Vol. 13, No. 1, March, 2006
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
<접수일:2005년 7월 15일, 심사통과일:2006년 2월 27일>
※통신저자:정 원 태
부산시 서구 동대신동 3가 1번지 동아대학교 의과대학 내과학교실
Tel:051) 240-2954, Fax:051) 245-2954, E-mail:[email protected] 이 논문은 2004학년도 동아대학교 학술연구비(공모과제) 지원에 의하여 연구되었음.
Association of Anti-cyclic Citrullinated Peptide (CCP) Antibodies and Functional Status in Rheumatoid Arthritis
Kyeong Hee Kim, M.D., Sung Won Lee, M.D.*, Won Tae Chung, M.D.*
Departments of Laboratory Medicine and Internal Medicine*, Dong-A University College of Medicine, Busan, Korea
= 국문초록 =
류마티스 관절염에서 항-CCP 항체와 기능적 상태와의 상관성
동아대학교 의과대학 진단검사의학교실, 내과학교실*
김 경 희․이 성 원*․정 원 태*
목적: 류마티스 관절염에서 항-CCP 항체와 임상 소견 및 검사실 소견 사이의 상관성을 횡단면적 으로 조사하였다.
방법: 미국류마티스협회의 기준에 의해 진단된 114명의 류마티스 관절염 환자를 대상으로 하였 다. 임상 소견으로 나이, 성별, 질병의 기간, 기능적 상태를 조사하였고, 검사실 소견으로는 총 백혈 구 수, 혈색소, 혈소판 수, 적혈구 침강속도, C-반응단백을 검사하였다. 항-CCP 항체와 함께 분석한 자가항체는 류마티스 인자, 항핵항체, 항핵주위인자였다.
결과: 항-CCP 항체는 대상 환자의 67.5% (77/114)에서 양성이었고, 류마티스 관절염의 기능적 상태가 나쁠수록 항-CCP 항체의 양성률이 의미 있게 높았다(functional class I/II vs III/IV, p<0.0001, OR=1.67). 항-CCP 항체 양성률은 류마티스 인자(p<0.0001), 항핵주위인자(p=0.018)의 양성과는 상 관성이 있었으나 다른 임상적 검사실적 소견과는 연관성이 없었다.
결론: 항-CCP 항체가 류마티스 관절염의 나쁜 기능적 상태와 연관성이 있었기 때문에 항-CCP 항체의 류마티스 관절염의 예후에 미치는 영향에 대한 추가적인 연구가 필요할 것으로 생각된다.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Rheumatoid arthritis, Anti-cyclic citrullinated peptide antibodies, Rheumatoid factor,
Anti-perinuclear factor, Autoantibody
INTRODUCTION
Rheumatoid arthritis (RA) is one of the most preva- lent systemic rheumatic diseases, affecting 1∼2% of the population worldwide (1). RA has been diagnosed according to clinical presentations and rheumatoid fac- tor (RF) is one of the classification criteria proposed by the American College of Rheumatology (ACR) (2).
However, RF has a low specificity because it may be found in healthy elderly individuals and in patients with other autoimmune diseases or chronic infec- tions (3-5). Early intervention with highly effective dis- ease modifying antirheumatic drugs (DMARDs) results in a better control of the disease. Therefore, it is important to differentiate between RA and self-limiting arthritis (6-9).
Recently, a new serological test, the anti-cyclic ci- trullinated peptide (CCP) antibodies enzyme linked im- munosorbent assay (ELISA) was developed and it has an excellent specificity for the diagnosis of RA, espe- cially in patients with early disease (10-12). In this study we evaluated the relationship between anti-CCP antibodies and various clinical and laboratory para- meters in RA patients.
MATERIALS AND METHODS
One hundred and fourteen patients (95 women and 19 men; mean age, 51.1 years; range, 23∼80 years) attending the rheumatology unit of the Dong-A Uni- versity Hospital were included. All patients were diag- nosed RA according to the revised criteria of ACR (2).
