The incidence of deep venous thrombosis (DVT) is highly dependent on the population studied and on the definition of DVT used. Moreover, in Korea, the prevalence of DVT is increasing (Table 1). The true incidence of this disease as quoted by previous epidemiological studies are generally underestimated because study populations have been restricted to those who present at hospitals and are then diagnosed as having DVT. Furthermore, one autopsy study concluded that up to 50% of venous thromboembolisms is overlooked ante mortem.1
Two main complications of DVT are pulmonary embolism and post-thrombotic syndrome (PTS), and the incidence of PTS is higher in patients that only receive anticoagulation for the management of DVT.2Most physicians consider that the delivery of a thrombolytic agent into a thrombus is more effective than systemic anticoagulation because this procedure reduces the complication rate of systemic anticoagulation.1,2 Contemporary venous thrombectomy has been reported to
Catheter-Directed Thrombolysis
with Conventional Aspiration Thrombectomy for Lower Extremity Deep Vein Thrombosis
Yong Sun Jeon,
2Yong Han Yoon,
1Joung Ym Cho,
1Wan Ki Baek,
1Kwang Ho Kim,
1Kee Chun Hong,
3and Joung Taek Kim
1Departments of 1Thoracic and Cardiovascular Surgery, 2Radiology, and 3General Surgery, Inha University Hospital, Incheon, Korea.
Purpose:The purpose of this study is to evaluate treatment outcomes in patients with symptomatic deep vein thrombosis (DVT) who had undergone a catheter-directed thrombolysis with conventional aspiration thrombectomy for the treatment of lower extremity deep vein thrombosis. Materials and Methods:The authors retrospectively reviewed the records of 74 patients (mean age 61 ± 15) that underwent a catheter-directed thrombolysis with conventional aspiration thrombectomy. A retrieval inferior vena cava (IVC) filter was placed to protect against a pulmonary embolism in 60 patients (81%). Stenting and balloon angioplasty were performed in 37 patients (50%) under the left common iliac vein compression. Results:Sixty-seven patients (91%) showed a clinical improvement within 48 hours, but seven patients (9%) showed no improvement. Multi detector computerized tomographic venography (MDCT venography) at discharge showed no thrombus in 15 patients (20%) and partial thrombus in 52 (70%). Twenty-eight patients (38%) developed post-thrombotic syndrome at 3.0 ± 4.2 months postoperatively. Six patients (8%) were admitted due to DVT recurrence at a mean of 5.6 ± 7.4 months postoperatively. Sixty-nine patients underwent follow up MDCT venography at 5.7 ± 5.6 months. fifty (72%) of these showed no thrombus, 15 (22%) partial thrombus, and 4 (6%) showed obstruction. Twentyeight of 61 (46%) were asymptomatic, twentyeight (46%) had moderate improvement, and four (6%) were mildly improved by a telephone interview (81%) at 22.8 ± 10.7 months postoperatively. Conclusion:Catheter-directed thrombolysis with conventional aspiration thrombec- tomy is an effective treatment for lower extremity deep vein thrombosis and produces satisfactory clinical results.
Key Words : Thrombolysis, thrombectomy, deep vein thrombosis, catheter
Received: March 3, 2009 Revised: May 26, 2009 Accepted: July 7, 2009
Corresponding author: Dr. Joung Taek Kim, Department of Thoracic and Cardiovascular Surgery, Inha University Hospital, 7-206 Sinheung-dong 3-ga, Jung-gu, Incheon 400-711, Korea.
Tel: 82-32-890-2280, Fax: 82-32-890-3099 E-mail: [email protected]
∙The authors have no financial conflicts of interest.
© Copyright:
Yonsei University College of Medicine 2010
INTRODUCTION
improve early and long term results in extensive iliofemoral DVT as compared with simple catheter-directed throm- bolysis.3,4Furthermore, several percutaneous thrombectomy devices have been recently released,4,5and replaced conven- tional thrombectomy. The aim of this study is to evaluate the clinical efficacy of catheter-directed thrombolysis with conventional aspiration thrombectomy for the treatment of lower extremity deep vein thrombosis, and to document clinical outcomes.
