서 론
세계적으로 대장암 발생이 급격하게 증가하고 있는데 식단 서구 화와 신체활동 저하에 따른 비만 증가가 그 원인이라 할 수 있다.1) 대 장암 발생률은 지역에 따라 25배 정도의 차이를 보이며 소득수준이 높은 서구에서 발생률이 가장 높지만 중진국 및 개발도상국에서도 발생률이 증가하는 추세이다.2)
대장암의 주된 위험인자는 복부비만, 대장암 가족력, 염증성장질 환, 신체활동 부족, 흡연, 음주 등이며 2007년 The World Cancer Re-
search Fund (WCRF)와 American Institute for Cancer Research는 복부 비만을 ‘신뢰할 근거가 있는(confident evidence)’ 대장암의 위험인자 로 평가하였다.3) 대사증후군(metabolic syndrome, MS)은 제2형 당뇨 병과 심혈관질환의 전 단계로서 복부비만, 인슐린저항성, 이상지질 혈증, 고혈압으로 이루어진 대사이상상태이며, 복부비만이 주된 위 험인자이다.4)
‘유전-환경 상호작용(multiplegene-environment interaction)’이 MS 와 대장암의 공통된 질병 발생기전으로 제시되고 있으며, 대장암은
‘adenoma-carcinoma sequence,’5) MS는 ‘thrifty genotype hypothesis’4)가
Original Article
대장선종과 대사증후군 사이의 관련성, 성별에 따른 차이
도동희, 김성희*, 조윤정, 채승환
대구가톨릭대학 의과대학 가정의학교실
Association of Colorectal Adenoma with Metabolic Syndrome, Gender Difference
Dong Hee Do, Sung Hi Kim*, Yun Jeong Jo, Seung Hwan Chae
Department of Family Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea
Background: Insulin resistance and abdominal obesity are known as common risk factors for metabolic syndrome (MS) and colorectal cancer and account for increasing prevalence of both. On the other hand, colorectal adenoma is considered a precursor to colorectal cancer owing to its biological potential. Therefore, This study aimed to analyze the association of colorectal adenoma with MS and its components on sex difference.
Methods: This study included 3,954 participants (2,705 [68.4%] men and 1,249 [31.6%] women) who were classified into an adenoma group (n= 1,094) and a non-adenoma group (n= 2,860) based on results of histological tests and screening colonoscopy performed at a health check-up center between January, 2010, and December. MS was defined based on the National Cholesterol Education Program’s Adult Treatment Panel III (2006). The results of multiple logistic regression analysis are presented as odds ratio (OR) and 95% confidence intervals (CI).
Results: The OR of colorectal adenoma with MS was significantly increased in men (OR, 1.54; 95% CI, 1.29-2.65) after covariate adjustment, but not in women. Additionally, MS components were associated with increased ORs of colorectal adenoma, waist circumference (OR, 1.39; 95% CI, 1.13-1.71), triglyceride (OR, 1.83; 95% CI, 1.39-2.42), high density lipoprotein cholesterol (OR, 1,51; 95% CI, 1.15-1,98), systolic blood pressure (OR, 1.55; 95% CI, 1.18-2.04), and diastolic blood pressure (OR, 1.55; 95% CI, 1.17-2.06), but not fasting blood sugar; however, none of the ORs for other MS components were significant in women. The ORs of colorectal adenoma increased with age in both men and women.
Conclusion: Colorectal adenoma was independently associated with MS and its components, but not in women.
Keywords: Colorectal Neoplasm; Metabolic Syndrome; Sex Difference
http://www.kafm.or.kr/kjfp.2015.5.3.204 pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2015;5(3):204-211KJFP
Korean Journal of Family PracticeReceived August 27, 2014 Accepted August 28, 2015 Corresponding author Sung Hi Kim
Tel: +82-53-650-4247, Fax: +82-53-650-4122 E-mail: khmksh@cu.ac.kr
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
도동희 외. 대장선종과 대사증후군의 관련성 Korean Journal of Family Practice
KJFP
Original Article
Korean Journal of Family Practice 대표적이다. 복부비만, 인슐린저항성을 매개로 MS와 대장암은 연관
되어 있으며6) 최근 MS와 유방암, 난소암, 전립선암 사이의 관련성에 도 관심이 모아지고 있다.7) 또한 건강행동 측면에서 MS와 대장암의 위험인자는 대부분 겹쳐지고,3) MS와 대장암 모두 1차 예방 및 관리 측면에서 적정 체중, 신체활동 증가, 금연, 적정 음주 등의 건강행동 개선이 효과적인 방법으로 활용되고 있다.8)
대장암은 대부분 대장선종에서 ‘adenoma–carcinoma sequence’과 정을 거쳐서 진행하기 때문에 대장선종은 대장암의 대리지표라 할 수 있으며 일반 인구집단을 대상으로 대장선종 위험도를 평가하여 대장암의 위험을 추정할 수 있다.9) 서구의 다수 연구들에서 비만, MS, 대장선종/대장암(대장종양)의 관련성은 복합적이고 남녀에 따 라 차이가 있었으나10) 최근 메타분석이 활발하게 시행되면서 정도의 차이가 있지만 남녀 모두에서 비만, MS는 대장종양의 위험을 증가시 키는 쪽으로 의견이 모아지고 있다.11)
국내에서도 건강검진 수진자를 대상으로 MS와 대장종양의 관련 성 연구가 활발히 시행되고 있으나 남녀로 구분하여 분석하는 경우 는 드문 편으로,12-15) 성별에 따라서 MS 유병률과 대장종양 유병률에 차이가 있기 때문에 MS와 대장종양 관련성 분석 시에 성별을 구분하 여 분석하는 것은 의미가 있으며, 본 연구는 건강검진 수검자를 대상 으로 하여 남녀별로 MS와 대장선종의 관련성을 알아보고자 하였다.
