서 론
유리체절제술과 백내장병합수술은 유리체망막 질환 환자에 있 어서 백내장이 같이 동반되어 있을 경우 흔하게 시행되는 수술이
다 유리체절제술만을 단독으로 시행했을 시 백내장으로 인해 망. 막의 관찰이 어려울 수 있으며 년 내에 백내장이 진행할 수 있, 2 다는 단점이 있다.1또한 선행 연구에 의하면 유리체절제술과 백 내장병합수술은 순차적인 수술과 비교하여 망막 질환과 백내장을 동시에 치료할 수 있는 안전하고 효과적인 방법이며 추가 수술을 피할 수 있어 경제적으로도 비용 절감에 도움이 되고 안구의 해, 부학적 회복 또한 만족할 만하다.2-5따라서 특히 특발성 망막앞 막처럼 수술 후 기대되는 시력 호전의 정도가 클수록 정확한 인, 공수정체 도수 예측력이 중요하다고 할 수 있겠다.
본 연구에서는 특발성 망막앞막 환자에서 A-scan과 IOL 로
master 측정한 유리체절제술과 백내장병합수술 전 목표 굴절
특발성 망막앞막 환자에서 유리체절제술과 백내장병합수술 후 굴절력 예측
연세대학교 의과대학 안과학교실 시기능개발연구소1, 국민건강보험 일산병원 안과2
김주연
1,2, 한승수
2, 정은지
2Accuracy of Intraocular Lens Power Estimation in Eyes Undergoing Phacovitrectomy for Idiopathic Epiretinal Membrane
Joo Yeon Kim1,2, John Seungsoo Han2, Eun Jee Chung2
1Department of Ophthalmology,Institute of Vision Research, Severance Hospital, Yonsei University, College of Medicine, Seoul, Korea
2Department of Ophthalmology, National Health Insurance Service Ilsan Hospital, Goyang, Korea
Background: To evaluate the accuracy of intraocular lens (IOL) power estimation and factors associated with outcomes in eyes undergoing combined phacovitrectomy for idiopathic epiretinal membrane.
Method: We performed a retrospective case review of 33 eyes that underwent phacovitrectomy for idiopathic epiretinal membrane.
Axial lengths were measured using ultrasound (A-scan) or optical biometry (IOL Master) or both. Achieved and predicted refrac- tions were compared to calculate mean postoperative refractive prediction error (ME) and mean absolute prediction error (MAE).
Systemic conditions of patients and several pre-operative and post-operative factors related to post-operative refraction were analyzed.
Result: Mean prediction errors (ME) of 33 eyes measured by A-scan and IOL master were -0.46 ± 0.47 diopters (D) and -0.36 ± 0.44 D after 3 months, respectively. A statistically significant myopic shift was identified with A-scan measurement(p=0.045).
Mean absolute prediction errors (MAE) measured by A-san and IOL master were 0.53 ± 0.38 D and 0.31 ± 0.31 D after 3 months, respectively with no statistical significant differences between results (p = 0.197). The amount of decrease in central macular thickness after surgery was significantly associated with greater myopic shift in IOL master measurements(p=0.037).
Conclusion: Combined phacovitrectomy for idiopathic epiretinal membrane showed small biometric errors within the tolerable range in most cases. Both optical biometry and ultrasound should be used to estimate axial lengths for improving the accuracy of IOL power calculations.
Key Words: Epiretinal membrane, Intraocular lens power estimation, Phacovitrectomy
책임저자 정은지:
경기도 고양시 일산동구 일산로
10444 100
국민건강보험 일산병원 안과
전화: (031)900-0590, 팩스: 0303-3448-7107 E-mail : [email protected]
본 연구는 국민건강보험 일산병원의 연구비 지원으로 이루어졌음
*
(NHIMC 2017CR038).
력과 수술 후 실제 굴절력 사이에 어떤 차이가 있는지 분석하고, 굴절력에 영향을 미치는 요소에 대해 알아보고자 한다.
대상 및 방법
년 월부터 년 월까지 국민건강보험 일산병원 2011 11 2015 12
에서 숙련된 두 명의 술자에게 망막앞막과 백내장 진단 하 유리체 절제술과 백내장병합수술을 시행받고 개월 이상 경과 관찰이 가6 능하여 현성 굴절 검사를 시행한 명33 , 33안 환자들의 의무기록 을 후향적으로 분석하였다 포도막염 외상 망막혈관질환 망막. , , , 박리 수술 등에 의한 이차성 망막앞막 유리체황반견인증후군이, 나 황반 원공이 동반되어있거나 이전의 안내 수술을 받은 수술력 이 있는 환자는 대상에서 제외하였다 본 연구는 기관생명윤리위. 원회의 승인을 받아(2017-04-022-002) 진행하였다.
