, Taenzer P. Guideline for primary care management of headache in adults. Can Fam Physician 2015;61:670-679
25. National Clinical Guideline Centre (UK). Headaches: Diagnosis and Management of Headaches in Young People and Adults. London: Royal College of Physicians (UK) 2012
26. Sempere AP, Porta-Etessam J, Medrano V, Garcia-Morales I, Concepción L, Ramos A, et al. Neuroimaging in the evaluation of patients with non-acute headache. Cephalalgia 2005;25:30-35
27. Becker LA, Green LA, Beaufait D, Kirk J, Froom J, Freeman WL. Use of CT scans for the investigation of head- ache: a report from ASPN, Part 1. J Fam Pract 1993;37:129-134
28. Demaerel P, Boelaert I, Wilms G, Baert AL. The role of cranial computed tomography in the diagnostic work- up of headache. Headache 1996;36:347-348
29. Jordan JE, Ramirez GF, Bradley WG, Chen DY, Lightfoote JB, Song A. Economic and outcomes assessment of magnetic resonance imaging in the evaluation of headache. J Natl Med Assoc 2000;92:573-578
30. Mitchell CS, Osborn RE, Grosskreutz SR. Computed tomography in the headache patient: is routine evalua- tion really necessary? Headache 1993;33:82-86
31. Reinus WR, Erickson KK, Wippold FJ 2nd. Unenhanced emergency cranial CT: optimizing patient selection with univariate and multivariate analyses. Radiology 1993;186:763-768
32. Weingarten S, Kleinman M, Elperin L, Larson EB. The effectiveness of cerebral imaging in the diagnosis of chronic headache. Arch Intern Med 1992;152:2457-2462
33. Cull RE. Investigation of late-onset migraine. Scott Med J 1995;40:50-52
34. Frishberg BM. The utility of neuroimaging in the evaluation of headache in patients with normal neurologic examinations. Neurology 1994;44:1191-1197
35. Nawaz M, Amin A, Qureshi AN, Jehanzeb M. Audit of appropriateness and outcome of computed tomogra- phy brain scanning for headaches in paediatric age group. J Ayub Med Coll Abbottabad 2009;21:91-93
36. Tsushima Y, Endo K. MR imaging in the evaluation of chronic or recurrent headache. Radiology 2005;235:
575-579
37. Wang HZ, Simonson TM, Greco WR, Yuh WT. Brain MR imaging in the evaluation of chronic headache in pa- tients without other neurologic symptoms. Acad Radiol 2001;8:405-408
38. Vernooij MW, Ikram MA, Tanghe HL, Vincent AJ, Hofman A, Krestin GP, et al. Incidental findings on brain MRI in the general population. N Engl J Med 2007;357:1821-1828
39. Forsyth PA, Posner JB. Headaches in patients with brain tumors: a study of 111 patients. Neurology 1993;43:
1678-1683
40. Evers S, Afra J, Frese A, Goadsby PJ, Linde M, May A, et al. EFNS guideline on the drug treatment of migraine--re- vised report of an EFNS task force. Eur J Neurol 2009;16:968-981
41. Hoang JK, Branstetter BF 4th, Gafton AR, Lee WK, Glastonbury CM. Imaging of thyroid carcinoma with CT and MRI: approaches to common scenarios. Cancer Imaging 2013;13:128-139
42. Edlow JA, Panagos PD, Godwin SA, Thomas TL, Decker WW; American College of Emergency Physicians.
Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emer- gency department with acute headache. Ann Emerg Med 2008;52:407-436
43. Meurer WJ, Walsh B, Vilke GM, Coyne CJ. Clinical guidelines for the emergency department evaluation of subarachnoid hemorrhage. J Emerg Med 2016;50:696-701
44. Mitsikostas DD, Ashina M, Craven A, Diener HC, Goadsby PJ, Ferrari MD, et al. European Headache Federa- tion consensus on technical investigation for primary headache disorders. J Headache Pain 2015;17:5
2017년 근거기반 임상영상 가이드라인에서 연구된 두통 환자 진단을 위한 한국형 영상 검사 권고안
정조성1 · 오세원1* · 장진희2 · 최치훈3 · 김수진4 · 문원진5 · 최미영6 · 정승은2
두통은 신경학적 문제를 일으키는 가장 흔한 질환으로 다양한 원인에 의해 발생할 수 있는 데, 환자의 임상양상과 상황에 따라 영상 검사의 유용성이 다를 수 있다. 대한영상의학회와 한국보건의료연구원은 환자를 진료하는데 필요한 영상 검사에 관한 통일된 근거기반의 가이 드라인을 개발하기로 하였으며 이 중 신경두경부 분과에서는 두통 환자 진료에서 임상적으 로 판단이 어려울 수 있는 상황을 선별하여 가이드라인 개발을 추진하였다. 가이드라인 개발 을 위하여 개발위원회와 실무위원회 그리고 자문위원회를 구성하였다. 개발위원회와 실무위 원회의 논의와 유관 전문학회의 자문을 통해 3가지 문장형 핵심질문을 선정하였고 기존 진 료지침을 근거로 하는 수용개작 개발방법을 통하여 최종 권고문을 도출하였다. 본 권고문은 다음과 같다. Subarachnoid hemorrhage가 의심되는 급성벼락두통 환자에서 신속한 비조 영 두부 CT를 권고하며 동맥류성 출혈 확인을 위한 CT 두부 혈관 조영검사도 권고한다. 신경 학적 진찰이 정상인 비급성 두통 환자에서는 영상의학적 검사를 권하지 않으나 2차성 두통 의 원인을 조사하기 위해 두부 MRI를 권장한다. 임산부에게 신경학적 이상을 동반한 두통이 새로 생긴 경우에는 비조영 두부 MRI를 권고한다.
1순천향대학교 천안병원 영상의학과,
2가톨릭대학교 의과대학 서울성모병원 영상의학과,
3충북대학교병원 영상의학과,
4서울대학교병원 강남센터 영상의학과,
5건국대학교 의과대학 건국대학교병원 영상의학과,
6한국보건의료연구원 보건의료근거연구본부