방 법
1. 연구대상
2010년 1월에서 2012년 12월까지 대구가톨릭대학교병원 검진센터 에서 대장내시경검사를 시행한 4,457명을 대상으로 하였다. 이 중에 서 대장암의 과거력이 있거나, MS 목표 질환인 당뇨병, 허혈성심질환 및 뇌혈관질환의 과거력이 있는 191명을 먼저 제외하고, 이후 과증식 성 용종(301명), 기타 용종(serrated polyp, 6명) 및 대장암(5명)을 제외 하여 3,954명(남자 2,705명, 여자 1,249명)을 분석대상으로 하였다.
2. 연구방법
1) 대장용종에 따른 구분
Long flexible colonoscope을 이용하여 회맹부까지 검사를 시행하 였으며, 용종의 병리조직 결과를 선종성(융모형 포함), 과증식성, 염 증성용종으로 구분하였다. 용종의 위치(우측, 좌측), 크기(2-30 mm), 개수(1-9개)와는 관계없이 선종성 용종만을 환자군에 포함시켰고 염 증성용종을 포함한 비용종군을 대조군으로 하였다.
2) 대사증후군의 정의
본 연구에서는 National Cholesterol Education Program’s Adult Treatment Panel III (2006)에서 제시하고 있는 MS의 진단기준을 기본 으로 World Health Organization West Pacific Region에서 권고하고 있 는 복부비만기준을 이용한 수정된 진단기준을 이용하였고4) 다음 5 가지 항목 중 3가지 이상을 만족하는 경우로 하였다. (1) 복부비만(허 리둘레): 남자 ≥90 cm, 여자 ≥80 cm; (2) 고혈압: ≥130/85 mm Hg 또 는 약물치료; (3) 고중성지방혈증: ≥150 mg/dL 또는 약물치료; (4) 고 혈당: 공복혈당 ≥100 mg/dL 또는 약물치료; (5) 저 고밀도지단백 콜 레스테롤(high density lipoprotein cholesterol, HDLC) 혈증: 남자 <40 mg/dL, 여자 <50 mg/dL.
3) 일반적 특성
자기기입식 설문지를 이용하여 자료를 수집하였다. 교육수준은 고졸 미만, 고졸 이상 대졸 미만, 대졸 이상으로 구분하였고, 흡연상 태는 현재흡연, 과거흡연, 비흡연으로 구분하였고, 음주상태도 현재 음주, 과거음주, 비음주로 구분하였다.
4) 신체계측 및 혈액검사
신체계측은 직립자세에서 신장, 몸무게를 측정하여 체질량지수 (body mass index, BMI; kg/m2)를 구하였다. 허리둘레는 직립한 상태 로 장골능(iliac crest) 수준에서 줄자를 이용하여 측정하였다. 혈압은 최소 5분 이상 휴식 후, 자동혈압계를 이용하여 수축기혈압, 이완기 혈압을 측정하였으며, 2회 이상 반복 측정 후 평균값을 구하였다. 혈 액검사는 최소 8시간 이상의 공복 후 상완정맥에서 혈액을 채취하였 으며, 공복혈당, 중성지방, HDLC, 저밀도지단백 콜레스테롤(low den- sity lipoprotein cholesterol, LDLC), 총 콜레스테롤(total cholesterol, TC) 및 요산 농도를 측정하였다.
3. 자료 분석
IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA)을 이용하였고 유의 성 검정은 P<0.05에서 시행하였다. MS 및 MS 요소에 따른 대장선종 교차비는 남, 여로 구분하여 다중 로지스틱회귀분석을 시행하였다.
분석 시 공변량은 연령, 교육수준, 흡연상태, 음주상태를 이용하였 다. 일반적 특성에서 대장선종 여부에 따른 교육수준, 흡연상태, 음 주상태의 비교는 chi-square test를 시행하였고, BMI, 허리둘레, 공복 혈당, 중성지방, HDLC, 수축기/이완기혈압 및 TC, LDLC, uric acid 비 교는 t-test를 시행하였다. 분석 시 고혈압 병력이 있으면 측정 혈압수 준에 관계없이 MS의 고혈압 요소를 포함하는 것으로 처리하였다.
Dong Hee Do, et al. The Association of Colorectal Adenoma with Metabolic Syndrome
Korean Journal of Family Practice
KJFP
결 과
1. 조사대상자들의 일반적 특성과 혈액검사
전체 대상자 3,954명 중에서 68.4% (2,705명)은 남자였고 31.6%
(1,249명)는 여자였다. 대장선종의 유병률은 전체에서는 30.4%였으며 남자 31.3%, 여자 19.9%로 남자의 유병률이 더 높았으며 남, 여 모두에 서 대장선종군이 대조군과 비교하여 연령이 많고 교육수준이 낮았 으며 남자는 흡연을 더 많이 하고 여자는 음주를 적게 하는 것으로 나타났다. 또한 남, 여 모두에서 대장선종군에서 MS 유병률이 높았 고, 복부비만, 공복혈당, 중성지방, 수축기/이완기혈압이 높았다.
LDLC, TC, 요산은 여자에서만 대장선종군이 대조군에 비하여 높게 나타났다(Table 1).