안축장의 길이는 A-scan(EchoScan US-1800, Nidek, 과
Gamagori, Japan) IOL master (IOL Master®, Ziess, 를 모두 이용하여 측정하였다 모든 검사는 숙
Jena, Germany) .
련된 한 명의 검사자에 의해 시행되었으며, 10회 이상 측정한 결 과 중 가장 신뢰할 만한 결과값을 택하였다.
인공수정체의 도수결정과 이에 따른 예상 굴절력은 SRK-T 공 식을 이용했으며 두 가지 방법 모두 내장된 소프트웨어를 이용해 , 계산하였다.
술 전 목표한 굴절력과 술 후 현성굴절검사를 통한 구면렌즈대 응 굴절력을 비교하였다 굴절예측이상값은 술 후 구면렌즈대응 . 굴절력과 술 전 목표 굴절력의 차이를 평균 예측오차(mean pre-
으로 계산하여 음의 값인 경우 술 전 목표보다 diction error, ME)
근시화된 것으로 양의 값인 경우 원시화된 것으로 평가하였고 두 , 굴절력 차의 절대값을 평균 절대예측오차(mean absolute pre-
으로 정의하여 결과 측정치로 확인하였다
diction error, MAE) .
대상 환자들의 수술 전과 수술 후 3, 6개월에 최대 교정 시력, 안압 굴절값을 조사하였다 최대 교정 시력은 스넬렌, . (Snellen) 시력표를 이용하여 측정하였으며, LogMAR(Logarithm of mini- mum angle of resolution)로 변환하였다 굴절값은 현성 굴절 . 검사를 이용하여 측정하고 구면대응치(Spherical equivalent) 로 환산하였다.
수술 전후의 중심망막두께는 빛간섭단층촬영(Spectral do- main optical coherence tomography, Cirrus OCT, Carl Zeiss
을 이용하여 측정하였다 meditec, Inc., Dublin, CA, USA) .
수술 방법은 전신 마취 혹은 구후마취 하에 각막 윤부에서 후방의 하이측에 공막 천자 후 상부 투명각막절개를 가 3.5mm
하고 이측 또는 비측에 보조 각막절개를 하였다 동시에 시행된 , .
백내장 수술은 유리체절제술에 앞서 먼저 시행하였다. 26 gauge 주사침을 이용하여 전낭 원형절개를 시행하고 수력분리술 수정, , 체 초음파유화술을 시행한 후 점탄물질로 전낭을 확보한 뒤 10-0
으로 각막절개창을 일시적으로 봉합하였다 이후 각막 윤
Nylon .
부에서 3.5mm 후방의 상비측 상이측에 , 23 혹은 25 gauge 공 막 천자 후 유리체 내 액체 유입기 유리체절제기와 눈속조명을 , 이용하여 유리체절제술을 시행하였다 망막앞막을 제거하였으며. , 을 이용한 내경계막 제거는 일부 환자에서 Indocyanine green
시행하였다 유리체절제 이후 일시적으로 봉합해 놓은 각막절개. 창을 열어 인공수정체(Acrysof IQ [SN60WF; Alcon, Fort Worth, TX, USA], Akreos Adapt[Bausch & Lomb, Rochester, NY, USA], Rayner Superflex 620H[Rayner Intraocular Lenses Limited, Hove, East Sussex, UK], Sensar AR40e [Pharamacia and Upjohn LLC, North Peapack, NJ, USA], CLARE[Cristalens, Lannion, FR], TECNIS ZCB00 [Abbott 를 낭내에 삽입하였다 Medical Optics, Santa Ana, CA, USA]) .
통계프로그램은 SPSS 18.0 (SPSS Inc., Chicago, IL, USA) 을 사용하였다 각각의 환자의 술 후 굴절예측이상 값에 대하여 . paired t-test를 이용하여 분석하였다. p-value가 0.05 미만인 경우를 통계적으로 유의한 것으로 하였다.
결 과
전체 연구대상은 총 33 (33 )명 안 이었고 남자는 17 (51.5%), 명 여자는 명16 (48.5%)이었다 평균연령은 . 66.33 ±7.86세 범위( : 세 이었다 명 중 당뇨 환자는 명 이었으며 52-79 ) . 33 22 (81.8%) , 고혈압 환자는 11명 (33.3%)이었다 수술 전 평균 최대 교정 시. 력은 logMAR 0.57 ±0.23였으며 수술 후 개월째 평균 최대 , 3 교정 시력은 logMAR 0.08 ±0.07로 통계학적으로 유의한 시력 호전을 보였다(p <0.001) (Table 1).
