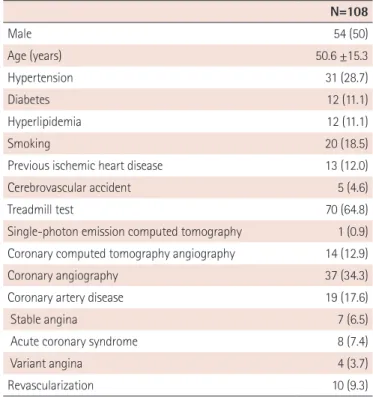
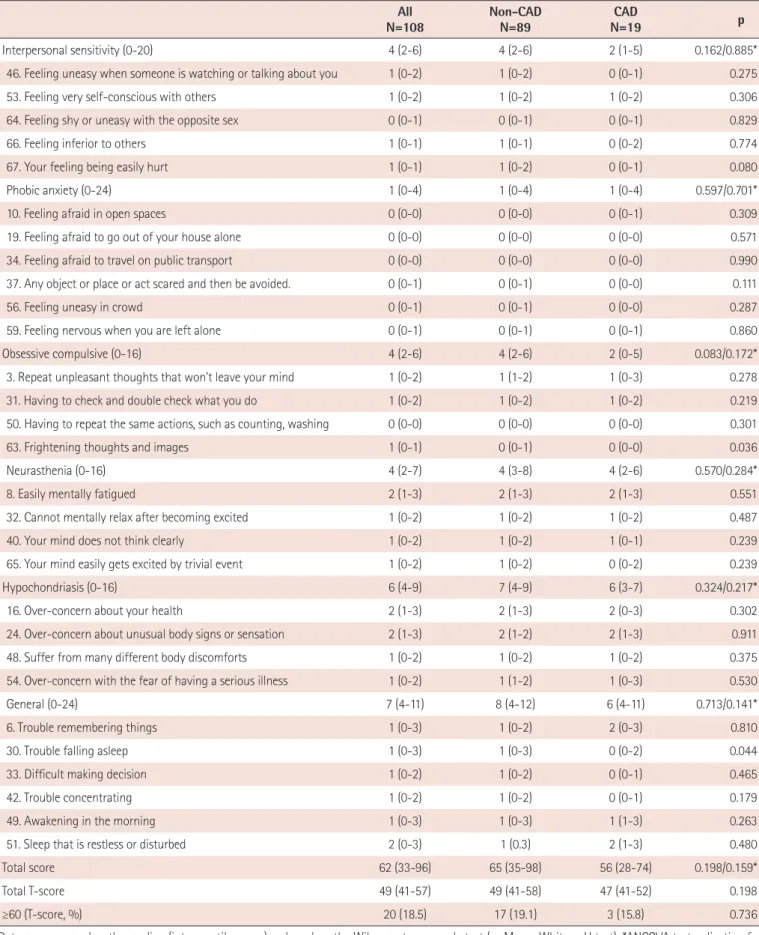
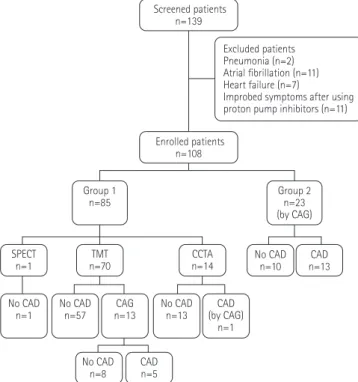
Psychiatric Characteristics of the Cardiac Outpatients with Chest PainJea-Geun Lee, MD, Joon Hyouk Choi, MD, Song-Yi Kim, MD, Ki-Seok Kim, MD, and Seung-Jae Joo, MD
10
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
수치

관련 문서
– Mechanisms of overpressure generation – Estimating pore pressure at depth.. Zoback MD, 2007, Reservoir Geomechanics,
Seung Soo Jang Sung Gyun Shin Min Jae Lee Sang Soo Han Chan Ho Choi Sungkyum Kim Woo Sung Cho and Song Hyun Kim POSTECH Yeong Rok Kang Wol Soon Jo Soo Kyung Jeong and
The purpose of this study was to identify the frequency and related factors of advanced airway management for patients with cardiac arrest by the
Result: During the study period, 482 patients had elevated cardiac troponin-T levels. The positive predictive value for the.. The diagnostic importance of
Chang Goo Kang, Ah Hyun Park, Jang Ho Ha, Young Soo Kim, Joon-Ho Oh, Jeong Min Park, Soo Mee Kim, Seung-Jae Lee, Seung Hee Lee, and Han Soo Kim(KAERI). Fabrication
Chang Je Park, Kwoen Ho Kang, Sang Ho Na, Young Hee Kim, Ho Jin Ryu, Geun Il Park, and Kee Chan Song (KAERI). Geun-Suk Choi and
Sang-Keun Woo, Yong Jin Lee, WonHo Lee, Min Hwan Kim, Ji Ae Park, In Ok Ko, Jin Su Kim, Jong Guk Kim, Young Hoon Ji, Joo Hyun Kang, Gi Jeong Cheon, Chang Woon Choi, Sang Moo
IL Soon Hwang, Myung Hyun Kim, Han Gyu Joo, Kyung Woo Yi, Bong Yoo, Moo Hwan Kim, Seung Rok Oh, Yoon Jae Kim, Jong Gye Shin, Kwang Myung Lee, Jae Yong