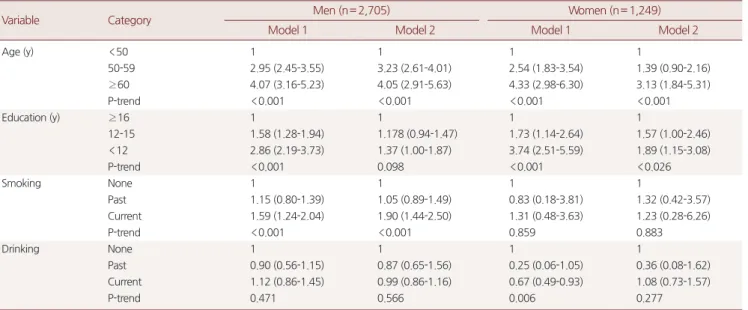
2. 남녀별 연령, 교육수준, 흡연 및 음주상태에 따른 대장선종 교차비
공변량 보정 후 남자에서는 40대와 비교하여 60대 이상의 대장선 종 교차비가 4.05 (2.91-5.63)로 증가하였고, 대졸 이상과 비교하여 고 졸 미만에서는 2.84 (2.19-3.73), 비흡연자와 비교하여 현재 흡연자에 서는 1.90 (1.44-2.50)으로 증가하였다. 여자에서는 대장선종 교차비 가 연령이 많을수록 2.99 (1.76-5.09)로 증가하였고 교육수준이 낮을 수록 1.89 (1.15-3.08)으로 증가하였다(Table 2).3. 남녀별 대사증후군 및 대사증후군 요소에 다른 대장선종 교차비
공변량(연령, 교육수준, 흡연, 음주)을 보정하지 않은 상태에서, MS 가 동반된 경우에 대장선종 교차비는 남, 여에서 각각 1.62 (1.34-1.96), 1.85 (1.29-2.65)로 증가하였다. MS 요소들은 남자에서는 허리둘레, 공 Table 1. General characteristics of participants according to gender and colorectal adenoma statusCharacteristic
Men (n= 2,705) Women (n= 1,249)
Control (n= 1,859)
Adenoma
(n= 846) P-value Control (n= 1,001)
Adenoma
(n= 248) P-value
Age* (y) 46.12± 9.07 52.20± 8.94 0.000 48.24± 9.64 54.58± 9.58 0.000
Education (y)† 0.000 0.000
<12 164 (8.8) 164 (19.4) 252 (25.2) 119 (47.8)
12-15 452 (24.3) 248 (29.3) 347 (34.7) 77 (31.3)
≥ 16 1,243 (66.9) 434 (51.3) 402 (40.1) 52 (20.9)
Smoking status 0.000 0.847
None 398 (21.4) 140 (16.6) 969 (96.8) 240 (96.4)
Past 757 (40.7) 309 (36.5) 12 (1.2) 2 (1.0)
Current 704 (37.9) 397 (46.9) 20 (2.0) 6 (2.6)
Drinking status 0.465 0.014
None 247 (13.3) 122 (14.4) 570 (56.9) 167 (67.2)
Past 82 (4.4) 44 (5.2) 34 (3.4) 2 (1.0)
Current 1,530 (82.3) 680 (80.4) 397 (39.7) 79 (31.8)
BMI (kg/m2) 24.58± 2.84 24.90± 2.84 0.008 23.12± 2.94 23.85± 2.82 0.000
BMI≥ 25 kg/m2 42.0 45.9 0.034 22.9 29.0 0.028
Prevalence of metabolic syndrome 18.6 26.3 0.000 12.7 21.2 0.001
WC (cm) 85.59± 7.61 87.21± 7.46 0.000 76.07± 7.58 78.44± 7.35 0.000
WC≥ 90 cm in men and WC≥ 80 cm in women 28.4 36.1 0.000 31.5 41.7 0.002
FBS (mg/dL) 91.20± 17.82 93.27± 19.60 0.007 89.20± 14.19 92.15± 21.20 0.008
FBS ≥ 100 mg/dL 17.6 23.3 0.000 13.6 18.4 0.057
TG (mg/dL) 127.39± 83.64 145.97± 99.98 0.000 79.64± 54.35 91.98± 55.33 0.001
TG≥ 150 mg/dL 27.9 37.0 0.000 7.8 11.7 0.035
HDLC (mg/dL) 52.86± 13.00 51.40± 13.05 0.007 63.01± 14.85 60.92± 15.14 0.048
HDLC<40 mg/dL in men and HDLC<50 mg/dL in women 12.0 16.3 0.002 18.7 25.2 0.001
SBP (mm Hg) 126.17± 14.43 128.81± 13.61 0.000 120.44± 15.00 124.52± 14.78 0.000
DBP (mm Hg) 76.59± 10.45 78.07± 9.67 0.000 73.06± 9.86 74.67± 9.83 0.022
SBP≥ 130 mm Hg or DBP≥ 85 mm Hg 48.1 59.8 0.000 31.3 46.8 0.000
Low density lipoprotein cholesterol (mg/dL) 131.1± 32.8 130.2± 32.7 0.571 123.9± 33.6 136.6± 34.9 0.000
Total cholesterol (mg/dL) 196.2± 35.5 197.1± 35.2 0.555 192.8± 35.1 204.0± 36.3 0.000
Uric acid (mg/dL) 6.01± 1.26 6.06± 1.29 0.330 4.21± 0.92 4.37± 0.99 0.014
Values are presented as mean± standard deviation or number (%). Values of SBP and DBP were excluded hypertension patients, who have medication (n= 336).
BMI, body mass index; WC, waist circumference; FBS, fasting blood sugar; TG, triglyceride; HDLC, high density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure.
*Age, BMI, WC, FBS, TG, HDLC, SBP, DBP, LDL, uric acid. †Education level, smoking status, dringking status, BMI≥ 25, prevalence of metabolic syndrome, WC≥ 90 in men WC≥ 80 in women, FBS≥ 100, TG≥ 150, HDLC<40 in men HDLC<50 in women, SBP≥ 130 or DBP≥ 85.
