예각기시(Acute Angle Takeoff)로 인한 독립된 좌주관상동맥 개구부협착 1예
5
0
0
전체 글
(2) 하였다.. 증. 례. 가족력 및 기타과거력:특이사항 없음. 이학적 소견:입원당시 혈압은 130/70 mmHg, 맥. 환 자:최○선, 여자, 34세.. 박은 분당 70회, 호흡수는 분당 22회, 체온은 36.5℃. 주 소:보행시 전흉부통.. 였다. 전경부에 미만성의 갑상선종대가 촉진되었다. 경. 현병력:환자는 평소 심계항진과 발한 증세 있었으. 정맥 울혈증세는 없었으며 흉부청진상에서 수포음이나. 며 내원 1주전에 보행시에 양어깨로 방사되는 6분 정. 심잡음은 청진되지 않았다. 복부는 촉진상 간과 비장종. 도의 날카로운 흉통을 주소로 본원 순환기내과에 입원. 대 소견 없었고 하지부종도 없었다. 검사실 소견:입원 당시 시행한 말초혈액 검사상 백 혈구 5,220/mm3, 혈색소 12.9 g/dL, 헤마토크리트 42%, 혈소판 221,000/mm3였다. 생화학적 검사상 BUN 16 mg/dL, Creatinine 0.7 mg/dL, 공복시 혈당 80 mg/dL, Total-Protein 6.6 g/dL, Albumin 4.2 g/dL, AST/ALT 18/20 IU/L, Total-Bilirubin 0.7 mg/dL, Na 140 mEq/L, K 3.8 mEq/L, Total-Cholesterol 158 mg/dL, HDL-Cholesterol 34 mg/dL, Triglyceride 169 mg/dL, LDL-Cholesterol 90.2 mg/dL였 다. 면역 혈청학적 검사에서 CRP 0.01 ng/dL, ESR 20 mm/hr, Homocystein 5.26 μmol/L, F-ANA 음성, RA factor 음성, VDRL 음성, TPHA 음성이었다. PT 와 aPTT는 정상소견 이었다. 갑상선기능검사상 TSH 0.00 mU/L, Free T4 3.19 ng/dL, Total T3 2.12. Fig. 1. Coronary angiography shows an left main coronary ostial stenosis.. A. ng/mL, Thyroglobulin Ab 양성(0.4 U/mL), AntiMicrosome Ab 양성(26.3 U/mL), TSH-Receptor. B. Fig. 2. A:Two-dimensional echocardiogram shows an ostial stenosis and acute angle takeoff of the left main coronary artery. B:Diagram of coronary arteries shows an acute angle takeoff of the left main coronary artery and posteriorly located ostium. The ostium of left main coronary artery is narrowed by atherosclerosis. AO: aorta, L:left sinus of Valsalva, LA:left atrium, LAD:left anterior descending coronary artery, LC:left circumflex coronary artery, R:right sinus of Valsalva, RV:right atrium, RC:right coronary artery.. 443.
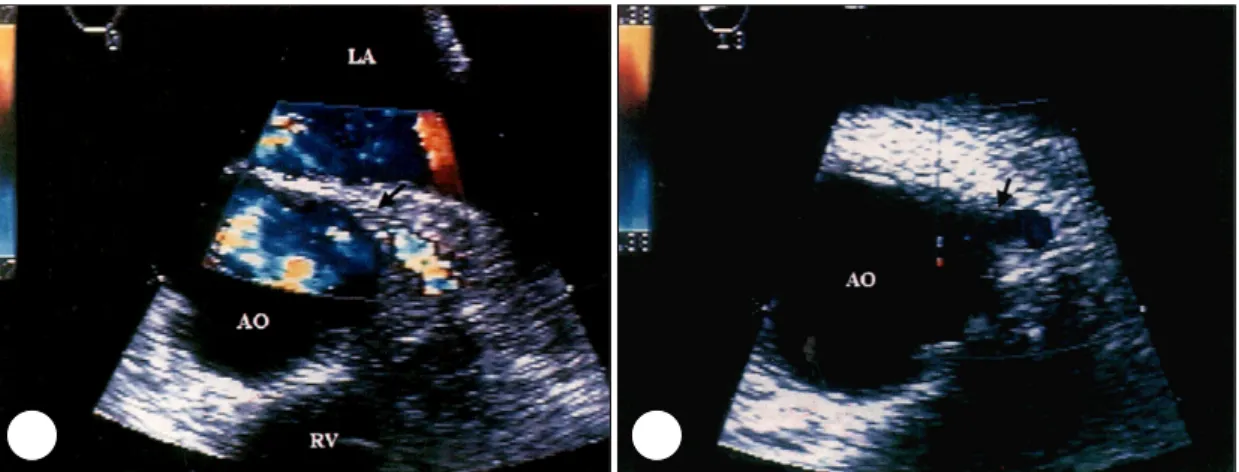
