대한안과학회지 2015년 제 56 권 제 3 호 J Korean Ophthalmol Soc 2015;56(3):447-451 ISSN 0378-6471 (Print)⋅ISSN 2092-9374 (Online)
http://dx.doi.org/10.3341/jkos.2015.56.3.447
Case Report
녹색광 레이저 포인터 조사 후 발생한 황반병증 1예
A Case of Maculopathy from Handheld Green Laser Pointer
김영준1⋅정인영1,2⋅김성재1,2⋅박종문1,2⋅한용섭1,2
Young Jun Kim, MD1, In Young Chung, MD, PhD1,2, Seong Jae Kim, MD, PhD1,2, Jong Moon Park, MD, PhD1,2, Yong Seop Han, MD, PhD1,2
경상대학교 의학전문대학원 안과학교실1, 경상대학교 건강과학연구원2
Department of Ophthalmology, Gyeongsang National University School of Medicine1, Jinju, Korea Gyeongsang Institute of Health Science, Gyeongsang National University2, Jinju, Korea
Purpose: To report a case of successfully treated maculopathy after exposure to a handheld green laser pointer beam.
Case summary: A-15-year-old patient visited our clinic complaining of visual disturbance in the left eye 5 days earlier after ex- posure to a handheld laser pointer with 532 nm wavelength green beam for 5 seconds. His best corrected visual acuity was 20/50 in the left eye. On fundus examination, a yellowish retinal scar was observed at the foveal area. The spectral domain opti- cal coherence tomography (SD-OCT) showed cone outer segment tip line and inner segment/outer segment line disruption, ex- ternal limiting membrane line and retinal pigment epithelial complex injury related to laser pointer exposure. We started occlu- sion therapy, oral prednisolone and, antioxidant treatment on his left eye for 2 weeks. The best corrected visual acuity was 20/20 in the left eye at 1 month after treatment. However, spectral domain optical coherence tomography showed a scar remained in the retinal pigment epithelial complex of the macular region of his left eye while the external limiting membrane line was restored and inner segment/outer segment line was partially restored.
Conclusions: Maculopathy can result from exposure to a handheld green laser pointer. Occlusion therapy, oral prednisolone and, antioxidant treatment might be helpful for recovery of visual acuity and restoration of external limiting membrane line.
J Korean Ophthalmol Soc 2015;56(3):447-451
Key Words: Antioxidant, Green laser pointer, Maculopathy, Prednisolone, SD-OCT
