36
• 교신저자:허정식, 제주대학교병원 비뇨기과 제주 제주시 아라 1동 번지 우 130-702
Tel: 064-717-1760, Fax: 064-717-1234, E-mail: [email protected] Received: February 29, 2012
Revised: March 1, 2012 Accepted: March 23, 2012
*이 연구는 제주대학교병원 연구비로 수행되었습니다.
경직장초음파하 전립선조직검사 후 발생한 발열을 동반한 요로감염의 위험인자
제주대학교 의학전문대학원 가정의학교실,
1비뇨기과학교실
김현주∙김영주
1∙허정식
1[Abstract]
The Risk Factors of Urinary Tract Infection with Fever after Transrectal Ultrasonography Guided Biopsy of Prostate
Hyeon Ju Kim, Young-Joo Kim
1, Jung-Sik Huh
1From the Department of Family Medicine, and 1Urology, School of Medicine, Jeju National University, Jeju, Korea
Purpose: Recently, incidence of prostatic cancer has increased due to the development of the prostatic
cancer screening test. The common procedure is the transrectal technique, whereby following prophylactic antibiotics, a core biopsy needle is passed through the rectum. Complications of prostate biopsy are peri- neal tenderness, hematuria, hematospermia, rectal bleeding, fever and sepsis. We estimated the risk factors and pathogens of urinary tract infections after transrectal ultrasound guided biopsy of prostate.
Materials and Methods: A retrospective chart review was conducted of patients, who had been treated
for urinary tract infection (UTI) after 365 prostatic biopsy between January 2009 and January 2012. We analyzed the parameters including past medical history, kind of antibiotics, number of biopsies, pathology, urine culture and blood culture.
Results: Hematuria was most common (5.4%), while UTI occurred in 4.9% of the cases. The symptoms
of UTI were dysuria and fever. Average admission day was 6.2 days. E. coli was identified in 7 patients.
It was observed that higher numbers of biopsies correlated with UTI. The other conditions investigated
didn't correlate with complications after biopsies.
Conclusions: We considered that UTI was a rare complication of prostatic biopsy and complications af-
ter biopsy were low. A higher number of fragments taken during biopsies showed a correlation with UTI.
(Korean J UTII 2012;7:36-42)
Key Words: Prostate, Urinary tract infection, Risk factors
서 론
전립선암의 유병율과 이로 인한 사망률은 미국 뿐만 아니라 선진국에서 연령의 증가와 전립선암 의 선별검사인 혈청 전립선특이항원 (prostate-spe- cific antigen: PSA)의 발견으로 인해 점차 증가하는 추세이며 미국에서 2010년에 220,000명이 전립선암 으로 새롭게 진단되고 30,000명 이상이 이 질환으 로 인해 사망하고 있다.
1우리나라에서 평균여명의 증가와 서구식 생활환경과 진단기술의 발달, 전립 선암에 대한 초기 진단을 위한 노력으로 인한 전립 선암이 증가하는 추세이다.
2직장을 통한 전립선의 조직검사는 전립선암을 진단하는 방법으로 비교적 안전한 방법으로 알려져 있다. 이 검사는 연령에 따른 전립선특이항원의 증가 혹은 직장수지검사에 서 전립선에 결절이 만져지거나 경직장초음파하에 저음영의 병변을 발견하는 경우에 시행하고 있다.
3전립선조직검사를 하는 방법은 회음부를 이용한 조직검사 혹은 직장을 통한 조직검사를 시행하고 있으며 두 방법의 진단율이나 합병증에는 별다른 차이를 보이지 않는다.
4,5다양하게 나타나는 합병 증을 줄이기 위해 여러 가지 시술 전 처치와 시술 후 처방 등 아직 표준화된 방법은 있지 않지만 일 반적으로 전립선조직검사를 위해 6시간 이상 금식 을 하며 검사 1-3시간 전에 quinolone 항생제를 경 구로 투약을 투약하거나, 검사 직전 정주로 quino- lone 항생제를 사용하기도 한다. 장에 대한 전 처치 로 아침에 배변을 하지 못한 경우에는 관장을 하기 도 한다.