For analysis of specificity, 202 non-RA controls were selected: systemic lupus erythematosus (SLE) (n=31), Sjogren's syndrome (n=3), mixed connective tissue dis- ease (MCTD) (n=4), systemic sclerosis (n=1), polymyo- sitis (n=3), osteoarthritis (n=40), Raynaud syndrome (n=1), palindromic rheumatism (n=4), fibromyalgia syn- drome (n=9), ankylosing spondylitis (n=4), adult- onset Still's disease (n=4), juvenile RA (n=4), gout (n=9),
Bechet's disease (n=8), unclassified arthritis (n=11), other diseases (n=10), and healthy subjects (n=56). The serum samples were aliquoted and stored at -20oC until use.
Among the RA patients, the variables recorded were age, gender, time from diagnosis, and functional sta- tus (13). Laboratory parameters tested were WBC, he- moglobin, platelet count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Analyzed auto- antibodies were RF, anti-CCP, antinuclear antibodies (ANA), and anti-perinuclear factors (APF).
Anti-CCP antibodies were determined by an ELISA using a commercial anti-CCP assay (Euro-Diagnostica, MALMö, Sweden). The assay was performed according to the manufacturer's protocol. RF was measured by immunoturbidimetry (LX-2200, Eiken Chemical Co., Tokyo, Japan). ANA was assayed by indirect immuno- fluorescence on HEp-2 cells (fluoroHEPANA, MBL, Japan), and APF by indirect immunofluorescence (IT- APF, ImmunoThink, Seoul, Korea).
Statistical analysis was performed using the SPSS 10.1 (SPSS, Chicago, USA). Subgroups of RA patients who were positive and negative for anti-CCP were compared by means of Student's t-test (for continuous variables) and the chi-square test (for discrete variables).
Odds ratio and 95% confidence interval between anti-CCP positivity and functional class were calculated using chi-square statistics. Correlations between anti- CCP and autoantibodies were analyzed by using Pear- son correlation coefficient. The level of statistical sig- nificance was established at p<0.05.
RESULTS 1. Association of anti-CCP with RA
The demographic and clinical characteristics of RA patients according to anti-CCP are shown in Table 1.
Anti-CCP were found in 77 (67.5%) of 114 RA pa- tients and anti-CCP positive RA patients had a mean antibody concentration of 564.5 (range, 27∼4,717) unit.
Only 8 of 202 control sera (4.0%) showed a positive
reaction: 1 SLE, 1 MCTD, 2 osteoarthritis, 2 palin- dromic rheumatism, and 2 healthy subjects. The sensitivity of anti-CCP was 67.5% and specificity was 96.0%. There was no significant association between anti-CCP positivity and patient's gender, age, and dis- ease duration. When the functional status of RA pa- tients was considered, anti-CCP positivity was signif- icantly associated with more severe disease (functional class I/II vs III/IV, p<0.0001, OR=1.67) (Table 1).
2. Association between anti-CCP and RF
RF was detected in 75 (65.8%) of 114 RA patients and a mean concentration of RF was 178.9 (range, 14.7∼872.5) IU/mL. RF was detected in 31 (15.3%) of 202 control sera. The sensitivity of RF was 65.8%
and specificity was 84.7%. Anti-CCP antibodies alone were present in 13 patients (11.4%), corresponding to 33.3% of all RF negative patients. RF was the only detected antibody in 11 (9.6%) patients and 25 patients (21.9%) were negative for both anti-CCP antibodies and RF. A relatively low level of correlation was found between anti-CCP titers and RF titers (p=0.023, Pearson correlation coefficient, r=0.213) (Fig. 1) but there was a strong association between RF and anti-
CCP positivity (p<0.0001, Pearson correlation coeffi- cient, r=0.448). In relationship between functional sta- tus and RF positivity, RF positivity was significantly higher in advanced group (p=0.043, data not shown).
