대한외과학회지:제 74 권 제 6 호
□ 증 례 □
Vol. 74, No. 6, June, 2008
456
책임저자:채현동, 대구광역시 남구 대명4동 3056-6번지
705-718, 대구가톨릭대학교 의과대학 외과학교실 Tel: 053-650-4429, Fax: 053-624-7185
E-mail: [email protected]
접수일:2008년 1월 13일, 게재승인일:2008년 3월 12일 본 논문의 요지는 2006년 대한외과학회 추계학술대회에서 포스터 발표되었음.
중심 단어: 간세포암, 이소성 간조직, 파열된 이소성 간세포암
좌횡경막하 기원의 파열된 이소성 간세포암
대구가톨릭대학교 의과대학 외과학교실 채현동ㆍ박기호
Ruptured Ectopic Hepatocellular Carcinoma Aris- ing from the Left Subdiaphragm
Hyun-Dong Chae, M.D. and Ki-Ho Park, M.D.
Department of Surgery, School of Medicine, Daegu Catholic University, Daegu, Korea
Most hepatocellular carcinomas arise in orthotopic liver tis- sue as a result of chronic hepatitis B or C infection or cir- rhosis secondary to other chronic liver disease. There have been reports of ectopic liver tissue located in an extrahepatic organ such as the gallbladder, spleen, hepatoduodenal liga- ment and subdiaphragm. However, the incidence of hep- atocellular carcinoma originating from ectopic liver is very low. There have been 22 cases of ectopic HCCs (hepatocel- lular carcinoma) reported in the literature, and ruptured HCC has not yet been reported in the literature. As for the patho- genesis, the development of an ectopic HCC may be result of a compromised vascular supply or biliary drainage. We report here on a case of ruptured ectopic hepatocellular car- cinoma arising in the left subdiaphragm in a 76-year-old man who was treated with surgical resection. The patient was fol- lowed up for 1 year after surgery and he remained free of recurrence. Therefore, the unique localization and growth pattern of ruptured ectopic HCC may give the physician and patient the chance to achieve a curative resection. (J Korean Surg Soc 2008;74:456-458)
Key Words: Hepatocellular carcinoma, Ectopic liver tissue, Ruptured ectopic HCC
서 론
간세포암은 간세포에서 발생되는 암으로 일반적으로 정 상적으로 위치하는 간실질조직에서 발생하며 만성 B형이 나 C형 간염의 감염이나 다른 원인의 만성 간질환에 의한 간경변 이후 발생하는 암으로 알려져 있다. 이소성 간조직 이 간 외의 다른 조직인 담낭, 비장, 간십이지장인대, 횡경 막 하부에 존재하는 경우는 드물게 있으나,(1-6) 간세포암 이 간 외에서 발생하는 이소성 간세포암은 그 빈도가 매우 드물다. 또한 간혈관과 담관을 포함하며 연결된 부속 간에 서 발생하는 경성 간세포암(pedunculated HCC)과 달리 이소 성 간세포암은 주로 이소성 간조직에서 기원하여 발생하고 정상적인 위치에 존재하는 간의 간질환과 연관되지 않고 발생하므로 그 빈도가 더 드물다고 한다.(7) 더욱이 파열된 이소성 간세포암의 경우 국내에서는 보고된 바가 없을 정 도로 그 빈도가 더 드물어 저자들이 경험한 좌횡경막하 파 열된 이소성 간세포암의 치료경험을 문헌고찰과 함께 보고 하는 바이다.
증 례
평소에 건강하게 지내던 76세 남자 환자로 내원 당일 외 상의 병력 없이 갑자기 발생한 심와부 동통과 좌측 어깨 동통을 주소로 응급실로 내원하였다. 과거력에서 특별한 병력은 없었으며, B형이나 C형 간염의 병력 또한 없었다.
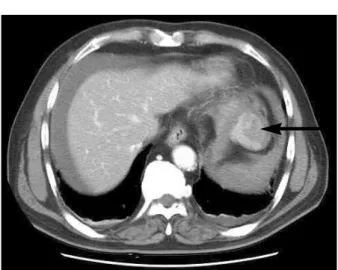
활력징후는 체온 섭씨 36.5도, 맥박 분당 110회, 호흡수 분 당 23회, 혈압 90/60 mmHg로 측정되었으며 이학적 검사에 서 전반적인 심한 복부팽만과 의식혼탁이 관찰되었고 혈액 검사에서 저혈색소수치를 보이며 응급실에서 촬영한 복부 단층촬영에서 4×5 cm 크기의 좌횡경막 종괴로부터 복강 내 출혈이 의심되어 응급개복수술을 시행하였다(Fig. 1).