The hospital records of 74 patients diagnosed with sympto- matic DVT from October 2004 to December 2007 were analyzed retrospectively. The male/female ratio was 34/40, and mean patient age was 60 ± 15 years. Sixty-eight patients (92%) complained of leg swelling, and 40 patients (54%) of leg pain. Mean symptom duration of the patients was 8.4 ± 12.1 days, with a median of 4 days and a range of 1 to 60 days. Patient characteristics are summarized in Table 2. Risk factors for hypercoagulability are listed in Table 3.
Diagnoses were established by color duplex ultrasound imaging or MDCT venography or venography, which was performed in an angiography suite. We performed MDCT pulmonary angiography to detect for a pulmonary embolism in all patients.
All patients underwent aspiration thrombectomy first and then a catheter-directed thrombolysis. A prophylactic retrievable IVC filter (OptEase, Cordis, Miami, FL, USA) was inserted in 15 patients with a free floating thrombus into the IVC or common iliac vein, in 10 patients diag- nosed with pulmonary embolism at admission, or in 35 patients with both. For venous access, a patient was placed in a prone position and the ipsilateral popliteal vein was accessed using a micropuncture needle kit (Micropuncture introducer set, Cook, Bloomington, IN, USA) under ultrasound guidance (Logiq P5 premium, GE, Seongnam, Korea). After an initial ascending venogram had been obtained using a 9 F introducer sheath (Radifocus intro- ducer II, Terumo, Leuven, Belgium), direct aspirations of the embolus were performed several times using an 8F guiding catheter (Vistabrite tip, Cordis, Miami, FL, USA) while maintaining negative pressure with a 50 mL syringe.
Stent placement was indicated if the left common iliac vein
was compressed after embolus aspiration. Stents were placed over a guide wire into the left common iliac vein and were typically between 10 to 14 mm in diameter and 60 to 90 mm long (Wallstent, Boston Scientific, Galway, Ireland). Stent dilatation was achieved using a balloon catheter (BlueMax 20, Boston Scientific, Galway, Ireland).
After the thrombectomy with or without stent placement, thrombolysis was performed by placing a 20 cm multi-side hole thrombolysis catheter (Multisideport catheter infusion set, Cook, Bloomington, IN, USA) into the thrombosed vein. The procedure started by infusing urokinase (GCC- Urokinase, Green Cross, Yongin, Korea) at a rate of 80,000 to 120,000 IU/hour; the rate used depended on the patient’s
MATERIALS AND METHODS
Table 1. Incidences of New or Recurring DVT in Korea
Year 2003 2004 2005 2006 2007
No. of patients* 35 37 40 42 51
DVT, deep vein thrombosis.
Data was provided by the Korean Health Insurance Review & Assessment Service.
*per 100,000 of the population.
Table 2. Patient Characteristics (n = 74)
Age (mean ± SD, yr) 61 ± 15
Gender (male) 34 (46%)
Symptoms
Leg swelling 68 (92%)
Leg pain 40 (54%)
Duration (mean ± SD) 8.4 ± 12.1 (days) Pulmonary embolism at admission 45 (61%) Predisposing factors
May-Thurner syndrome 34 (46%)
Immobilization 23 (37%)
Hypercoagulability 18 (29%)
Previous operation 12 (19%)
Obesity 7 (11%)
Previous DVT 7 (11%)
Malignancy 2 (3%)
Location of thrombus
Left limb 59 (80%)
Suprainguinal 57 (77%)
SD, standard deviation; DVT, deep vein thrombosis.
Table 3. Primary Hypercoagulable States (n = 18, 24%)
Protein C deficiency 5 (28%)
Protein S deficiency 4 (22%)
Homocystein abnormality 4 (22%)
Factor V deficiency 2 (11%)
Betchet’s disease 2 (11%)
Polyarteritis nodosa 1 (6%)
condition, amount of thrombus, and the patient’s weight.
Venography was carried out 12 hour later to evaluate the progress of thrombolysis and to correct the catheter position.
Infusion was continued for a further 24 hours if the thro- mbus had not completely resolved. Anticoagulation was carried out after thrombolysis by continuously infusing heparin to a partial thromboplastin time of 70-90 seconds, which was subsequently checked at 6-hour intervals. The subsequent treatment protocol included oral anticoa- gulation with warfarin to a target international normalized ratio of 2.0-2.5 for 3 months. The retrieval IVC filter was removed at 2 weeks postoperatively from 46 (76%) patients with optimal patency by MDCT venography. It was left behind for permanent use in 14 (24%) patients with suboptimal patency by MDCT venography.