도동희 외. 대장선종과 대사증후군의 관련성 Korean Journal of Family Practice
KJFP
복혈당, 중성지방, HDLC, 혈압 모두에서 MS 기준에 해당되는 경우 대장선종 교차비는 증가하였고 여자에서는 공복혈당을 제외한 요 소들에서 교차비가 증가하였다.
공변량 보정 후 MS 동반 시 대장선종 교차비는 남자에서 1.54 (1.29- 2.65)로 증가하였으나 여자는 유의하지 않았다. MS 요소별 대장선종 교차비 증가는 공복혈당을 제외한 허리둘레 1.39 (1.13-1.71), 중성지방
1.46 (1.20-1.78), HDLC 1.52 (1.15-2.00), 혈압 1.31 (1.08-1.58)로 증가하였 던 반면, 여자에서는 모든 요소들에서 유의하지 않았다(Table 3).
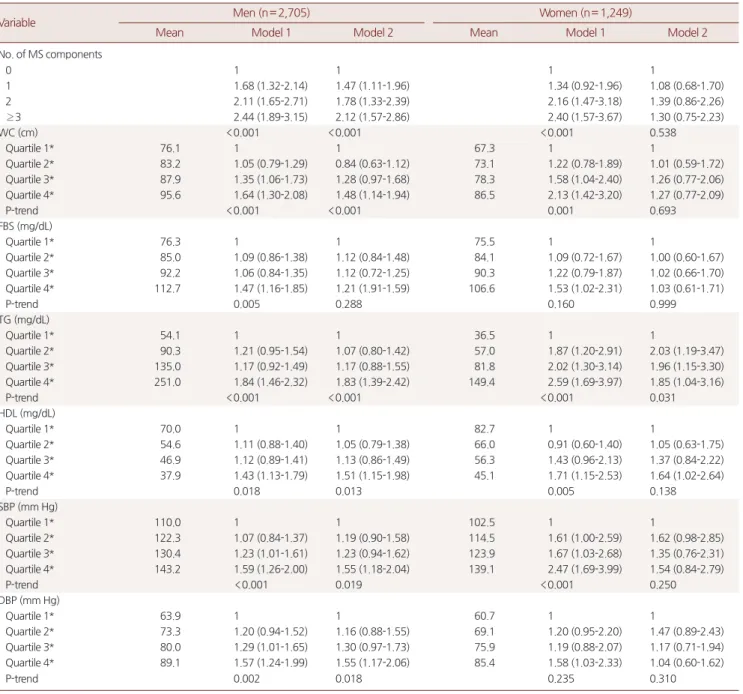
4. 남녀별 대사증후군 수 및 대사증후군 요소들의 사분위수에 따른 대장선종 위험도
공변량 보정 전 MS 요소 개수가 증가할수록 대장선종 교차비는 Table 2. Odds ratios and 95% confidence intervals for colorectal adenoma according to gender and age, education, smoking status, drinking sta- tus
Variable Category Men (n= 2,705) Women (n= 1,249)
Model 1 Model 2 Model 1 Model 2
Age (y) <50 1 1 1 1
50-59 2.95 (2.45-3.55) 3.23 (2.61-4.01) 2.54 (1.83-3.54) 1.39 (0.90-2.16)
≥ 60 4.07 (3.16-5.23) 4.05 (2.91-5.63) 4.33 (2.98-6.30) 3.13 (1.84-5.31)
P-trend <0.001 <0.001 <0.001 <0.001
Education (y) ≥ 16 1 1 1 1
12-15 1.58 (1.28-1.94) 1.178 (0.94-1.47) 1.73 (1.14-2.64) 1.57 (1.00-2.46)
<12 2.86 (2.19-3.73) 1.37 (1.00-1.87) 3.74 (2.51-5.59) 1.89 (1.15-3.08)
P-trend <0.001 0.098 <0.001 <0.026
Smoking None 1 1 1 1
Past 1.15 (0.80-1.39) 1.05 (0.89-1.49) 0.83 (0.18-3.81) 1.32 (0.42-3.57)
Current 1.59 (1.24-2.04) 1.90 (1.44-2.50) 1.31 (0.48-3.63) 1.23 (0.28-6.26)
P-trend <0.001 <0.001 0.859 0.883
Drinking None 1 1 1 1
Past 0.90 (0.56-1.15) 0.87 (0.65-1.56) 0.25 (0.06-1.05) 0.36 (0.08-1.62)
Current 1.12 (0.86-1.45) 0.99 (0.86-1.16) 0.67 (0.49-0.93) 1.08 (0.73-1.57)
P-trend 0.471 0.566 0.006 0.277
Model 1: crude. Model 2: adjusted for age, education level, smoking status, drinking status.
Table 3. Odds ratios and 95% confidence intervals for colorectal adenoma according to gender and MS, five MS components
Variable Men (n= 2,705) Women (n= 1,249)
Model 1 Model 2 Model 1 Model 2
MS
No 1 1 1 1
Yes 1.62 (1.34-1.96) 1.54 (1.23-1.93) 1.85 (1.29-2.65) 1.17 (0.76-1.82)
Waist circumference (cm)
≥ 90 in men, ≥ 80 in women 1 1 1 1
<90 in men, <80 in women 1.42 (1.19-1.69) 1.39 (1.13-1.71) 1.63 (1.22-2.15) 1.13 (0.80-1.62) Fasting blood sugar (mg/dL)
<100 1 1 1 1
≥ 100 1.42 (1.16-1.73) 1.25 (0.99-1.58) 1.43 (0.99-2.06) 0.98 (0.62-1.54)
Triglyceride (mg/dL)
<150 1 1 1 1
≥ 150 1.44 (1.22-1.70) 1.46 (1.20-1.78) 1.59 (1.10-2.30) 1.28 (0.85-1.94)
High density lipoprotein cholesterol (mg/dL)
≥ 40 in men, ≥ 50 in women 1 1 1 1
<40 in men, <50 in women 1.50 (1.21-1.87) 1.52 (1.15-2.00) 1.40 (1.01-1.98) 1.28 (0.85-1.94) BP (mm Hg)
SBP<130 and DBP<85 1 1 1 1
SBP≥ 85 or DBP≥ 85 1.43 (1.21-1.68) 1.31 (1.08-1.58) 1.65 (1.23-2.22) 1.02 (0.71-1.48)
Model 1: crude. Model 2: adjusted for age, education level, smoking status, drinking status.