6,7전립선조직검사는 침습적인 방법이며 이로 인해 발생되는 주요 합병증으로는 패혈증을 포함한 요로감염, 급성요폐, 입원을 요하는 직장출 혈 등이 있으며 별다른 치료가 필요없는 혈뇨와 단
순한 압박을 통해 지혈이 되는 직장출혈, 혈정액증 등이 발생하기도 한다.
6,8,9이러한 합병증 중 요로감 염은 무증상의 농뇨에서부터 단순한 감염, 열을 동 반한 패혈증 혹은 쇼크를 일으키는 경우가 있다.
이에 저자들은 이러한 경직장초음파하에 전립선조 직검사를 시행할 때 발생하는 합병증의 종류와 발 생률을 알아보고, 아울러 요로감염과 관련된 위험 인자를 알아보고자 하였다.
대상 및 방법
2009년 1월부터 2012년 1월까지 빈뇨 혹은 야간 빈뇨, 요주저 등의 배뇨증상으로 본원 외래를 방문 하거나 본원의 건강검진 혹은 개인병원에서 우연 하게 검사한 전립선특이항원 검사에서 연령특이 전립선특이항원의 참고치보다 증가되었거나 전립 선직장검사에서 경결이 촉지되거나 경직장초음파 검사에서 저음영의 병변이 발견된 365명의 환자를 대상으로 경직장초음파하에 전립선조직검사를 실 시하였다. 이들의 평균연령은 68.2세 (32-92세)였으 며 전립선특이항원은 0.29-419.7로 평균치는 20.5 ng/ml였다. 전립선의 크기는 18-170cc로 평균부피는 37.7cc였다 (Table 1). 이들 환자 중 아스피린 혹은 항응고제를 복용하는 경우에는 약 1주간 복용을 중 단하였고 전립선조직검사를 하는 당일 6시간 이상 금식을 하였으며, 대변을 보지 않은 경우에는 관장 을 오전에 실시한 이후 조직검사를 오후에 실시하 였다. 조직검사 전 중간요검사, 일반혈액검사를 실 시하여 이상이 없는 경우에만 조직검사를 하였다.
경직장초음파하에 전립선조직검사를 받은 환자에
서 전립선조직검사 전 항생제 처치로는 술자에 따
라 차이는 있으며 시술 3시간 전에 quinolone제제인
ciprofloxacin 250mg을 경구 투여하거나 시술 직전
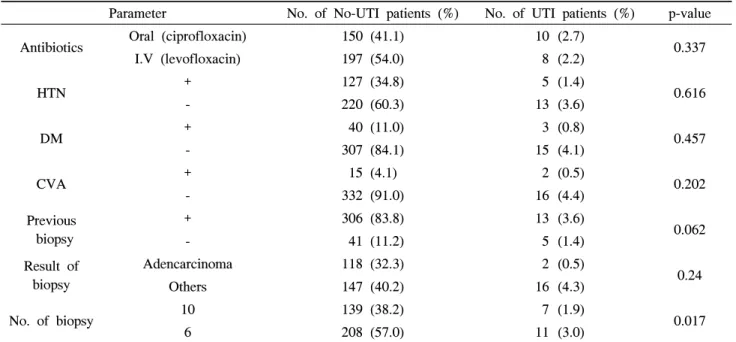
Table 3. Risk factors for prostatic biopsy
Parameter No. of No-UTI patients (%) No. of UTI patients (%) p-value
Antibiotics Oral (ciprofloxacin) 150 (41.1) 10 (2.7)
0.337
I.V (levofloxacin) 197 (54.0) 8 (2.2)
HTN + 127 (34.8) 5 (1.4)
0.616
- 220 (60.3) 13 (3.6)
DM + 40 (11.0) 3 (0.8)
0.457
- 307 (84.1) 15 (4.1)
CVA + 15 (4.1) 2 (0.5)
0.202
- 332 (91.0) 16 (4.4)
Previous biopsy
+ 306 (83.8) 13 (3.6)
0.062
- 41 (11.2) 5 (1.4)
Result of biopsy
Adencarcinoma 118 (32.3) 2 (0.5)
Others 147 (40.2) 16 (4.3) 0.24
No. of biopsy 10 139 (38.2) 7 (1.9)