개복소견에서 간의 경계와 표면은 정상이었고 복강 내에 는 다량의 혈액 및 혈종이 존재하였다. 복강 세척 후 관찰해 보니 좌횡경막하 종괴가 파열되어 있고, 출혈이 지속되고 있어 횡경막으로부터 분리하고 좌하부 횡경막하 동맥으로 추정되는 종양공급혈관을 Hem-o-lok ligating clipⓇ을 이용 하여 결찰 후 endo-GIAⓇ를 이용하여 일부 횡경막을 포함하 여 종괴를 절제한 후 더 이상의 출혈과 간종괴 및 복강 내
Hyun-Dong Chae and Ki-Ho Park:Ruptured Ectopic Hepatocellular Carcinoma Arising from the Left Subdiaphragm 457
Fig. 1. A contrast-enhanced helical CT scan of the abdomen at por- tal venous phase shows a large, lobulating, ruptured hetero- genous mass (arrow) with irregular contrast enhancement, measuring approximately 4×5 cm in the Left subdia- phragmatic space. There is no remarkable abnormality in the liver.
Fig. 2. Gross specimen consists of a well-demarcated, solid firm mass measureing approximately 4×5×4 cm with ruptured capsule at lower pole. There are linear stapling clip at re- secting surface from diaphragm and Hem-o-lok ligating clipⓇ at feeding vessel.
Fig. 3. Microscopic findings of the ruptured HCC. Magnified view of the tumor demonstrating moderately differentiated hep- atocellular carcinoma. Tumor cells with relatively abundant eosinophilic cytoplasms are arranged in thin or thick trabe- culae with conspicuous sinusoidal spaces between them.
The nuclei are enlarged and hyperchromatic. H&E stain,
×100.
다른 이상 소견은 관찰되지 않았다. 복강 세척 후 폐복하고 환자는 내원 9일째 별다른 합병증 없이 퇴원하였다. 절제된 종괴는 경계가 분명한 외막을 지니고 있었으나 일부 외막 이 파열되어 있었고, 병리학적 진단에서 이소성 간세포암 으로 진단되었다(Fig. 2, 3). 수술 1개월 후 외래 추적검사에 서 측정한 이중시기 나선식 전산화단층촬영과 간초음파 및 알파태아단백은 정상치로 측정되었고 6개월, 12개월에 외 래추적검사로 시행된 간초음파 및 알파태아단백 및 이중시 기 나선식 복부단층촬영에서 재발소견을 보이지 않았다.
고 찰
발생학적 이상에 의해 발생하는 비정상 위치에 존재하는 간조직은 발생빈도가 매우 드물고 주로 복강경이나 개복술 또는 부검 시에 우연히 발견되는데 복강경수술 시 0.7%정 도에서 발견된다고 한다.(8) 이러한 비정상 위치에 존재하 는 간조직은 크게 네 가지로 모간(mother liver)과 연결되어 있지 않은 이소성 간(ectopic liver), 담낭 벽에서 발견되는 현미경적 이소성 간(microscopic ectopic liver), 모간과 경 (stalk)으로 연결되고 붙어있는 큰 부속간(large accessory liv- er, pedunculated liver)과 경(stalk) 없이 모간과 붙어있는 10
∼30 g 무게의 작은 부속간(small accessory lover)으로 분류 하기도 하고,(4) 비정상 위치의 간세포를 간조직의 발생학 적 이동의 장애로 인해 발생하는 이소성 간(ectopic liver)과 하나 이상의 간성삭(hepatic cord)의 비대로 인해 발생하는 경성간(pedunculated liver)으로 나누어 분류하기도 한다.(9) 저자들이 경험한 비정상 위치에 존재하는 간세포암은 이소 성 간조직에서 발생한 간세포암으로 분류될 수 있다. 이소 성 간세포암은 1965년에서 1999년까지 전세계적으로 22예 정도만이 보고된 매우 드문 질환이고 파열되어 복강 내 출 혈의 임상적 증상이 나타난 이소성 간세포암은 아직까지 보고된 바가 없다.(10)
정위간(orthotopic liver)에서 발생하는 간세포암은 80%
정도에서 B형, 또는 C형 간염바이러스감염과 관련이 있으 며 간경변증을 동반한 경우는 69.3∼81.3% 정도로 보고된 다.(11,12) 이와 달리 이소성 간세포암은 모간의 바이러스성
458 J Korean Surg Soc. Vol. 74, No. 6
간염이나 간경변과 관련 없이 이소성 간조직의 담즙배출과 혈행공급장애에 의해 발생한다고 하고,(9) 모간의 간경화와 동반된 경우는 단지 22명 중 7명(31%)에서만 발생하였다고 하여 이소성 간세포암의 발생기전은 정위간에서 발생하는 간세포암과 그 발생기전에 있어 다르다고 한다.(10) 저자들 이 경험한 이소성 간세포암에 있어서 모간의 바이러스성 간염이나 간경변 등의 간질환의 과거력 없이 이소성 간조 직이 간세포암으로 진행되고 파열되어 복강 내 출혈이 발 생한 것으로 생각되며 이를 통해 볼 때 이소성 간세포암은 정상위치에 존재하는 간세포암과는 다르게 이소성 간조직 의 담즙배출과 혈행공급장애에 의해 이소성 간조직에서 간 세포암이 발생한다고 생각한다.