3. Association of anti-CCP and other autoanti- bodies
APF and ANA were detected in 21 (33.3%) of 63, and 20 (44.4%) of 45 RA patients, respectively. The significant association was observed only for APF (p=
0.018, Pearson correlation coefficient, r=0.298), but not for ANA (p=0.885).
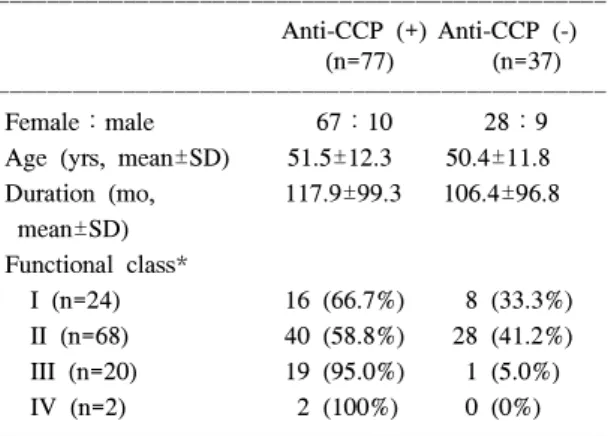
Table 1. Clinical characteristics of rheumatoid arthritis pa- tients according to anti-CCP positivity
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Anti-CCP (+) Anti-CCP (-)
(n=77) (n=37)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Female:male 67:10 28:9
Age (yrs, mean±SD) 51.5±12.3 50.4±11.8 Duration (mo, 117.9±99.3 106.4±96.8 mean±SD)
Functional class*
I (n=24) 16 (66.7%) 8 (33.3%) II (n=68) 40 (58.8%) 28 (41.2%) III (n=20) 19 (95.0%) 1 (5.0%) IV (n=2) 2 (100%) 0 (0%) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*anti-CCP positivity, class I/II (56/92, 60.9%) vs III/IV (21/22, 95.5%): p<0.0001, OR=1.67 (95% confidence interval 1.42∼1.98)
Table 2. Laboratory characteristics of patients with rheu- matoid arthritis according to anti-CCP positi- vity
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Anti-CCP (+) Anti-CCP (-)
Parameters p-value
(n=77) (n=37)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ WBC (mm3) 8,476±2,548 8,130±2,954 0.521 Hemoglobin (g/dL) 12.1±1.6 12.7±1.7 0.092 Platelet count
307.7±86.3 313.3±80.3 0.742 (×103/mm3)
ESR (mm/hr) 35.5±28.3 26.8±24.0 0.109 CRP (mg/dL) 1.25±1.73 0.99±1.64 0.442 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ WBC: white blood cells, ESR: erythrocyte sedimentation rate, CRP: C-reactive protein
Fig. 1. Relationship between anti-CCP and RF levels (r=0.213, p=0.023).
4. Association of anti-CCP and laboratory parame- ters
No differences were observed in WBC, hemoglobin, platelet count, ESR, and CRP between anti-CCP posi- tive and negative patients (Table 2).
DISCUSSION
Although the presence of RF was identified in pa- tients with RA over 50 years ago (14), the RF assay remains suboptimal as a diagnostic test as it lacks sensi- tivity (54∼88%) and specificity (48∼92%) (10,12,15-17).
The shortcomings of the RF assay have provided stim- ulus for identification of other serological assays for RA. This search has yielded serological reactivity to a number of autoantigens in subsets of patients with RA, including antikeratin antibodies (18), Sa (19), BiP (20), RA33 (21), glucose-6-phosphate isomerase (22), and APF (23). Although, these autoantibodies have all de- monstrated lower sensitivity for diagnosis of RA than RF, many of them are present almost exclusively in patients with RA. Analysis of antikeratin antibody and APF showed that most of the reactivity present against these antigens was directed against citrulline residues, a post-translational modification of the amino acid arginine (24). This discovery led to the development of assays employing CCP to measure antibodies recog- nizing citrullinated antigens as a diagnostic test for RA.
