182
•교신저자:이길호, 단국대학교 의과대학 비뇨기과학 교실 충남 천안시 동남구 망향로 359 우 330-715 Tel: 041-330-715, Fax: 041-556-0524 E-mail: [email protected]
Received: September 7, 2010 Accepted: October 4, 2010
여성 성매매자들에 있어서 Mycoplasma genitalium 및 Ureaplasma urealyticum 검출
단국대학교 의과대학 비뇨기과학교실
이길호∙박희윤[Abstract]
Detection of Mycoplasma genitalium and Ureaplasma urealyticum Infection in Female Commercial Sex Workers
Gilho Lee, Hee Yoon Park
From the Department of Urology, Dankook University College of Medicine, Cheonan, Korea
Purpose: To detect Ureaplasma urealyticum (U. urealyticum) and Mycoplasma genitalium (M.
genitalium) infections in female commercial sex workers (FCSW) in Korea.
Materials and Methods: Total 127 samples from FCSWs were randomly collected. Endo-cervical swab
was obtained and DNA was extracted from the samples. Gene amplification was performed with specific primers for U. urealyticum and M. genitalium from the patients’ DNA.
Results: Of the 127 samples, 49 samples were positive by amplification of U. urealyticum and 7 samples were positive by amplification of M. genitalium. In this study, the prevalence of U. urealyticum and M. genitalium in FCSW were 38.5% and 5.51%, respectively.
Conclusions: Detection of U. urealyticum was relatively high, whereas detection of M. genitalium was
relatively low in FCSW in Korea. Further studies should be performed to characterize the mycoplasma infections in sexually transmitted infectious core groups. (Korean J UTII 2010;5:182-187)
Key Words: Ureaplasma urealyticum, Mycoplasma genitalium, Sex
서 론
성 전파성 감염증으로 70년대 중반까지 증가하던 임
균성 요도염의 빈도는 그 후 감소하는 반면, 비임균성
요도염의 빈도는 점차 증가하고 있다.
1,2과거에는 요도
염을 유발하는 균을 주로 배양법으로 분류하여 임균이
자라면 임균성 요도염, 증상이 있지만 임균이 자라지
않으면 비임균성 요도염으로 분류하고 치료하였다. 하
지만 근 20년 동안 유전자 증폭법 및 염기서열 분석법
을 이용하거나, 과거에 잘 배양되지 않았던 균을 배양
할 수 있는 기술이 개발되어 임균성 요도염, Chlamydia
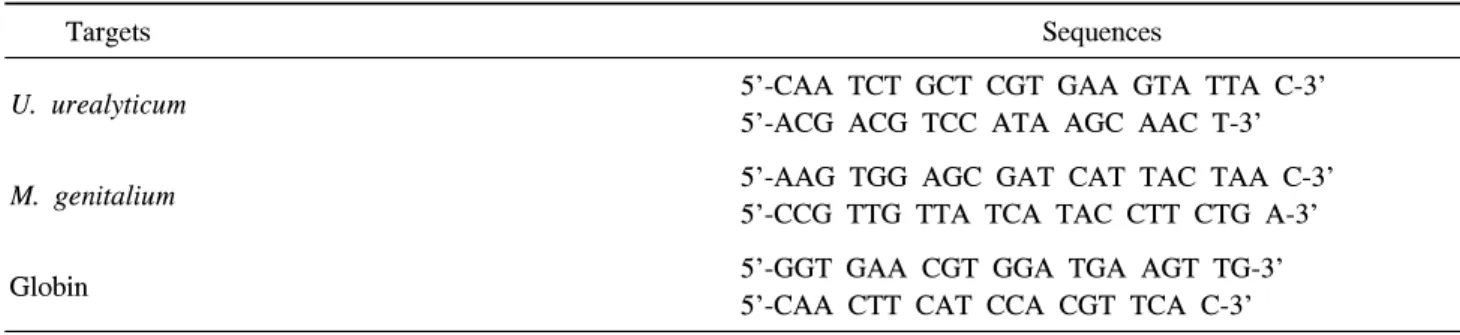
trachomatis (C. trachomatis)에 의한 요도염, 그리고 그Table 1. Primers for amplifications
Targets Sequences
U. urealyticum 5'-CAA TCT GCT CGT GAA GTA TTA C-3'
5'-ACG ACG TCC ATA AGC AAC T-3'
M. genitalium 5'-AAG TGG AGC GAT CAT TAC TAA C-3'
5'-CCG TTG TTA TCA TAC CTT CTG A-3'
Globin 5'-GGT GAA CGT GGA TGA AGT TG-3'
5'-CAA CTT CAT CCA CGT TCA C-3'
외 비임균 및 비 C. trachomatis 요도염으로 분류하고
있다. 이러한 분류에 의하면 과거에는 C. trachomatis 감 염 빈도가 30∼50%까지 보고되었으나
1-4최근에는 15%
정도로 낮게 보고되고 있다.