MS, metabolic syndrome; BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Dong Hee Do, et al. The Association of Colorectal Adenoma with Metabolic Syndrome
Korean Journal of Family Practice
KJFP
남, 여 모두에서 증가하였으나 공변량 보정 후에는 남자에만 MS 요 소 0개와 비교하여 ≥3개에서 교차비가 2.12 (1.57-2.86)로 증가하였고 여자에서는 유의하지 않았다. MS 요소들을 사분위하여 제1사분위 를 기준으로 대장선종 교차비를 구하였다(HDLC는 역으로 제4사분 위를 기준). 남자에서는 공변량 보정 전 허리둘레, 공복혈당, 중성지 방, 수축기/이완기혈압이 높을수록, HDL이 낮을수록 교차비가 증가
하였고, 공변량 보정 후에도 공복혈당을 제외한 다른 요소들에서 요 소 개수가 증가할수록 선형적인 교차비 증가를 보이었으나 여자에 서는 공변량 보정 전에는 공복혈당, 이완기혈압을 제외한 대부분 요 소 등에서 대장선종 교차비가 선형적으로 증가하였으나 공변량 보 정 후에는 중성지방을 제외한 대부분의 요소들에서 유의한 차이가 없었다(Table 4).
Table 4. Odds ratios and 95% confidence intervals for colorectal adenoma according to gender and MS, five components of MS
Variable Men (n= 2,705) Women (n= 1,249)
Mean Model 1 Model 2 Mean Model 1 Model 2
No. of MS components
0 1 1 1 1
1 1.68 (1.32-2.14) 1.47 (1.11-1.96) 1.34 (0.92-1.96) 1.08 (0.68-1.70)
2 2.11 (1.65-2.71) 1.78 (1.33-2.39) 2.16 (1.47-3.18) 1.39 (0.86-2.26)
≥ 3 2.44 (1.89-3.15) 2.12 (1.57-2.86) 2.40 (1.57-3.67) 1.30 (0.75-2.23)
WC (cm) <0.001 <0.001 <0.001 0.538
Quartile 1* 76.1 1 1 67.3 1 1
Quartile 2* 83.2 1.05 (0.79-1.29) 0.84 (0.63-1.12) 73.1 1.22 (0.78-1.89) 1.01 (0.59-1.72)
Quartile 3* 87.9 1.35 (1.06-1.73) 1.28 (0.97-1.68) 78.3 1.58 (1.04-2.40) 1.26 (0.77-2.06)
Quartile 4* 95.6 1.64 (1.30-2.08) 1.48 (1.14-1.94) 86.5 2.13 (1.42-3.20) 1.27 (0.77-2.09)
P-trend <0.001 <0.001 0.001 0.693
FBS (mg/dL)
Quartile 1* 76.3 1 1 75.5 1 1
Quartile 2* 85.0 1.09 (0.86-1.38) 1.12 (0.84-1.48) 84.1 1.09 (0.72-1.67) 1.00 (0.60-1.67)
Quartile 3* 92.2 1.06 (0.84-1.35) 1.12 (0.72-1.25) 90.3 1.22 (0.79-1.87) 1.02 (0.66-1.70)
Quartile 4* 112.7 1.47 (1.16-1.85) 1.21 (1.91-1.59) 106.6 1.53 (1.02-2.31) 1.03 (0.61-1.71)
P-trend 0.005 0.288 0.160 0.999
TG (mg/dL)
Quartile 1* 54.1 1 1 36.5 1 1
Quartile 2* 90.3 1.21 (0.95-1.54) 1.07 (0.80-1.42) 57.0 1.87 (1.20-2.91) 2.03 (1.19-3.47)
Quartile 3* 135.0 1.17 (0.92-1.49) 1.17 (0.88-1.55) 81.8 2.02 (1.30-3.14) 1.96 (1.15-3.30)
Quartile 4* 251.0 1.84 (1.46-2.32) 1.83 (1.39-2.42) 149.4 2.59 (1.69-3.97) 1.85 (1.04-3.16)
P-trend <0.001 <0.001 <0.001 0.031
HDL (mg/dL)
Quartile 1* 70.0 1 1 82.7 1 1
Quartile 2* 54.6 1.11 (0.88-1.40) 1.05 (0.79-1.38) 66.0 0.91 (0.60-1.40) 1.05 (0.63-1.75)
Quartile 3* 46.9 1.12 (0.89-1.41) 1.13 (0.86-1.49) 56.3 1.43 (0.96-2.13) 1.37 (0.84-2.22)
Quartile 4* 37.9 1.43 (1.13-1.79) 1.51 (1.15-1.98) 45.1 1.71 (1.15-2.53) 1.64 (1.02-2.64)
P-trend 0.018 0.013 0.005 0.138
SBP (mm Hg)
Quartile 1* 110.0 1 1 102.5 1 1
Quartile 2* 122.3 1.07 (0.84-1.37) 1.19 (0.90-1.58) 114.5 1.61 (1.00-2.59) 1.62 (0.98-2.85)
Quartile 3* 130.4 1.23 (1.01-1.61) 1.23 (0.94-1.62) 123.9 1.67 (1.03-2.68) 1.35 (0.76-2.31)
Quartile 4* 143.2 1.59 (1.26-2.00) 1.55 (1.18-2.04) 139.1 2.47 (1.69-3.99) 1.54 (0.84-2.79)
P-trend <0.001 0.019 <0.001 0.250
DBP (mm Hg)
Quartile 1* 63.9 1 1 60.7 1 1
Quartile 2* 73.3 1.20 (0.94-1.52) 1.16 (0.88-1.55) 69.1 1.20 (0.95-2.20) 1.47 (0.89-2.43)
Quartile 3* 80.0 1.29 (1.01-1.65) 1.30 (0.97-1.73) 75.9 1.19 (0.88-2.07) 1.17 (0.71-1.94)
Quartile 4* 89.1 1.57 (1.24-1.99) 1.55 (1.17-2.06) 85.4 1.58 (1.03-2.33) 1.04 (0.60-1.62)
P-trend 0.002 0.018 0.235 0.310
Values of SBP and DBP of hypertension patients, who have medication were excluded (n= 336). Model 1: crude. Model 2: adjusted for age, education level, smoking status, drinking status.