■Received: 2014. 11. 8. ■ Revised: 2015. 2. 10.
■Accepted: 2015. 2. 17.
■Address reprint requests to Yong Seop Han, MD, PhD Department of Ophthalmology, Gyeongsang National University Hospital, #79 Gangnam-ro, Jinju 660-702, Korea Tel: 82-55-750-8181, Fax: 82-55-758-4158
E-mail: [email protected]
ⓒ2015 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
빛은 다양한 범주의 전자기파로 구성되어 있으며 기계적, 열적, 광화학적 효과로 안조직에 영향을 줄 수 있으며, 특 히 파장이 짧은 자외선이나 청색 빛이 망막 및 망막색소상 피, 맥락막에 손상을 주는 것으로 알려졌다.1,2 빛에 의한 망 막손상의 예로는 자연광에 의한 손상, 수술 안내 레이저 장 비, 세극등현미경, 광응고 레이저 장비 등이 있으며, 용접광
에 의한 자외선 노출 등에 의해 망막이 손상되는 경우도 보 고되고 있다.1,3
레이저 포인터는 1976년 미국 식품의약품안전청 승인 이 후 전 세계적으로 널리 사용되고 있으며, 특히 최근에는 산 업용 및 교육용으로 사용범위가 넓어지면서 이로 인한 망 막 손상도 보고되고 있다. 특히 파장이 짧은 녹색광 레이저 포인터는 적색광 레이저 포인터보다 원거리 및 야간에 잘 관찰되어 실내외에서 그 사용이 증가되고 있는 추세이다. 최근에는 파장 및 그 강도가 기준치보다 높은 레이저 포인 터로 인한 망막 손상이 보고되고 있으며, 장난감에 사용된 레이저에 의해 망막 손상이 발생한 예도 보고된 바 있으 나,4-6 스펙트럼영역 빛간섭단층촬영기(SD-OCT)를 이용하 여 발생초기부터 병의 경과를 살펴본 증례는 국내에서 보
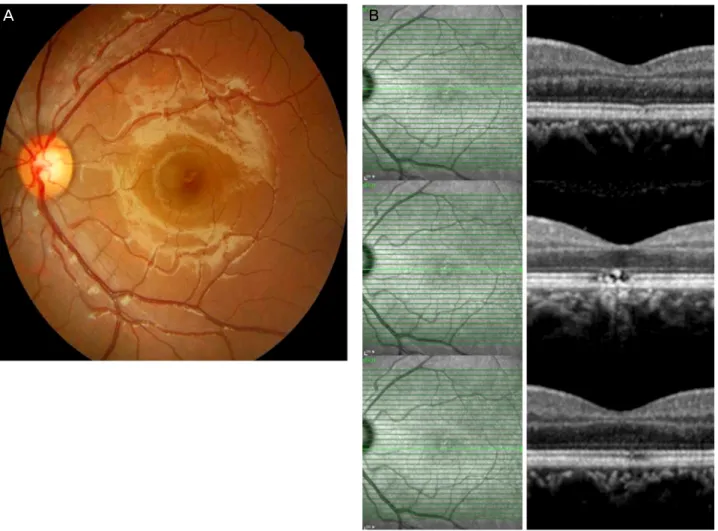
Figure 1. Fundus photograph (A) and SD-OCT (B) at the first ophthalmic examination show yellowish retinal scar at the foveal area
and cone outer segment tip line and inner segment/outer segment line disruption, external limiting membrane line and retinal pig- ment epithelial complex injury in the left eye. SD-OCT = spectral domain optical coherence tomography.고된 바 없다.
저자들은 Class 3A 등급의 녹색광 레이저 포인터에 약 5 초간 좌안 노출 후 발생한 레이저 포인터 황반병증 1예를 경험하였고 초기부터 스펙트럼영역 빛간섭단층촬영기를 이용하여 황반부의 변화를 연속적으로 살펴보았으며 성공 적으로 치험하였기에 이를 보고하고자 한다.
증례보고
15세 남자 환자가 내원 5일 전 532 nm 파장, 최대 출력 5 mW의 녹색광 레이저 포인터를 약 5초 동안 주시한 후 발생한 갑작스런 좌안 시력저하를 주소로 내원하였다. 환 자는 녹색광 레이저 포인터로 좌안에 직접 조사를 하였고 이후 시력이 감소하였다고 했다. 당시 인근 안과에서 진료 를 보았고 망막 중심부 손상 의심되어 정밀검사 및 치료를 위해 본원 외래에 내원하였다.
내원 당시 환자의 최대교정 시력은 우안 20/20, 좌안
20/50였고, 안압은 골드만압평안압계로 우안 19 mmHg, 좌 안 20 mmHg였다. 세극등 현미경 검사상 전안부는 정상이 었으나 안저검사에서 좌안 중심망막 부위에서 황색 변성 및 반흔이 관찰되었고(Fig. 1A), 빛간섭단층촬영에서 좌안 광수용체 내외절 경계가 모호하였으며, 외경계막 및 망막 색소상피층의 손상이 관찰되었다(Fig. 1B).
환자의 병력과 안저소견을 바탕으로 레이저 포인터에 의한 황반병증으로 진단하였고, 빛에 의한 추가적인 손상을 최소화 하기 위해 좌안 가림치료를 시행하였으며, 경구 Prednisolone (Solondo®, Yuhanmedica, Korea) 30 mg, 항산화제(Ocuvite® Bausch & Lomb Surgical, Rochester, USA)를 처방하였다.