In addition, the role of anti-CCP in the pathogenesis of RA remains to be established. A recent study has shown that there is a RA susceptibility haplotype in the peptidylarginine deiminases (PADIs) gene citrul- linating enzymes and a PADI4 haplotype is associated with higher levels of antibodies to citrullinated peptide in RA patients (25).
Initial studies containing the frequency of antibodies to CCP in mixed cohorts characterizing patients with rheumatic diseases, infectious diseases, and healthy pa- tients, have shown it to be moderately sensitive (68%) but highly specific (98%) for RA (10). Furthermore, in
a clinical model for the prediction of arthritis outcome, anti-CCP positivity had the highest odds ratio for persis- tent erosive arthritis among 7 diagnostic variables (26).
Recently in an early arthritis cohort, anti-CCP antibod- ies were a predictor of progression to RA in patients with undifferentiated arthritis (27). In the present study, the specificity of anti-CCP antibodies (96%) was high- er than that of the RF (84.6%) and the sensitivity of anti-CCP antibodies (67.5%) was similar to that of RF (65.8%). This sensitivity and specificity of anti-CCP in our study confirms the results of previous stud- ies (11,12,28).
We investigated the associations between clinical and laboratory parameters and anti-CCP positivity in 114 RA patients by conducting a cross-sectional study. The positivity of anti-CCP was significantly different ac- cording to functional class and RA patients with more advanced functional class showed higher anti-CCP positivity. It is not certain whether the higher frequ- ency of anti-CCP in advanced group of RA is a con- sequence or a cause. But it is suggested that anti-CCP antibodies might be a prognostic indicator for the de- velopment of more aggressive disease. There are sev- eral predictors of radiological progression in patients with RA, of which IgM RF has the highest prognostic value. Other serologic markers such as IgA RF, IgG RF, antineutrophil cytoplasmic antibody, and ANA show a considerable disagreement (29-31). Recently, Forslind et al (32) reported the presence of anti-CCP was associated with significantly higher Larsen score at baseline and at end point after two years of follow up in early RA patients. Overall, these data support that anti-CCP and RF have a similar ability to predict radio- logic outcome in RA. In present study, both RF and anti-CCP were associated with higher functional class.
In conclusion, anti-CCP positivity was significantly associated with more advanced functional class in RA patients and further evaluation for the prognostic value of anti-CCP in RA is needed.
CONCLUSION
We investigated the associations between anti-CCP antibodies and clinical and laboratory parameters in 114 RA patients. Anti-CCP antibodies were detected in 67.5% (77/114) of RA patients and anti-CCP positivity was significantly associated with more severe disease.
Anti-CCP positivity was associated with rheumatoid factor and anti-perinuclear factor, but not with other clinical or laboratory parameters. Since anti-CCP anti- bodies are significantly associated with functional class of the disease, further evaluation for the prognostic value of anti-CCP in RA is needed.
REFERENCES
1) O'dell JR. Rheumatoid arthritis: the clinical picture.
In: Koopman WJ, Moreland LW, eds. Arthritis and allied conditions. 15th ed. p. 1165-9, Philadelphia, Lippincott Williams & Wilkins, 2005.
2) Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheuma- tism Association 1987 revised criteria for the clas- sification of rheumatoid arthritis. Arthritis Rheum 1988;31:315-24.
3) Newkirk MM. Rheumatoid factors: what do they tell us? J Rheumatol 2002;29:2034-40.
4) Spadaro A, Riccieri V, Terracina S, Rinaldi T, Taccari E, Zoppini A. Class specific rheumatoid factors and antiphospholipid syndrome in systemic lupus erythe- matosus. Lupus 2000;9:56-60.
5) Witte T, Hartung K, Sachse C, Matthias T, Fricke M, Kalden JR, et al. Rheumatoid factors in systemic lupus erythematosus: associated with clinical and lab- oratory parameters. Rheumatol Int 2000;19:107-11.