로 측정한 안축장의 길이는 으로 측정한
IOL master A-scan
안축장의 길이보다 더 길게 측정되었다 (23.77 ± 0.95 mm vs 23.58 ± 0.95 mm, p<0.001). A-scan에 의한 평균 목표 굴절 값은 -0.03 ±0.50D, IOL master에 의한 평균 목표 굴절값은 –0.13 ±0.41D이었고 수술 후 개월째 현성굴절검사를 통해 , 3 측정한 실제 평균 굴절값은 -0.49 ±0.58 D이었다.
술 전 중심망막 두께는 474.79 ± 53.32 μm였고 술 후 개월 , 3 째에는 379.94 ± 58.17 μm로 유의한 황반부 두께 감소를 보였 다(p<0.001). 술 후 개월째 굴절값의 평균 예측오차는 3 A-scan 을 이용한 경우에는 -0.46 ± 0.47D이며 IOL master를 이용한 경우에는 -0.36 ± 0.44D으로 나타나, A-scan으로 측정한 것이
유의하게 더 근시편위를 보였다(p=0.045). 술 후 개월 째 3 굴절값 의 평균 절대예측오차는 A-scan을 이용한 경우는 0.53 ± 0.39D,
를 이용한 경우에는
IOL Master 0.47 ±0.32D로 두 검사간 유 의한 차이는 나타나지 않았다 (p =0.197) (Table 2).
당뇨 혹은 고혈압의 기왕력은 황반부 두께 감소와 유의한 상관 관계를 보이지 않았다 각 ( p=0.777, 0.334). 전체 안 중 안33 9 에서 Acrysof IQ, 11안에서 Akreos Adapt, 2안에서 Rayner
안에서 안에서
Superflex 620H, 2 Sensar AR40e, 7 CLARE, 2 안에서 Tecnis ZCB00 렌즈를 삽입하였으며 황반부 두께 감소, 는 렌즈 종류에 따라 유의한 차이가 없었다 (p=0.692).
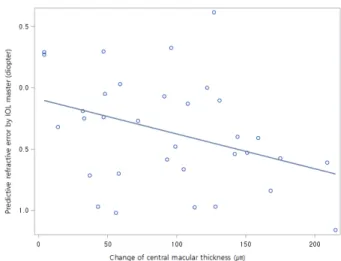
술 후 중심망막두께의 변화량과 굴절값의 평균 예측오차는 의 경우에는 유의하지는 않지만 음의 상관관계
A-scan (r=-0.33;
p=0.060)를 나타냈고, IOL master을 이용한 경우에는 유의한 음의 상관 관계(r=-0.36; p=0.037)를 나타냈다 (Fig. 1, Fig. 2).
고 찰
본 연구에서는 특발성 망막앞막 환자에서 유리체 절제술과 백 내장병합수술을 시행하였을 때에 목표 굴절값에 비해 근시 편위 를 나타냈으나, IOL master가 A-scan보다 더 적은 근시 편위가
Characteristics Results
Total number of eyes 33 eyes
(33 patients) Gender
Male 17 eyes (51.5%)
Female 16 eyes (48.5%)
Age 66.38 ± 8.27
Associated systemic disease
Diabetes mellitus 27 of 33 patients (81.8%)
Hypertension 11 of 33 patients
(33.3%) BCVA (logMAR)
Baseline 0.57 ± 0.23
3 months after surgery 0.08 ± 0.07 Mean axial length measure by A-scan 23.58 ± 0.95 Mean axial length measure by IOL master 23.77 ± 0.95 Mean pre op central macular thickness 474.79 ± 53.32 Mean post op central macular thickness 379.94 ± 58.17 BCVA = best-corrected visual acuity; IOL = intraocular lens.
Table 1. Baseline characteristics of Patients
Group ME MAE
A-scan
After 3 months -0.46 ± 0.47 0.53 ± 0.39 IOL master
After 3 months -0.36 ± 0.44 0.47 ± 0.32
P value 0.045 0.197
Values are presented as mean ± SD.
IOL = intraocular lens.
Table 2. Mean prediction error (ME) and mean absolute prediction error (MAE).