3일 뒤 경구 Prednisolone (Solondo®, Yuhanmedica, Korea) 20 mg으로 감량하였으며, 이후 10일에 걸쳐 점차 감량하였다.
치료 14일째, 환자의 좌안 최대 교정시력은 20/25이었고, 안저소견상 큰 변화는 보이지 않았으나(Fig. 2A) 빛간섭단 층촬영에서 황반 중심부 외경계막이 점차 회복되는 모습이 관찰되었다(Fig. 2B). 치료 1개월 후 내원 시, 환자의 좌안
A B
- 김영준 외 : 녹색광레이저포인터 유발 황반병증 1예 -
Figure 2. Fundus photograph (A) and SD-OCT (B) after 2 weeks of treatment show external limiting membrane, inner segment/out-
er segment line were partially restored, but retinal scar at the foveal area and retinal pigment epithelial complex injury persist in the left eye. SD-OCT = spectral domain optical coherence tomography.최대 교정시력은 20/20으로 측정되었으며, 안저검사상 크 기가 감소하였으나 다소 짙어진 황갈색 황반 반흔은 여전 히 관찰되었다(Fig. 3A). 빛간섭단층촬영에서 좌안 외경계 막은 회복되었으나, 광수용체 내외절 경계는 부분적 회복 만 보였고 망막색소상피층의 반흔은 지속되었다(Fig. 3B).
이후 6개월간 재발이나 악화 소견은 관찰되지 않았으며, 최 대 교정시력은 20/20으로 유지되고 있다.
고 찰
레이저는 단색, 단방향, 최소한의 발산을 특징으로 하는 빛을 말하며, 원거리의 좁은 지역에 빛을 조사할 수 있어 사회 전반적으로 다양한 분야에서 널리 이용되고 있다.7 레 이저에 의한 망막 손상의 종류는 크게 4등급으로 나눠진다.
Class 1은 출력이 작아 안손상을 유발하지 않으며 Class 2 는 가시광선의 레이저로 최대 출력이 1 mW이며 0.25초 이 상 주시할 경우 안손상을 유발할 수 있다. Class 3은 최대
출력에 따라 A, B로 나눠지며 A는 최대 출력이 5 mW, B는 500 mW에 해당한다. Class 4는 500 mW 이상의 최대 출력 을 가지는 레이저에 해당하며 군사용, 실험용, 또는 의학적 목적으로 사용되고 있다. 여러 선진국에서 Class 2 이상의 등급의 레이저 포인터는 판매가 제한되고 있으며, 국내에 서도 2004년 이후 Class 2 이상의 레이저 포인터의 판매가 금지되고 있다. 하지만 실제 해당 기준보다 고출력의 레이 저 포인터가 유통되고 있어 이로 인한 황반병증 사례가 점 차 늘고 있다.8
비록 시판되는 레이저 포인터에는 ‘Avoid direct eye ex- posure’나 ‘Please lasers placed where children cannot reach’
등의 경고문이 붙어 있지만 레이저 포인터 사용이 확산되 고 대중화됨에 따라 이로 인한 황반병증이 발생한 사례들이 보고되고 있다. Ham et al9은 Class 3A 등급의 레이저 포인 터를 10초 이상 눈에 조사했을 때 황반병증이 발생함을 동 물실험을 통해 입증한 바 있으며, Robertson et al10은 Class 3A 등급의 적색과 녹색의 레이저포인터를 인위적으로 15분
A B
Figure 3. Fundus photograph (A) and SD-OCT (B) after 1 month of treatment show external limiting membrane was fully restored,
and inner segment/outer segment line was partially restored, but the retinal scar at the foveal area, and retinal pigment epithelial complex injury remain in place. SD-OCT = spectral domain optical coherence tomography.간 조사하였을 때, 적색광의 경우에는 망막 손상이 관찰되 지 않은 반면 녹색광의 경우에서 황반병증이 발생됨을 보 고하였고, Sell and Bryan11 또한 Class 3A 등급의 레이저 포인터에 우안 노출 후 발생한 황반병증을 보고하였다.