(3) 근하여 좌주관상동맥의 협착부위 이상까지 절개한 후. Ab 19%였다. 심전도 소견:내원 당시 검사한 심전도에서 ST 분절 의 상승이나 Q파는 없었다. 흉부 방사선 소견:특이 소견은 관찰되지 않았다. 심초음파 소견:좌심실의 수축시 내경은 23 mm, 이 완기 내경은 43 mm이었으며 심박 구출율은 정상이었. 신선한 자가 심낭편을 첨포로 이용하여 혈관성형술을 시행하였다. 수술직후 확장된 좌주관상동맥의 개구부를 경식도심초음파로 확인하였다(Fig. 3A and B). 현재 환자는 보행시나 운동시에 흉통 호소 없으며 건 강한 상태로 외래추적관찰중이다.. 다. 다른 특이소견은 없었다.. 고. 관상동맥조영술 소견:좌주관상동맥 입구만 70~80%. 찰. 정도의 협착된 소견을 보였으며 우관상동맥과 좌회선관 상동맥은 정상이었다(Fig. 1).. 임상적으로 중증의 좌주관상동맥 개구부협착이 있는. 경식도 심초음파 소견:좌주관상동맥의 기시부가 정. 경우 적어도 세 개의 관상동맥중 둘 이상은 동맥경화로. 상보다 뒤쪽에서 개구하며 대동맥동과의 45°이하의 각. 인하여 심하게 협착된 소견을 보이는데 본 증례와 같은. 도를 이루며 기시하고 있었다(Fig. 2A and B).. 독립된 좌주관상동맥 개구부협착증은 매우 드문 질환. 갑상선 초음파검사:협부와 양엽이 미만성으로 종대 되어 있었다.. 이다. Charles등10)은 1969년에서 1973년까지 3000 명에서 관상동맥조영술을 시행하여 관상동맥개구부에. 갑상선 스캔:갑상선 양엽의 전반적 종대와 섭취가 증가되어 있었고 내부에 냉결절등은 관찰되지 않았다.. 협착이 있는 4명(0.13%)의 환자를 경험했으며 Thompson등11)과 Graham등12)은 각각 2105명과 4000 명의 관상동맥조영술을 검사하여 27명과 35명의 관상. 치료 및 경과. 동맥개구부 협착증환자를 발견하였고 양쪽 모두 5명 (0.2%, 0.12%)의 환자에서 다른 관상동맥에는 병변이. 입원 후 환자는 협심증에 대한 약물치료를 시행하였. 없는 독립된 관상동맥개구부 협착증이 있었다고 보고. 으며 갑상선 기능항진증에 대하여 Propylthiouracil 300. 했다. 한가지 특이한 점은 이 14명의 환자는 대부분 폐. mg을 하루 3회 3주동안 투여하였다. 수술전 시행한 경. 경전의 여성이었다는 점이다. 하지만 이 이유에 대해서. 식도심초음파검사상 좌주관상동맥이 정상보다 뒤쪽에서. 는 아직 확실히 밝혀진 바 없다. 독립된 좌주관상동맥. 기시되면서 대동맥 벽과 45도 이하의 각을 이루고 있. 개구부협착이 있는 환자군과 개구부협착 뿐만아니라 그. 었다.. 외의 혈관에도 병변이 같이 있는 환자군을 비교해 보았. 흉부외과에서 대동맥을 횡으로 절단 후 후방에서 접. A. 을 때 독립으로 있는 환자군에서는 보다 최근에 처음으. B. Fig. 3. Two-dimensional color flow Doppler images of short axis view through the aortic valve. A:Color flow Doppler image shows an acceleration signal (arrow) at the site of stenosis and poststenotic segment. B:After surgical enlargement of the left main coronary ostium. Note the disappearance of the acceleration signal. AO:aorta, LA:left atrium, RV:right atrium.. 444. Korean Circulation J 2001;31(4):442-446.