일반적으로 정위간에서 발생하는 파열된 간세포암의 경 우 수술 전 진단율이 25% 정도로 매우 낮고,(13) 발생 당시 간 기능이 좋지 않고 간경변 등의 기존 간질환에 의해 간 기능이 좋지 않고 혈복강에 의한 혈류동태의 불안정성 때 문에 수술사망률이 16.5%로 매우 높다고 하며,(14) 재발률 또한 높아 3년 생존율 및 5년 생존율이 40.5%, 26.5%로 매 우 낮다고 한다.(15) 이와 달리 이소성 간세포암은 완전절 제만으로 그 치료성적이 우수한데 이는 종양 발생의 가능 성이 이소성 간조직에 국한되어 있어 이를 수술적 치료로 제거하는 것만으로 완전치유가 가능하기 때문이라고 한 다.(16) 저자들이 경험한 이소성 간세포암도 수술 후 1년간 의 추적검사에서 재발이나 AFP의 증가가 없는 것으로 보아 정상으로 위치하는 간 실질 조직의 기존 간질환 없이 발생 하고 단독으로 위치하는 해부학적 특성 때문에 수술적 절 제만으로도 치료성적이 우수한 것으로 생각한다.
저자들이 경험한 이소성 간세포암은 발생 빈도가 낮고 더욱이 파열된 이소성 간세포암의 경우는 그 빈도가 더 드 물어 저자들이 경험한 좌횡경막하 파열된 이소성 간세포암 의 치료경험을 문헌고찰과 함께 보고하는 바이다.
REFERENCES
1) Bassis ML, Izenstark JL. Ectopic liver; its occurrence in the gallbladder. AMA Arch Surg 1956;73:204-6.
2) Lieberman MK. Cirrhosis in ectopic liver tissue. Arch Pathol
1966;82:443-6.
3) Heid GJ Jr, von Haam E. Hepatic heterotopy in the splenic capsule. Arch Pathol 1948;46:377-9.
4) Collan Y, Hakkiluoto A, Hastbacka J. Ectopic liver. Ann Chir Gynaecol 1978;67:27-9.
5) Jimenez AR, Hayward RH. Ectopic liver; a case of esophageal obstruction. Ann Thorac Surg 1971;12:300-4.
6) Sehdeva JS, Logan WD Jr. Heterotopic (supradiaphragmatic) liver. Ann Thorac Surg 1971;11:468-71.
7) Takayasu K, Itabashi M, Moriyama N. Case report: ectopic hepatocellular carcinoma arising from the left diaphragm. Clin Radiol 1994;49:579-81.
8) Sato S, Watanabe M, Nagasawa S, Niigaki M, Sakai S, Akagi S. Laparoscopic observations of congenital anomalies of the liver. Gastrointest Endosc 1998;47:136-40.
9) Christine PJ, Caygill CP, Gatenby PA. Ectopic liver and hepa- tocarcinogenesis. Eur J Gastroenterol Hepatol 2004;16:727-9.
10) Arakawa M, Kimura Y, Sakata K, Kubo Y, Fukushima T, Okuda K. Propensity of ectopic liver to hepatocarcinogenesis:
case reports and a review of the literature. Hepatology 1999;
29:57-61.
11) Song HS, Chae KM, Kim HC. A clinical analysis of primary hepatocellular carcinoma. Korean J Gastroenterol 1994;26:521- 8.
12) Bae TS, Kim SB, Park SH, Choi DW. Outcome of hepatic resection for hepatocellular patients. J Korean Surg Soc 2003;64:480-6.
13) Vivarelli M, Cavallari A, Bellusci R, De Raffele E, Nardo B, Gozzetti G. Ruptured hepatocellular carcinoma: an important cause of spontaneous haemoperitoneum in Italy. Eur J Surg 1995;161:881-6.
14) Vergara V, Muratore A, Bouzari H, Polastri R, Ferrero A, Galatola G, et al. Spontaneous rupture of hepatocelluar carci- noma: surgical resection and long-term survival. Eur J Sur Oncol 2000;26:770-2.
15) Chen M, Hwang T, Jeng L, Wang C. Clinical experience with hepatic resection for ruptured hepatocellular carcinoma. Hepa- togastroenterology 1995;42:166-8.
16) Leone L, Paolis P, Carrera M, Carucci P, Musso A, David E, et al. Ectopic liver and hepatocarcinogenesis: report of three cases with four years' follow-up. Eur J Gastroenterol Hepatol 2004;16:731-5.