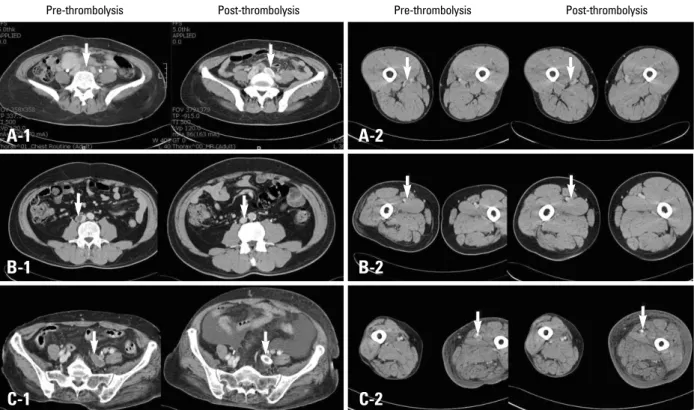
Thrombus removal was defined as complete if the MDCT venogram at discharge showed no evidence of a residual clot (Fig. 1A), and partial thrombus removal was defined if any residual clot was visualized (Fig. 1B). Treatment failure was defined as near total obstruction of the venous lumen by thrombus (Fig. 1C). Follow-up examinations were performed at 6 months postoperatively by MDCT venography. In addition, a telephone interview was con- ducted with each patient during September 2008 by a trained nurse to determine the clinical outcome and clinical symptoms; outcomes were defined as asymptomatic, moderately improved, mildly improved, unchanged,
mildly worsened, moderately worsened, and considerably worsened.
Thrombosis was located on the left side in 58 (78%) patients and on the right side in 16 (22%) patients. The IVC was affected in 6 (8%) patients. Thrombosis was involved up to the supra inguinal segments in 57 (77%) patients, and up to the infra inguinal segments in 17 (23%) patients. Pulmonary embolism was diagnosed in 45 (61%) patients. Clinical improvement, as defined by a decrease in pain and/or swell- ing of the affected extremity within 48 hours of intervention, was displayed by 67 (91%) patients. Primary stent place- ment for segmental stenosis was necessary in 37 (50%) patients. The mean urokinase infusion time was 31 (8-48) hours, and the mean amount of urokinase delivered was 2,630,000 ± 1,083,000 units. Complete thrombus removal was achieved in 15 (20%) patients, and partial thrombus removal in 52 (70%) by MDCT venography at discharge.
Treatment failure occurred in 7 (9%) patients (Table 4).
Four (5%) bleeding complications related to thrombolysis occurred. However, only one patient had a major bleeding complication and retroperitoneal hematoma, and required a blood transfusion. DVT recurrence was diagnosed with a Doppler study and MDCT venography in 6 (8%) patients.
RESULTS
Fig. 1. MDCT angiograms showing complete thrombus removal (A), partial thrombus removal (B), and treatment failure (C). Each A-1, B-1, C-1 are in an axial view before thrombolysis at the level above the iliac vein (arrow), and A-2, B-2, C-2 are in an axial view after thrombolysis at the level of the superficial femoral vein (arrow). MDCT, multi detector computerized tomographic.
Pre-thrombolysis Post-thrombolysis Pre-thrombolysis Post-thrombolysis
A-1 A-2
B-1 B-2
C-1 C-2
These patients were readmitted for further treatment. Post- thrombotic syndrome, defined as affected limb edema, pigmentation, pain, and/or venous insufficiency by a Doppler study, was noted in 28 (38%) patients at 3.0 ± 4.2 months postoperatively. MDCT venography showed complete thrombus removal in 50 (72%) patients, partial removal in 15 (22%), and treatment failure in 4 (6%) during the 5.7 ± 5.6 month follow-up (Table 4). The mean clinical follow-up interval was 22.8 ± 10.7 months, and 61 patients among the 74 patients were accessed via a tele- phone interview (81%). Twenty-eight of the 61 (46%) tele- phone patients were asymptomatic, twenty-eight (46%) had moderate improvement, and four (6%) were mildly improved.