(4) 로 흉통을 경험했으며 대부분에서 조직을 얻기 어려워. 이 새로 생기거나 악화되는 경우가 있어 주의가 요구된. 조직검사는 시행하지 않았지만 수술시 육안적으로 동. 다.13) 최근에는 혈관성형술이외에도 stent를 이용한 확. 맥경화성 변화를 보인 반면 동맥경화증의 위험인자는. 장술이 이러한 좌주관상동맥개구부 협착증에 시도되고. 적어 이들에게 동맥경화를 유발하는 다른 요인이 있을. 있다.19) 그러나 독립된 좌주관상동맥 개구부협착증은. 것으로 추정된다.11). 대동맥질환과 연관이 많으며 형태학적인 문제로 인하. 1990년부터 1998년까지 세종병원에서 5611명의 진. 여 기인할 수도 있다고 볼 때 stent를 이용한 확장술이. 단적 관상동맥조영술중 24명(0.43%)이 독립된 좌주. 나 관상동맥 우회술보다는 혈관성형술이 더 좋을 것으. 관상동맥 개구부협착증으로 진단받았으며 이중 20명이. 로 생각되어진다.. 여자였고 동맥경화 위험인자가 없는 경우가 11예였다. 22예에서는 동맥경화증에 의한 것이었고 1예는 Takayasus 동맥염, 1예는 원인은 알 수 없었지만 병리조. 중심 단어:독립된 좌주관상동맥 개구부협착증・관상동 맥 예각기시.. 직소견으로 fibromyxoid를 보였다.13). REFERENCES. 본 증례에서 관찰된 관상동맥의 예각기시(acute angle. 1) Shah DC, Subramanyan K. Clinically isolated left co-. takeoff)는 관상동맥 개구부가 대동맥동과 45°이하의. ronary ostial stenosis: A manifestation of cardiovascular syphiliscase history. Angiology 1993;44:919-21. [No Authors]. Case records of the Massachusetts general hospital. Weekly clinicopathological exercise. Case 10-1998. A 46-year-old man with chest pain and coronary ostial stenosis. N Engl J Med 1998;338:897-903. Amano J, Suzuki A. Coronary artery involvement in Takayasus arteritis. J Thorac Cardiovasc Surg 1991;102: 554-60. Allen JM, Thompson GR, Myant NB, Steiner R, Oakley CM. Cardiovascular complications of homozygous familial hypercholesterolaemia. Br Heart J 1980;44:361-8. Codecasa R, Scioti G, Baglini R, Pratali S, Milano A, Bortolotti U. Concomitant aortic valve replacement and surgical angioplasty of left main coronary ostium. Thorac Cardiov Surg 2000;48:105-7. Firstenberg MS, Greenberg NL, Lin SS, Garcia MJ, Alexander LA, Thomas JD. Transesophageal echocardiography assessment of severe ostial left main coronary stenosis. J Am Soc Echocardiogr 2000;13:696-8. Kalangos A. Left coronary ostial stenosis caused by focal intimal fibrosis. Ann Intern Med 1999;131:717. Menke DM, Jordan MD, Aust CH, Waller BF. Isolated and severe left main coronary atherosclerosis and thrombosis: A complication of acute angle takeoff of the left main coronary artery. Am Heart J 1986;112:1319-20. Virmani R, Chun PK, Goldstein RE, Robinowitz M, McAllister HA. Acute takeoffs of the coronary arteries along the aortic wall and congenital coronary ostial valvelike ridges. Association with sudden death. J Am Coll Cardiol 1984;3:766-71. Pritchard CL, Mudd JG, Barner HB. Coronary ostial stenosis. Circulation 1975;52:46-8. Thompson R. Isolated coronary ostial stenosis in women. J Am Coll Cardiol 1986;7:997-1003. Miller GA, Honey M, El-Sayed H. Isolated coronary ostial stenosis. Cathet Cardiovasc Diagn 1986;12:30-4. Moon KS, Kim YJ, Kim JS, Hong SK, Hwang HK. Outcome of surgical angioplasty for isolated coronary ostial stenosis. Circulation 1999;29:46-54. Hitchcock JF, Robles de Medina EO, Jambroes G. An-. 각도를 이루며 기시하고 있을 때를 말하며 이는 선천적 인 개구부의 기형으로 Virmani등9)은 평소 심혈관 질환. 2). 의 기왕력이 없었던 22명의 급사환자들을 대상으로 부 검을 실시한 결과 이중 13명(59%)이 관상동맥 개구부. 3). 의 예각기시(acute angle takeoff)소견을 보였고 이러 한 형태학적인 문제가 관상동맥 근위부에 비정상적인. 