0.017
6 208 (57.0) 11 (3.0)
UTI: urinary tract infection, HTN: hypertension, DM: diatbetes mellitus, CVA: cardiovascular accident, I.V: intravenous +: presence, -: absence
Table 1. Clinical characteristics of patients undergoing prostatic biopsy
Range Mean±SD
Age (years) 32-92 68.2±9.2
PSA (ng/ml) 0.29-419.7 20.5±48.2
Volume of prostate (cc) 18-170 37.7±18.8 SD: standard deviation
Table 2. Incidence of adverse events of prostatic biopsy Complications No. of patients (%)
Gross hematuria 20 (54.8)
Acute urinary retention 5 (1.3) Urinary tract infection 18 (4.9)
Rectal bleeding 11 (3.0)
Hematospermia 1 (0.2)
Total 55 (100)
levofloxacin을 정주로 하였으며, 조직검사 시에 베 타딘으로 회음부를 광범위하게 소독한 이후 직장 안을 깨끗이 소독하였다. 초음파는 7.5 MHz 양면 탐침을 이용하였으며 일회용조직검사침을 이용하 였다. 전립선조직은 전립선의 양측 소엽의 첨부, 중 간부, 기저부에서 각각 조직검사를 하는 체계적인 전립선육분의 생검을 하였고 초음파에서 이상소견 이나 결절이 만져지는 곳에 추가로 확대생검을 실 시하였다. 조직검사 중 항문 출혈이 심한 경우에는 조직검사를 더 이상 시행하지 않았다. 시술 후 직 장출혈, 발열, 배뇨장애 등 다른 합병증이 없는 경 우에 입원 다음날에 퇴원을 하였다.
결 과
전립선조직검사 이후 합병증으로는 육안적 혈뇨 가 20명이었지만 특별한 조치없이 자연적으로 모 두 호전되었다. 급성요폐는 5명으로 도뇨관을 약 7 일간 삽입하였으며 1명에서는 조직검사 이후 암이 발견되지 않아 내시경적 전립선절제술을 받았다.
직장출혈은 11명으로 조직검사 직후 발견되어 수
지압박을 통한 지혈로 출혈이 멈추었으며 수혈을
한 경우는 발생하지 않았다. 혈정액증은 1명에서
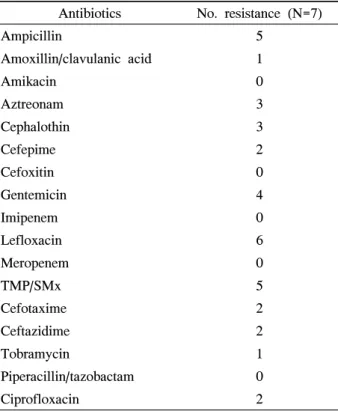
Table 4. Antibiotics resistance of E. coli
Antibiotics No. resistance (N=7)
Ampicillin 5
Amoxillin/clavulanic acid 1
Amikacin 0
Aztreonam 3
Cephalothin 3
Cefepime 2
Cefoxitin 0
Gentemicin 4
Imipenem 0
Lefloxacin 6
Meropenem 0
TMP/SMx 5
Cefotaxime 2
Ceftazidime 2
Tobramycin 1
Piperacillin/tazobactam 0
Ciprofloxacin 2