Fig. 1. Correlation between change in central macular thickness and predictive refraction error measured by A-scan. (r=-0.33; p=0.060)
Fig. 2. Correlation between change in central macular thickness and predictive refraction error measured by IOL master. (r=-0.36; p=0.037)
나타나 더 정확한 예측력을 나타냈다는 점을 밝혔다 또한. , IOL 검사에서 술 후 중심망막두께가 더 많이 감소할수록 근시 master
편위가 더 심하게 나타나는 것을 확인할 수 있었다.
최근 백내장 수술과 유리체절제술의 수술 기구와 술기가 발전 함에 따라 여러 유리체망막 질환에서 두 수술을 동시에 시행하는 비율이 높아지고 있다.6-8백내장 수술을 하는 경우에는 환자들의 시력 향상에 대한 기대치가 높기 때문에 정확한 인공수정체의 도 수 예측력이 중요하다고 할 수 있다 유리체절제술과 백내장병합 . 수술 후에는 수술 후 전방 깊이의 변화 안축장 길이의 변화 유효, , 렌즈 위치의 변화 유리체의 방수로의 치환으로 인한 매질 변화 , 등 여러 원인에 의해 예측 굴절력의 오차가 발생하는 것으로 알려 져 있다.
정확한 안축장 측정이 인공수정체 도수 계산에서 중요함은 잘 알려져 있다.9,10 A-scan은 각막 표면과 내경계막 사이의 길이를 측정하는데 반해, IOL master의 경우 망막색소상피까지의 길이 를 측정한다 따라서 만일 망막 두께를 증가시킬 수 있는 . 망막앞 막 및 당뇨성 황반 부종 등의 황반 질환에서는 A-scan으로 측정한 경우 안축장이 실제보다 짧게 측정될 수 있다 또한 비접촉식인 . , 와는 달리 에서는 접촉에 의한 각막 함입이 발 IOL master A-scan
생하여 안축장이 더 짧게 측정될 수 있다 이전 연구에서 안축장이 . 에 비해 으로 측정한 경우에 약
IOL master A-scan 0.1- 0.5 mm 짧게 측정된다고 보고하였다.11-13본 연구에서도 A-scan에 의한 안축장 측정값이 IOL master에 비하여 0.19 mm 더 짧게 측정 되었다 (p<0.001). Attas-Fox 등14은 IOL master와 A-scan으 로 정상안 안 당뇨성 황반부종이 있는 안의 안축장을 측정23 , 23 하여 비교하였는데 정상안에서는 두 기기의 측정값 간에 유의한 , 차이가 없었으나 황반부종이 있는 안에서는 안축장이 , A-scan에 서는 23.02 ± 0.97 mm (range, 21.53 - 24.81) IOL master 에서는 23.27 ±0.924 mm (range, 21.9 - 25.13)로 측정되어,
에서 안축장이 더 짧게 측정되었다
A-scan (p<0.001). 하지만 망, 막두께와 두 검사기기간의 안축장 차이 간의 상관관계는 없으며 추후 연구가 더 필요할 것이라고 말하였다. Kov cs á 등5은 수술 전 황반 부종이 있을 때 A-scan으로 측정 시 짧게 측정된 안축장
으로 인해 술후 굴절값이 목표굴절값에 비해 근시 편위되어 나타 난다고 하였다 본 연구에서 특발성 망막앞막에 의해 발생한 . 황반 부종으로 인해 술 전 평균 중심망막두께가 474.79 ± 53.32 μm 로 두꺼웠으며 술 후 굴절값의 평균 예측오차는 , A-scan과 IOL
를 이용한 경우 둘 다 근시편위가 나타났고 을
master , A-scan 이
용했을 때 더 유의하게 근시편위가 많이 나타났다(-0.46 ± 0.47D vs -0.36 ± 0.44D, p=0.045). 이는 중심망막두께가 두꺼울수록
으로 측정한 실제 안축장이 측정값에 비해 길어서 수술
A-scan ,
후 인공수정체에 의한 굴절 교정이 부족 교정되어 근시편위가 나 타나기에, IOL master과 비교하여 더 유의하게 근시편위가 많이 나타났다고 설명할 수 있다.
본 연구의 제한점으로 후향적 연구로서 적은 환자 수를 대상으 로 하였다는 점과 짧은 경과 관찰 기간을 들 수 있다 따라서 향후 . 전향적으로 보다 대규모의 연구를 통해 유리체절제술과 백내장병 합수술에서의 굴절력 이상에 대한 확인이 필요할 것이다 또한 본 . 연구에서는 인공수정체 도수 계산 공식으로 SRK-T만을 사용하 였지만, Holladay나 Hoffer-Q 등의 다른 공식을 사용했을 때에 는 평균예측오차에 다른 영향을 주었을 가능성도 있으며 추후 방, 수 치환으로 인한 유리체절제술 후의 매질 변화를 고려한 공식에 대한 연구도 필요할 것이다.