MS, metabolic syndrome; WC, waist circumference; FBS, fasting blood sugar; TG, triglyceride; HDLC, high density lipoprotein cholesterol; SBP, Systolic blood pressure;
DBP, diastolic blood pressure.
*Quartile cut-off values: WC, 77.0, 83.2, 89.1 cm; FBS, 82, 88, 96 mg/dL; TG, 62, 95, 145 mg/dL; HDLC, 63.9, 53.3, 45.3 mg/dL; SBP, 116, 125, 134 mm Hg; DBP, 69, 76, 82 mm Hg.
도동희 외. 대장선종과 대사증후군의 관련성 Korean Journal of Family Practice
KJFP
고 찰
본 연구에서 남자의 경우 MS 및 MS 요소는 대장선종과 양의 관련 성이 있었으나 여자에서는 유의하지 않았으며, 남자에서는 흡연을 하는 경우, 여자에서는 교육수준이 낮은 경우에 대장선종 위험이 증 가하였다. MS뿐만 아니라 대장종양도 환경질환이라는 인식이 널리 받아들여지고 있는데,16,17) 대장암은 20세기 이전에는 드문 편이었으 나 이후 발생이 급격하게 증가하였고, 세계적으로 지역에 따라 발생 률 차이가 25배 이상이며, 이민자 연구에서 생활습관 서구화에 의해 인종적 차이가 소실된 점 등에서 건강행동을 포함한 환경적 영향을 추정할 수 있다.3)
복부비만과 신체활동 저하가 MS와 대장종양의 공통 위험요인으 로 알려지면서 MS와 대장종양의 관련성이 제기되었고,18) 다수의 역 학적 연구들에서 MS가 동반된 경우 대장종양의 위험이 증가하였 다.19) MS는 인슐린저항을 유발하여 insulin-like growth factors, aroma- tase 활성화, adipokines, angiogenesis, 산화적 스트레스/DNA 손상 등 의 경로를 통해서 암 발생 위험을 높이는 것으로 보고되고 있다.20) 서 구의 전향적 연구와21) 중국,22) 일본19) 그리고 국내의 단면연구12,15,23,24)
에서도 MS에서 대장선종의 상대위험도와 교차비가 증가하였고 MS 요소 개수와는 양의 용량-반응 관련성이 있었다.
MS 요소들 중에서 비만은 혈중 유리지방산(free fatty acids) 증가, 간의 당신생(gluconeogenesis) 및 중성지방 증가와 인슐린저항성을 유 발하여 대장종양의 위험을 포괄적으로 증가시켰으며25) 대장종양이 동반된 경우 중성지방이 높았고,26) HDLC가 높은 군에서 대장종양 발생이 저하되었다.22) 고혈압과 대장종양의 관련성에서는 염분 민감 성 고혈압의 경우 AMP-activated protein kinase(에너지 대사 조절인 자; 에너지 생성을 활성화하고 생합성경로[biosybtheric]를 억제함)가 억제되어 대장종양의 위험이 증가하였다.27)
대장암 위험요인 중에서 연령의 영향이 가장 강력하고 실제로 대 장암의 95% 이상은 50세 이상에서 발생하는 것으로 보고되고 있으 며,28) 흡연은 대장선종의 위험을 높이고,29) 사회경제적 수준이 낮을 수록 대장암 발생률이 증가하였는데30) 본 연구에서도 이와 유사한 결과들을 보이었다.