6) Egsmose C, Lund B, Borg G, Pettersson H, Berg E, Brodin U, et al. Patients with rheumatoid arthritis benefit from early 2nd line therapy: 5 year follow up of a prospective double blind placebo controlled study. J Rheumatol 1995;22:2208-13.
7) Van der Heide A, Jacobs JW, Bijlsma JW, Heurkens AH, Van Booma-Frankfort C, Van der Veen MJ, et al. The effectiveness of early treatment with “sec- ond-line” antirheumatic drugs: a randomized con- trolled trial. Ann Intern Med 1996;124:699-707.
8) Symmons DP, Jones MA, Scott DL, Prior P. Long- term mortality outcome in patients with rheumatoid arthritis: early presenters continue to do well. J Rheu- matol 1998;25:1072-7.
9) Anderson JJ, Wells G, Verhoeven AC, Felson DT.
Factors predicting response to treatment in rheumatoid arthritis: the importance of disease duration. Arthritis Rheum 2000;43:22-9.
10) Schellekens GA, Visser H, De Jong BA, Van den Hoogen FH, Hazes JM, Breedveld FC, et al. The diagnostic properties of rheumatoid arthritis antibod- ies recognizing a cyclic citrullinated peptide. Arthritis Rheum 2000;43:155-63.
11) Vasishta A. Diagnosing early-onset rheumatoid arthri- tis: the role of anti-CCP antibodies. Am Clin Lab 2002;21:34-6.
12) Bizzaro N, Mazzanti G, Tonutti E, Villalta D, Tozzoli R. Diagnostic accuracy of the anti-citrulline antibody assay for rheumatoid arthritis. Clin Chem 2001;47:
1089-93.
13) Hochberg MC, Chang RW, Dwosh I, Lindsey S, Pincus T, Wolfe F. The American College of Rheu- matology 1991 revised criteria for the classification of global functional status in rheumatoid arthritis. Ar- thritis Rheum 1992;35:498-502.
14) Rose HM, Ragan C, Pearce E, Lipman MO. Differen- tial agglutination of normal and sensitized sheep erythrocytes by sera of patients with rheumatoid arthritis. Proc Soc Exp Biol Med 1949;68:1-6.
15) Weinblatt ME, Schur PH. Rheumatoid factor detection by nephelometry. Arthritis Rheum 1980;23:777-9.
16) Saraux A, Berthelot JM, Chales G, Le Henaff C, Mary JY, Thorel JB, et al. Value of laboratory tests in early prediction of rheumatoid arthritis. Arthritis Rheum 2002;47:155-65.
17) Bas S, Perneger TV, Kunzle E, Vischer TL. Compara- tive study of different enzyme immunoassay for measurement of IgM and IgA rheumatoid factors.
Ann Rheum Dis 2002;61:505-10.
18) Young BJ, Mallya RK, Leslie RD, Clark CJ, Hamblin TJ. Antikeratin antibodies in rheumatoid arthritis. Br Med J 1979;2:97-9.
19) Hayem G, Chazerain P, Combe B, Elias A, Haim T, Nicaise P, et al. Anti-Sa antibody is an accurate diagnostic and prognostic marker in adult rheumatoid arthritis. J Rheumatol 1999;26:7-13.
20) Blass S, Specker C, Lakomek HJ, Schneider EM, Schwochau M. Novel 68 kDa autoantigen detected by rheumatoid arthritis specific antibodies. Ann Rheum
Dis 1995;54:355-60.
21) Hassfeld W, Steiner G, Graninger W, Witzmann G, Schweitzer H, Smolen JS. Autoantibody to the nuclear antigen RA33: a marker for early rheumatoid arthritis. Br J Rheumatol 1993;32:199-203.
22) Schaller M, Burton DR, Ditzel HJ. Autoantibodies to GPI in rheumatoid arthritis: linkage between an ani- mal model and haman disease. Nat Immunol 2001;
2:746-53.
23) Nienhuis RL, Mandema E. A new serum factor in patients with rheumatoid arthritis, the antiperinuclear factor. Ann Rheum Dis 1964;23:302-5.