본 증례에서 황반병증을 유발한 레이저 포인터는 중국에 서 생산된 제품으로 현재 국내에서 시판 금지된 Class 3A 등급의 녹색광 레이저 포인터였다. 실제 적색광보다는 녹 색광처럼 파장이 짧은 레이저에서 더욱 많은 에너지가 열 에너지로 전환되어 망막 및 맥락막의 구조 단백질의 변성 을 유발하며, 효소 대사과정을 와해시켜 망막 신경계가 손 상을 받는 것으로 알려졌다.2
치료법에 대한 연구로는 Lam et al12은 동물실험을 통해 스테로이드 제제가 망막 및 맥락막 혈관, 망막색소 상피증 의 회복에 도움이 된다고 하였으며, Rosner 쥐를 이용한 실 험에서 스테로이드 제제가 단기간의 호전효과를 보였다고 보고하였다.13 사람에 있어 스테로이드 제제가 망막 손상에 대한 세포면역 반응을 감소시켜 망막 회복에 도움이 된다 는 연구 보고가 있으나 각 연구에 따라 시력 예후의 결과가
다양하게 나타났으며,14,15 항산화제 또한 효과가 있다는 보 고가 있지만 명확한 치료법으로 규명되지는 않았다.16,17,18 또한 손상 당한 눈에 추가적인 빛으로부터 안전성을 확보 하기 위해 가림치료를 시행하는 경우는 일상생활을 제한하 고 환자의 순응도가 떨어진다.9
위와 같이 레이저 포인터에 의한 황반병증의 치료법이 명확히 정립되어 있지 않은 상태여서, 저자들은 빛에 의한 안손상을 최소화하기 위해 가림치료를 시행하였고, 경구 스테로이드 제제, 항산화제 치료를 복합적으로 시행하였으 며 스펙트럼영역 빛간섭단층촬영기를 이용하여 황반부의 변화를 연속적으로 살펴보았다. 다른 증례들에서는 시력예 후가 낮거나 불량한 것으로 보고하였으나, 본 증례에서는 망막색소상피층의 반흔은 지속되지만 광수용체 내외절의 경계가 회복되고 시력이 호전되는 것을 경험하였다. 본 증 례 외에 다른 환자들에서 같은 효과가 나타날지에 대한 추 가적인 고찰 및 연구가 필요할 것으로 생각한다. 뿐만 아니 라 본 증례에서처럼 허용 기준 이상의 고출력 레이저 포인 터가 불법적으로 유통되고 있어 이에 대한 사회적인 엄격
A B
= 국문초록 =
녹색광 레이저 포인터 조사 후 발생한 황반병증 1예
목적: 녹색광 레이저 포인터 조사 후 발생한 황반병증을 경험하였기에 보고하고자 한다.
증례요약: 15세 남자 환자가 5일 전 약 5초 동안 레이저 포인터를 주시한 후 발생한 좌안 시력저하를 주소로 내원하였다. 환자의 좌안 최대 교정시력은 0.4였고 안저검사상 황반 중심오목에 황색의 반흔이 관찰되었으며 스펙트럼영역 빛간섭 단층촬영상 광수용체 내외 절 경계과 광수용체 외절의 손상, 외경계막 및 망막색소상피층의 손상이 관찰되었다. 가림치료, 경구 스테로이드제, 항산화제로 치료 한 이후 환자의 시력은 1.0까지 회복되었다. 안저검사상 황반부 반흔은 지속되었으나, 스펙트럼영역 빛간섭 단층촬영상 외경계막은 회복된 모습이 관찰되었고 광수용체 내외절 경계는 부분적인 회복을 보였다.