본 연구에서 공변량(연령, 교육수준, 흡연상태, 음주상태) 보정 전 에는 남, 여 모두에서 MS와 MS 요소와 대장선종의 교차비는 양의 양-반응 관련성을 보이었으나, 공변량 보정 후 남자는 MS와 MS 요소 에 따라서 대장선종 교차비가 증가하였으나 여자에서는 연령을 보 정하면서 중성지방을 제외한 대부분의 유의성이 소실되었다. 다른 연구들에서도 남, 여로 구분하여 분석하는 경우, 남자에서만 관련성 이 있었고 여자에서는 유의하지 않은 경우가 대부분 이었으며,10) 성
별에 따른 위험요인의 차이가 일부 연구의 논쟁점 이었으나 최근의 메타연구들에 따르면 남, 여 모두에서 MS와 대장종양은 유의한 관 련성이 있었는데,11) 본 연구에서 여자의 경우 MS와 대장선종의 관련 성에서 연령이 주요 혼란변수임을 추정할 수 있다. 지역, 인종, 연령 등의 다양한 차이에도 불구하고 여자의 대장종양 유병률은 남자의 절반 정도로 보고되고 있으며 이외에도 여자의 대장종양 발생 시기 가 늦고 조직타입이 상대적으로 양호한 편이었으며,28) 이러한 남녀별 차이는 건강행동(비만, 흡연, 음주, 식이요인, 신체활동량)의 차이와 관련되어 있지만 MS와 대장종양을 동시에 예방하는 여성호르몬(es- trogen/progesteron) 효과가 주된 원인으로 추정되고 있다.10,11)
효율적인 대장암 관리방법은 대장내시경을 시행하여 대장선종을 발견 및 제거하는 2차 예방(단기 효과)과 생활습관 개선을 통해 종양 의 발생률을 낮추는 1차 예방(장기 효과)을 병행하는 것이라 할 수 있으며, 최근 서구에서는 대장내시경 screening과 생활습관 개선에 의해 대장암의 발생률과 사망률이 감소하고 있다.2) 그러나 국내에서 는 아직까지 발생률, 사망률 모두 증가하는 추세여서23) 보다 적극적 인 1, 2차 예방의 실천이 필요하다고 할 수 있으며, 본 연구에서는 MS 가 동반된, 남자, 고령자, 사회경제적 수준이 낮은 경우가 예방활동의 우선 대상이라 할 수 있는 고위험군에 해당되었다.
본 연구의 제한점으로는 먼저, 일개 병원 건강검진센터에 국한되 어 선택편견에 의한 일반화의 어려움이 있고 단면연구여서 MS와 대 장선종 사이의 시간적 전후 관계 추정이 어려운 점과 둘째, 개개인의 건강행동에 대한 세밀한 정보수집이 부족한 점으로 음주의 경우 이 미 WCRF에서 충분한 대장암의 위험요인으로 확인이 되었지만 본 연구에서는 음주상태에 따른 선종 유병률의 차이가 없었으며, 신체 활동량 정보가 수집되지 않은 점이 그 예들이라고 할 수 있고 셋째, 남, 여의 성별 차이를 설명하는 중요 변수인 폐경 여부와 여성호르몬 사용 정보가 수집되지 않아서 여자의 연령보정 후 통계적 유의성이 소실되는 점은 위의 제한점과 관련이 있을 수 있다. 마지막으로 이전 의 대장내시경검사 및 선종 여부에 대한 정보가 없는 점이 MS와 대 장선종의 관련성을 약화시키는 쪽으로 작용할 수 있다. 그러나 본 연 구는 비교적 다수를 조사대상으로 하였고 남, 여로 구분하여 연령, 흡연, 교육수준, 질병상태를 보정한 후 MS와 대장선종의 관련성을 알아보고자 한 점에서 의미가 있다고 할 수 있다.
요 약
연구배경:
인슐린저항성, 복부비만은 대사증후군과 대장암의 공통 된 위험요인으로 알려져 있다. 또한 대장선종은 대장암의 선행질환 으로 대장암의 위험도를 반영한다. 본연구에서는 대장선종과 대사Dong Hee Do, et al. The Association of Colorectal Adenoma with Metabolic Syndrome
Korean Journal of Family Practice
KJFP
증후군 및 대사증후군 요인들간의 관련성을 알아보고자 하였다.
방법:
연구대상자는 3,954명(남자 2,705명[68.4%], 여자 1,249명 [31.6%]) 으로 2010년 1월에서 12월까지 대구가톨릭대학교병원 검진 센터에서 스크리닝 대장내시경검사를 시행하였다. 연구대상자들은 조직검사에 따라 선종군(n=1,094)과 비선종군(n=2,860)으로 구분 하였고, modified National Cholesterol Education Program’s Adult Treatment Panel III (2006) 기준으로 대사증후군과 정상군으로 구분 하였다. 다중로지스틱회귀분석을 시행하여 대장선종에 대한 대사증 후군의 교차비를 구하였다.결과:
공변량 보정후 남자는 대사증후군이 동반된 경우 대장선종의 교차비가 증가(odds ratio [OR], 1.54; 95% confidence interval [CI], 1.29- 2.65)하였으나, 여자에서는 유의한 차이가 없었다. 또한 남자에서는 공복혈당을 제외한 복부비만(OR, 1.39; 95% CI, 1.13-1.71), 중성지방 (OR, 1.83; 95% CI, 1.39-2.42), high density lipoprotein cholesterol (OR, 1.51; 95% CI, 1.15-1.98), 수축기혈압(OR, 1.55; 95% CI, 1.18-2.04) 등의 대 사증후군 요인이 동반된 경우 대장선종 교차비가 증가하였으나, 여 자는 유의성이 없었다. 남, 여 모두에서 연령이 증가할수록 대장선종 교차비가 증가하였다.결론:
대사증후군 및 대사증후군 요인들은 남자에 국한하여 독립적 인 대장선종의 위험요인으로 작용하였다.중심단어:
대장직장신생물; 대사증후군; 성별 차이REFERENCES
1. Borritz M, Rugulies R, Bjorner JB, Villadsen E, Mikkelsen OA, Kristensen TS. Burnout among employees in human service work: design and baseline findings of the PUMA study. Scand J Public Health 2006;34:49-58.
2. International Agency for Research Cancer. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012 [Internet].
Lyon: International Agency for Research Cancer; 2012 [cited 2012 Apr 1].
Available from: http://globocan.iarc.fr/factsheets/cancers/colorectal.asp.
3. Chan AT, Giovannucci EL. Primary prevention of colorectal cancer. Gastro- enterology 2010;138:2029-2043.e10.
4. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific State- ment. Circulation 2005;112:2735-52.