24) Schellekens GA, De Jong BA, Van den Hoogen FH, Van de Putte LB, Van Venrooij WJ. Citrulline is an essential constituent of antigenic determinants recog- nized by rheumatoid arthritis-specific autoantibodies.
J Clin Invest 1998;101:273-81.
25) Suzuki A, Yamada R, Chang X, Tokuhiro S, Sawada T, Suzuki M, et al. Functional haplotypes of PADI4, encoding citrullinating enzyme peptidylarginine dei- minase 4, are associated with rheumatoid arthritis. Nat Genet 2003;34:395-402.
26) Visser H, Cessie SL, Vos K, Breedveld FC, Hazes JM. How to diagnose rheumatoid arthritis early: a prediction model for persistent (erosive) arthritis.
Arthritis Rheum 2002;46:357-65.
27) Van Gaalen FA, Linn-Rasker SP, Van Venrooij WJ, de Jong BA, Breedveld FC, Verweij CL, et al. Auto-
antibodies to cyclic citrullinated peptides predict pro- gression to rheumatoid arthritis in patients with un- differentiated arthritis. A prospective cohort study.
Arthritis Rheum 2004;50:709-15.
28) Van Boekel MA, Vossennaar ER, Van den Hoogen FH, Van Venrooij WJ. Autoantibody systems in rheumatoid arthritis: specificity, sensitivity and diag- nostic value. Arthritis Res 2002;4:87-93.
29) Bas S, Perneger TV, Seitz M, Tiercy JM, Roux- Lombard P, Guerne PA. Diagnostic tests for rheu- matoid arthritis: comparison of anti-cyclic citrullinat- ed peptide antibodies, anti-keratin antibodies and IgM rheumatoid factors. Rheumatology 2002;41:809-14.
30) Vittecoq O, Pouplin S, Krzanowska K, Jouen-Beades F, Menard JF, Gayet A, et al. Rheumatoid factor is the strongest predictor of radiological progression of rheumatoid arthritis in a three year prospective study in community-recruited patients. Rheumatology 2003;
42:1-8.
31) Bas S, Genevay S, Meyer O, Gabay C. Anti-cyclic citrullinated peptide antibodies, IgM and IgA rheuma- toid factors in the diagnosis and prognosis of rheu- matoid arthritis. Rheumatology 2003;42:677-80.
32) Forslind K, Ahlmen M, Eberhardt K, Hafstrom I, Svensson B; BARFOT Study Group. Prediction of radiological outcome in early rheumatoid arthritis in clinical practice: role of antibodies to citrullinated peptides (anti-CCP). Ann Rheum Dis 2004;63:1090-5.
Abstract ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Objective: The purpose of this cross-sectional study was to investigate the association between anti-cyclic citrullinated peptide (CCP) antibodies and clinical and laboratory parameters in rheumatoid arthritis (RA) patients.
Methods: We studied 114 patients with RA, diagnosed according to the revised criteria of American College of Rheumatology. Clinical informations were collected such as age, sex, func- tional status, and disease duration. Tested laboratory parameters were WBC, hemoglobin, platelet count, erythrocyte sedimentation rate, and C-reactive protein. Analyzed autoantibody profiles were rheumatoid factor, anti-nuclear antibodies, and anti-perinuclear factors.
Results: Anti-CCP antibodies were detected in 67.5% (77/114) of RA patients and anti-CCP positive RA patients had a mean antibody concentration of 564.5±755.7 (range, 27∼4717) units. Anti-CCP positivity was significantly associated with more severe disease (functional class I/II vs III/IV, p<0.0001, OR=1.67). Anti-CCP positivity was associated with rheumatoid factor (p<
0.0001) and anti-perinuclear factor (p=0.018), but not with other clinical or laboratory parameters.
Conclusion: Since anti-CCP antibodies are significantly associated with functional class of the disease, further evaluation for the prognostic value of anti-CCP in RA is needed.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