요약하면 특발성 망막앞막 환자에서 유리체절제술과 백내장, 병합수술은 허용할 만한 수준의 굴절력 오차 범위 내의 결과를 보 였으며, A-scan이 IOL master에 비하여 근시편위정도가 더 크 게 나타났으며 술 후 황반부 부종의 감소정도가 클수록 근시편위, 가 증가하였다 따라서 특발성 망막앞막 환자의 유체절제술과 백. 내장병합수술에서 목표굴절값 설정 시 이러한 점을 고려하여 인 공수정체 도수를 결정하는 것이 좋겠다.
REFERENCES
1. Melberg NS, Thomas MA. Nuclear sclerotic cataract after vitrectomy in patients younger than 50 years of age.
Ophthalmology 1995;102:1466-71.
2. Dugas B, Ouled-Moussa R, Lafontaine PO, Guillaubey A,
A-scan IOL master P Value
Axial length, mm 23.58 ± 0.95 23.77 ± 0.95 <0.001
Intended SE, D -0.03 ± 0.50 -0.13 ± 0.41 0.045
Mean prediction error(ME), D -0.46 ± 0.47 -0.36 ± 0.44 0.045
Mean absolute prediction error(MAE), D 0.53 ± 0.39 0.47 ± 0.32 0.197
SE = spherical equivalent.
Table 3. Comparison of measurements between A-scan and IOL master
Berrod JP, Hubert I, et al. Idiopathic epiretinal macular membrane and cataract extraction: combined versus consecutive surgery. Am J Ophthalmol 2010;149:302-6.
3. Savastano A, Savastano MC, Barca F, Petrarchini F, Mariotti C, Rizzo S. Combining cataract surgery with 25-gauge high-speed pars plana vitrectomy: results from a retrospective study. Ophthalmology 2014;121:
299-304.
4. Demetriades AM, Gottsch JD, Thomsen R, Azab A, Stark WJ, Campochiaro PA, et al. Combined phacoemulsifi- cation, intraocular lens implantation, and vitrectomy for eyes with coexisting cataract and vitreoretinal pathology.
Am J Ophthalmol 2003;135:291-6.
5. Kovacs I, Ferencz M, Nemes J, Somfai G, Salacz G, Recsan Z. Intraocular lens power calculation for combined cataract surgery, vitrectomy and peeling of epiretinal mem- branes for macular oedema. Acta Ophthalmol Scand 2007;85:88-91.
6. Byoung Young G, Md, Min S, Md, Woo Hyok C, Md.
Phacovitrectomy versus Vitrectomy only for Primary Rhegmatogenous Retinal Detachment Repair. J Korean Ophthalmol Soc 2011;52:537-43.
7. Hurley C, Barry P. Combined endocapsular phacoemul- sification, pars plana vitrectomy, and intraocular lens implantation. J Cataract Refract Surg 1996;22:462-6.
8. Chung TY, Chung H, Lee JH. Combined surgery and se- quential surgery comprising phacoemulsification, pars plana vitrectomy, and intraocular lens implantation:
comparison of clinical outcomes. J Cataract Refract Surg 2002;28:2001-5.
9. Norrby S. Sources of error in intraocular lens power calculation. J Cataract Refract Surg 2008;34:368-76.
10. Olsen T. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 1992;18:125-9.
11. Manvikar SR, Allen D, Steel DH. Optical biometry in combined phacovitrectomy. J Cataract Refract Surg 2009;35:64-9.
12. Rose LT, Moshegov CN. Comparison of the Zeiss IOLMaster and applanation A-scan ultrasound: biometry for intraocular lens calculation. Clin Exp Ophthalmol 2003;31:121-4.
13. Haigis W, Lege B, Miller N, Schneider B. Comparison of immersion ultrasound biometry and partial coherence interferometry for intraocular lens calculation accord- ing to Haigis. Graefes Arch Clin Exp Ophthalmol 2000;
238:765-73.
14. Attas-Fox L, Zadok D, Gerber Y, Morad Y, Eting E, Benamou N, et al. Axial length measurement in eyes with diabetic macular edema: a-scan ultrasound versus IOLMaster. Ophthalmology 2007;114:1499-504.