4). 혈류양상을 일으킴으로써 내막에 손상을 주어 조기 동 맥경화를 촉진하고 또한 대동맥궁의 확장에 의해 쉽게. 5). 압박받아 급격한 혈류장애를 가져와 사망의 한 원인이 되었을 것이라고 보고하고 있다. David등8)은 44세의 여자환자에서 좌주관상동맥의 예각기시(acute angle. 6). takeoff)에 기인한 급성심근경색증으로 사망한 예를 보 고하였으며 이 환자에서도 다른 관상동맥에는 동맥경화 변화가 없었으나 개구부에만 심한 동맥경화판이 있었 다. 본 저자들의 예에서는 수술시 육안적으로 좌주관상. 7) 8). 동맥이 정상보다 뒤쪽에서 예각기시하면서 동맥경화성 비후와 석회화가 관찰되었고 완전한 조직을 얻지는 못. 9). 하였으나 조직검사상 초기 동맥경화로 의심되는 소견 을 보였다. 과거에는 이러한 좌주관상동맥 개구부의 협착증은 우 회로 조성수술이 일반적으로 시행되었지만 우회로가 다 시 막히는 등의 여러 문제가 보고되다가 1983년도에 14). Hitchcock등 에 의해 첨포를 이용한 혈관성형술이 보 편화되기 시작하여 국내외에서도 여러 좋은 결과들이 보고되고 있다.15-18) 본원에서도 현재까지 40예에서 혈 관성형술을 시행하여 좋은 결과를 얻은 경험이 있지만 혈관성형술을 시행한 환자에서 대동맥판막 폐쇄부전증. 10) 11) 12) 13) 14). 445.
(5) gioplasty of the left main coronary artery for isolate left main coronary artery disease. J Thorac Cardiovasc Surg 1983;85:880-4. 15) Yoon CS, Yoo KJ, Lee KJ, Kim DJ, Kang MS. The clinical experiences of patch angioplasty in isolated critical left main coronary artery stenosis. Korean Thora & Cardiovase Surg 1998;31:674-8. 16) Bortolotti U, Milano A, Balbarini A, Tartatini G, Levantino M, Borzoni G, et al. Surgical angioplasty for isolated coronary ostial stenosis. Tex Heart Inst J 1997; 24:366-71.. 446. 17) Dion R, Elias B, Khoury G, Noirhomme P, Verhelst R, Hanet C. Surgical angioplasty of the left main coronary artery. Eur J Cardiothorac Surg 1997;11:857-64. 18) Bonacchi M, Prifti E, Giunti G, Leacche M, Ballo E, Furci B, et al. Mid-Term outcome of surgical coronary ostial plasty: our experience. J Card Surg 1999;14:294-300. 19) Park SJ, Lee CW, Hong MK, Kim JJ, Park SW. Stent placement for ostial left anterior descending coronary artery stenosis: acute and long-term (2-year ) results. Catheter Cardiovasc Interv 2000;49:267-71.. Korean Circulation J 2001;31(4):442-446.
(6)
수치

관련 문서
We report a case of complete thrombotic occlusion of an unprotected left main coronary artery in acute myocardial infartion and cardiogenic shock treated successfully
Acute left main coronary artery thrombosis as an initial presentation of systemic lupus erythematosus.. Kang Un
Therefore, intravascular imaging, especially IVUS, should be considered for patients with focal lesions in the proximal LAD or left main coronary artery, in whom severe vasospasm
(C, D) At 1 month after cataract surgery and 7 months after nonarteritic anterior ischemic optic neuropathy following acute angle‐closure crisis, left eye showed the optic disc
A:an entrapped and fractured cutting balloon black arrow impacted in the left main and proximal left anterior descending coronary artery and distal end of detached balloon
Disc photographs and printout of optical coherence tomog- raphy (OCT) taken at the time of left acute primary angle closure show a hyperemic and slightly edematous left optic
This study demonstrates that in the proximal and mid segments of all 3 major arteries and the left main trunk, CTCA has a high accuracy in excluding coronary artery disease