5. Fearnhead NS, Wilding JL, Bodmer WF. Genetics of colorectal cancer: he- reditary aspects and overview of colorectal tumorigenesis. Br Med Bull 2002;
64:27-43.
6. Chiu HM, Lin JT, Shun CT, Liang JT, Lee YC, Huang SP, et al. Association of metabolic syndrome with proximal and synchronous colorectal neoplasm.
Clin Gastroenterol Hepatol 2007;5:221-9.
7. Esposito K, Chiodini P, Colao A, Lenzi A, Giugliano D. Metabolic syndrome
and risk of cancer: a systematic review and meta-analysis. Diabetes Care 2012;35:2402-11.
8. Ahmed FE. Effect of diet, life style, and other environmental/chemopreven- tive factors on colorectal cancer development, and assessment of the risks. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev 2004;22:91-147.
9. Vargas AJ, Thompson PA. Diet and nutrient factors in colorectal cancer risk.
Nutr Clin Pract 2012;27:613-23.
10. Slattery ML, Potter JD, Curtin K, Edwards S, Ma KN, Anderson K, et al. Es- trogens reduce and withdrawal of estrogens increase risk of microsatellite in- stability-positive colon cancer. Cancer Res 2001;61:126-30.
11. Jinjuvadia R, Lohia P, Jinjuvadia C, Montoya S, Liangpunsakul S. The associ- ation between metabolic syndrome and colorectal neoplasm: systemic re- view and meta-analysis. J Clin Gastroenterol 2013;47:33-44.
12. Ju JH, Lim TK, Shin KK, Park KH, Park KC, Kim MJ, et al. Relationship be- tween the metabolic syndrome and colorectal polyps. J Korean Acad Fam Med 2007;28:134-40.
13. Kang HW, Kim D, Kim HJ, Kim CH, Kim YS, Park MJ, et al. Visceral obesity and insulin resistance as risk factors for colorectal adenoma: a cross-section- al, case-control study. Am J Gastroenterol 2010;105:178-87.
14. Kim JH, Lim YJ, Kim YH, Sung IK, Shim SG, Oh SO, et al. Is metabolic syn- drome a risk factor for colorectal adenoma? Cancer Epidemiol Biomarkers Prev 2007;16:1543-6.
15. Pyo JH, Kim ES, Chun HJ, Keum B, Jeen YT, Lee HS, et al. Fasting blood sug- ar and serum triglyceride as the risk factors of colorectal adenoma in korean population receiving screening colonoscopy. Clin Nutr Res 2013;2:34-41.
16. Johnson IT, Lund EK. Review article: nutrition, obesity and colorectal cancer.
Aliment Pharmacol Ther 2007;26:161-81.
17. Willett WC. Diet and cancer: an evolving picture. JAMA 2005;293:233-4.
18. Seow A, Yuan JM, Koh WP, Lee HP, Yu MC. Diabetes mellitus and risk of colorectal cancer in the Singapore Chinese Health Study. J Natl Cancer Inst 2006;98:135-8.
19. Ishino K, Mutoh M, Totsuka Y, Nakagama H. Metabolic syndrome: a novel high-risk state for colorectal cancer. Cancer Lett 2013;334:56-61.
20. Giovannucci E. Metabolic syndrome, hyperinsulinemia, and colon cancer: a review. Am J Clin Nutr 2007;86:s836-42.
21. Stefan N, Kantartzis K, Machann J, Schick F, Thamer C, Rittig K, et al. Identi- fication and characterization of metabolically benign obesity in humans.
Arch Intern Med 2008;168:1609-16.
22. Wang YY, Lin SY, Lai WA, Liu PH, Sheu WH. Association between adeno- mas of rectosigmoid colon and metabolic syndrome features in a Chinese population. J Gastroenterol Hepatol 2005;20:1410-5.
23. Park HY, Kim JR, Seo JY, Shin KS, Yoo BW, Cho YJ, et al. The association be- tween colon polyp and the metabolic syndrome in asymptomatic Korean adults. Korean J Health Promot 2013;13:87-92.
24. Kim BC, Shin A, Hong CW, Sohn DK, Han KS, Ryu KH, et al. Association of colorectal adenoma with components of metabolic syndrome. Cancer Causes Control 2012;23:727-35.
25. Erarslan E, Turkay C, Koktener A, Koca C, Uz B, Bavbek N. Association of visceral fat accumulation and adiponectin levels with colorectal neoplasia.
Dig Dis Sci 2009;54:862-8.
26. Yang MH, Rampal S, Sung J, Choi YH, Son HJ, Lee JH, et al. The association of serum lipids with colorectal adenomas. Am J Gastroenterol 2013;108:833-41.
27. Uzu T, Kimura G, Yamauchi A, Kanasaki M, Isshiki K, Araki S, et al. En-
도동희 외. 대장선종과 대사증후군의 관련성 Korean Journal of Family Practice
KJFP
hanced sodium sensitivity and disturbed circadian rhythm of blood pressure in essential hypertension. J Hypertens 2006;24:1627-32.
28. Nguyen SP, Bent S, Chen YH, Terdiman JP. Gender as a risk factor for ad- vanced neoplasia and colorectal cancer: a systematic review and meta-analy- sis. Clin Gastroenterol Hepatol 2009;7:676-81.e1-3.
29. Botteri E, Iodice S, Raimondi S, Maisonneuve P, Lowenfels AB. Cigarette smoking and adenomatous polyps: a meta-analysis. Gastroenterology 2008;134:388-95.
30. Atkin W, Kralj-Hans I, Wardle J, Duffy S. Colorectal cancer screening: ran- domised trials of flexible sigmoidoscopy. BMJ 2010;341:c4618.