Epidemiologic studies have shown that DVT is highly pre- valent in western populations. The incidence of venogra- phically confirmed DVT in Sweden has been reported to be as high as 160 cases of new or recurring DVT per 100,000 of the population per year,6and 116,000 to more than 250,000 new cases of clinically recognized DVT per year are recorded in the United States.7The Korean Health Insurance Review & Assessment Service reported that in 2007, 51 per 100,000 of the population were treated for new or recurring DVT, and that the incidence of this disease is increasing (Table 1). The causes of this increase are multi- factorial, but the main reason is likely to be a Westernization of diet resulting from economical development in the past 20 years. The number of May-Thurner syndrome patients was 34 (46%), which was higher than that reported pre- viously.5There is a reason why the left limb was more
frequently involved (80% vs. 20%) in our population.
Patients with anatomical compression of the left common iliac vein by the left common iliac artery are prone to develop venous flow stasis in the left leg. Husmann, et al.8 reported that combined thrombolysis and stenting of a common iliac vein obstruction is effective. Our results showed a good 6 months MDCT venography follow-up in patients with stent placement. The incidence of hypercoa- gulable disorder was 29%, which is lower than the 78%
previously reported.9Differences between the above-men- tioned predisposing risk factors may be due to racial differences.
Numerous studies have reported positive outcomes for catheter-directed thrombolysis in acute DVT.1-3,5Mewissen, et al.10documented a complete resolution rate of 31%, a partial rate of 52%, and a failure rate of 17%, whereas Verhaeghe, et al.11 reported a complete resolution rate of 79% and a failure rate of 21%. In the present study, the complete resolution rate was 20%, the partial resolution rate was 70%, and the failure rate was 10%. Our immediate complete resolution rate was lower than those of these other reports. The duration of symptoms at the onset of lytic therapy was predictive of lytic outcome.10 For acute cases (less than 10 days), the prevalence of complete lysis was 34% compared with 19% in cases with a history of chronic DVT (> 10 days).10The median was 4 days duration of symptoms in our cases although the range was up to 60 days. It may result from different patients’ compositions such as more May-Thurner syndrome patients, or higher rate of suprainguinal DVT involvement than other reports.
Catheter directed thrombolysis with adjunctive mechani- cal thrombus removal is becoming the standard for the catheter based management of DVT,1,2and contemporary venous thrombectomy has substantially improved early and long term results.1-3,5Numerous devices have been recently released for pharmacomechanical thrombolysis.3,5 We performed a mechanical thrombectomy by manual aspiration, i.e., we did not use the thrombectomy devices.
It is difficult to use newly developed catheters, such as the Trellis catheter, the AngioJet system, or an ultrasound incorporating system in our public health system because public health insurance does not cover the cost of the catheters. However, Lin, et al.5showed no statistical differ- ence between thrombus removal rates for the pharmaco- mechanical thrombectomy using the AngioJet system and catheter direct thrombolysis. The complete thrombus free rate was 67% in the present study and 75% for Angiojet catheter-directed thrombolysis in the report by Lin, et al.5 The conventional manual aspiration can be an alternative for thrombectomy in the absence of special catheter systems.
Acute pulmonary embolismis a major morbidity of acute DVT.1,2In our study cohort, we used a temporary IVC filter Table 4. Clinical Results
Clinical improvement within 48 hours 67 (91%) Treatment success at discharge
Complete thrombus removal 15 (20%)
Partial thrombus 52 (70%)
Treatment failure 7 (10%)
On 6 months follow-up
Complete thrombus removal 50 (72%)
Partial thrombus 15 (22%)
Treatment failure 4 (6%)
DVT recurrence 6 (8%)
Post-thrombotic syndrome 28 (38%) Complications
Hematoma formation requiring transfusion 1 (1%)
Minor bleeding 3 (4%)
DVT, deep vein thrombosis.
DISCUSSION
in 60 (81%) of the patients to prevent thrombus emboliza- tion during the procedures. Currently, prophylactic IVC filter placement is performed without departmental gui- delines. IVC filter insertion is recommended in patients with a free floating IVC thrombus that is longer than 5 cm.1The incidence of preoperative pulmonary embolism at admission in our study was 61%, which was higher than the 10-26 % previously reported.11,12 This may have been due to a higher rate of suprainguinal DVT involvement in our patients (77%), or routine preoperative MDCT pulmo- nary angiography check up. Post-thrombotic syndrome, which is the most important late complication, has been reported to occur in 29% to 79% of acute DVT cases.14 Valvular insufficiency and residual obstruction are primary contributors to venous hypertension, which may result in limb edema, hyperpigmentation, or ulceration.15Experi- mental reports on acute DVT in canine models have demonstrated that thrombolysis preserves endothelial function and valve competence.16 Early post-thrombotic syndrome in our cohort at a 3 month follow-up (39%) could be lower on later follow up periods, considering that the 20% complete thrombus removal rate at discharge imp- roved to 67% on a 6 months follow-up. Our mid-term follow up via telephone interview (81%) showed asympto- matic in 46% of patients and moderate improvement in 46%.