결론: 레이저 포인터에 의해 황반병증이 발생한 환자에서 초기부터 스펙트럼영역 빛간섭 단층촬영을 이용하여 경과관찰을 하였으며, 가림치료, 경구 스테로이드제, 항산화제 치료를 통해 시력호전 및 외경계막 회복에 효과가 있었던 증례를 경험하여 보고하는 바이다.
<대한안과학회지 2015;56(3):447-451>
- 김영준 외 : 녹색광레이저포인터 유발 황반병증 1예 -
한 규제와 이들의 사용 시 영구적인 시력 저하 위험성에 대 한 충분한 교육이 필요하리라 생각한다.
결론적으로 녹색광 레이저 포인터에 의한 황반병증으로 진단된 환자에서 초기부터 스펙트럼영역 빛간섭단층촬영 기를 이용하여 경과관찰하였고, 가림치료 및 경구 스테로 이드제제, 항산화제 병합 치료가 시력호전과 광수용체 내 외절 회복에 효과가 있었던 증례를 보고하는 바이다.
REFERENCES
1) Choi SW, Chun KI, Lee SJ, Rah SH. A case of photic retinal injury associated with exposure to plasma arc welding. Korean J Ophthalmol 2006;20:250-3.
2) Ryan SJ. Retina, 5th ed. Vol. 2. Los Angeles: Elsevier Mosby, 2013;1555-8.
3) Jeong WD, Hwang YH, Kim JS, Lee JH. Maculopathy from red la- ser pointer. J Korean Ophthalmol Soc 2007;48:1007-11.
4) Robertson DM, McLaren JW, Salomao DR, Link TP. Retinopathy from a green laser pointer: a clinicopathologic study. Arch Ophthalmol 2005;123:629-33.
5) Kim Martha, Kwon JW, Han YK. A case of green laser pointer in- jury to the macula. J Korean Ophthalmol Soc 2008;49:681-4.
6) Raoof N, Chan TK, Rogers NK, et al. 'Toy' laser macular burns in children. Eye (Lond) 2014;28:231-4.
7) Barkana Y, Belkin M. Laser eye injuries. Surv Ophthalmology 2000;44:459-78.
8) Schulmeister K, Jean M. The risk of retinal injury from Class 2 and visible Class 3R lasers, including medical laser aiming beams.
Medical Laser Application 2010;25:99-110.
9) Ham WT Jr, Geeraets WJ, Mueller HA, et al. Retinal burn thresh- olds for the helium-neon laser in the rhesus monkey. Arch Ophthalmol 1970;84:797-809.
10) Robertson DM, McLaren JW, Salomao DR, Link TP. Retinopathy from a green laser pointer: a clinicopathologic study. Arch Ophthalmol 2005;123:629-33.
11) Sell CH, Bryan JS. Maculopathy from handheld diode laser pointer. Arch Ophthalmol 1999;117:1557-8.
12) Lam TT, Takahashi K, Fu J, Tso MO. Methylprednisolone therapy in laser injury of the retina. Graefes Arch Clin Exp Ophthalmol 1993;231:729-36.
13) Rosner M, Solberg Y, Turetz J, Belkin M. Neuroprotective therapy for argon-laser induced retinal injury. Exp Eye Res 1997;65:
485-95.
14) Hirsch DR, Booth DG, Schocket S, Sliney DH. Recovery from pulsed-dye laser retinal injury. Arch Ophthalmol 1992;110:1688-9.
15) Zwick H, Stuck BE, Dunlap W, et al. Accidental bilateral Q-switch- ed neodymium laser exposure: treatment and recovery of visual function. In BiOS'98 International Biomedical Optics Symposium.
International Society for Optics and Photonics 1998;3254:80-89.
16) Cai YS, Xu D, Mo X. Clinical, pathological and photochemical studies of laser injury of the retina. Health Phys 1989;56:643-6.
17) Lam TT, Tso MO. Retinal injury by neodymium: YAG laser. Retina 1996;16:42-6.
18) Liu HF, Gao GH, Wu DC, et al. Ocular injuries from accidental la- ser exposure. Health Phys 1989;56:711-6.