The reported complications of catheter-directed throm- bolysis are bleeding, pulmonary embolism, and death.1,2In the present study, there was no death. 5% of patients de- veloped a bleeding complication, but only one case had a retroperitoneal hematoma and required a transfusion.
We conclude that catheter-directed thrombolysis by conventional aspiration thrombectomy is an effective treat- ment for lower extremity deep vein thrombosis, and the clinical results achieved were satisfactory.
This work was supported by research grant from INHA University.
1. Meissner MH, Wakefield TW, Ascher E, Caprini JA, Comerota AJ, Eklof B, et al. Acute venous disease: venous thrombosis and
venous trauma. J Vasc Surg 2007;46 Suppl S:25S-53S.
2. Comerota AJ, Gravett MH. Iliofemoral venous thrombosis. J Vasc Surg 2007;46:1065-76.
3. Comerota AJ, Paolini D. Treatment of acute iliofemoral deep venous thrombosis: a strategy of thrombus removal. Eur J Vasc Endovasc Surg 2007;33:351-60.
4. Plate G, Akesson H, Einarsson E, Ohlin P, Eklof B. Long-term results of venous thrombectomy combined with a temporary arterio-venous fistula. Eur J Vasc Surg 1990;4:483-9.
5. Lin PH, Zhou W, Dardik A, Mussa F, Kougias P, Hedayati N, et al. Catheter-direct thrombolysis versus pharmacomechanical thrombectomy for treatment of symptomatic lower extremity deep venous thrombosis. Am J Surg 2006;192:782-8.
6. Nordström M, Lindblad B, Bergqvist D, Kjellström T. A pros- pective study of the incidence of deep-vein thrombosis within a defined urban population. J Intern Med 1992;232:155-60.
7. Anderson FA Jr, Wheeler HB, Goldberg RJ, Hosmer DW, Pat- wardhan NA, Jovanovic B, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med 1991;151:933-8.
8. Husmann MJ, Heller G, Kalka C, Savolainen H, Do DD, Schmi- dli J, et al. Stenting of common iliac vein obstructions combined with regional thrombolysis and thrombectomy in acute deep vein thrombosis. Eur J Vasc Endovasc Surg 2007;34:87-91.
9. Kölbel T, Lindh M, Holst J, Uher P, Eriksson KF, Sonesson B, et al. Extensive acute deep vein thrombosis of the iliocaval segment:
midterm results of thrombolysis and stent placement. J Vasc Interv Radiol 2007;18:243-50.
10. Mewissen MW, Seabrook GR, Meissner MH, Cynamon J, Labropoulos N, Haughton SH. Catheter-directed thrombolysis for lower extremity deep venous thrombosis: report of a national multicenter registry. Radiology 1999;211:39-49.
11. Verhaeghe R, Stockx L, Lacroix H, Vermylen J, Baert AL.
Catheter-directed lysis of iliofemoral vein thrombosis with use of rt-PA. Eur Radiol 1997;7:996-1001.
12. Berry RE, George JE, Shaver WA. Free-floating deep venous thrombosis. A retrospective analysis. Ann Surg 1990;211:719-2.
13. Beyth RJ, Cohen AM, Landefeld CS. Long-term outcomes of deep-vein thrombosis. Arch Intern Med 1995;155:1031-7.
14. Monreal M, Martorell A, Callejas JM, Valls R, Llamazares JF, Lafoz E, et al. Venographic assessment of deep vein thrombosis and risk of developing post-thrombotic syndrome: a prospective study. J Intern Med 1993;233:233-8.
15. Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr. Rela- tionship between changes in the deep venous system and the development of the postthrombotic syndrome after an acute episode of lower limb deep vein thrombosis: a one- to six-year follow-up. J Vasc Surg 1995;21:307-12.
16. Rhodes JM, Cho JS, Gloviczki P, Mozes G, Rolle R, Miller VM.
Thrombolysis for experimental deep venous thrombosis main- tains valvular competence and vasoreactivity. J Vasc Surg 2000;
31:1193-205.