5비임균 및 비 C.
trachomatis
감염균은 Ureaplasma
urealyticum(U.
urealyticum), Mycoplasma hominis
(M.
hominis), Mycoplasma genitalium (M. genitalium), cryptic organism등이 원인균으로 보고되고 있다.
6하지만 U. urealyticum 는 건강인의 비뇨생식기에서 분리되기도 하고 경우에 따라서는 요도염, 전립선염 및 부고환염 뿐만 아니라 그 합병증으로 불임의 원인균으로도 알려져 있다.
6-8성 매개 전파질환으로 분류하기 위해서는 성교를 통해 감 염균이 전파하여야 하는데 여성에서 Mycoplasma 속 (species)이 병을 유발하는 감염균인지 (pathogenic bacteria) 아니면 무해한 균인지 아직 잘 정립되어져 있 지 않다.
6-8이에 저자들은 성매개 질환의 높은 위험군 인 여성 성매매자를 대상으로 유전자 증폭법을 이용하 여 U. urealyticum 과 M. genitalium의 유병률을 조사하 여 Mycoplasma 감염의 임상적 의미를 추정하고자 한다.
대상 및 방법
1. 대상
2004년 4월부터 8월까지 약 5개월에 걸쳐 경기도 에 있는 1개 보건소에서 주기적인 건강검진을 받기 위해 모인 여성 성매자 410명 중 유전자 증폭법으로 임균과 C. trachomatis 감염이 없었던 환자 중 무작 위로 선택된 127명을 대상으로 하였다. 대상군의 평 균연령은 26±7세 였다.
2. 검체에서 DNA 추출
Phosphate-buffered saline (PBS, 8g NaCl, 0.2g KCl, 1.44g Na2HP04, 0.24g KH2PO4, pH 7.4)을 적신 면봉 을 자궁경부 안쪽에 넣어 상피세포를 얻어 미리 냉 장 보관된 1ml의 PBS 용액이 들어있는 소독된 1.5ml 관에 보관하였다. 여러 번 vortexing을 시행한 후 면 봉은 버리고 13,000 xg로 원심분리한 후 상층액은 버 린 후 다시 PBS 용액으로 다시 한 번 반복하여 수 세, 원심분리 후 상층액을 버리고 침전물을 남아있는 PBS 용액으로 부유시켰다. Wizard genomic DNA purification kit (Promega, USA)를 이용하여 genomic DNA를 추출한 후 TE buffer (DNA rehydration buffer) 로 용해시킨 후 -20℃에 냉장 보관하였다.
93. 중합효소연쇄반응
(polymerase chain reaction)
시동염기서열은 바이오니아 (대전, 대한민국)에
의뢰하여 제작하였으며 그 순도는 MALDI-TOF로
확인하였다. Housekeeping 유전자는 beta-globin으로
하였으며 이를 바이오니아에 제작 의뢰하였다
(Table 1). 모든 증폭 혼합물은 master 혼합물을 만
들어 24µl씩 분주하였으며 위에 추출한 주형 1µl를
혼합하여 증폭하였다. Master 혼합물 24µl 안에는
Taq polymerase 1 unit (Promega, USA), 10배
Solution B (20mM Tris-HCl 100mM KCl, 0.1mM
EDTA, 1mM DTT, 50% glycerol, 0.5% Tween 20,
0.5% Nonidet-P40) 2.5µl를 사용하였다. dNTP 혼합
Fig. 1. Polymerase chain reaction results of Ureaplasma urealyticum in patient samples. M; 100bp DNA ladder marker, S1,2,3,4 were from patients samples. N1 was from negative control. S1, 2, 3 showed positive bands.
M N P
Fig. 2. Polymerase chain reaction results of Mycoplasma genitalium in patient samples. M; 100bp DNA ladder marker. P and N were from patients samples. N showed negative result and P showed a positive band.
물 (Promega, USA) 200µM, MgCl
2(1.5mM), 시동염 기서열 앞, 뒤 방향으로 각각 25pmole로 총 25µl로 만들었다. 유전자증폭기는 GeneAmp 9700 (Applied Biosystems, USA)를 사용하였으며 첫 회 증폭 조건 은 94℃에 4분, 94℃에 30초, 55℃에 30초, 72℃에 30초로 25회 증폭하였으며 72℃에 4분 연장하였다.
House keeping 유전자인 beta-globin의 증폭은 상기 같은 조건의 master 혼합물을 만들고, 증폭조건은 94℃에 4분, 94℃에 30초, 53℃ 30초, 72℃에 1분 50초로 30회 증폭하였으며 72℃에 4분 연장하였다.
증폭한 DNA 5µl를 1.5% agarose gel (Promega, USA)에 0.5배 희석 TBE buffer (1M Tris, 1M boric acid, 20mM EDTA, pH 8.3)를 이용하여 100V 전압 으로 45분 동안 이동시켰다. Ethidium bromide (Sigma, USA)로 1시간 염색한 후 30분간 증류수로 수세를 시키고 사진을 얻었다 (Fig. 1, 2).
결 과
127명의 모든 검체에서 housekeeper 유전자의 일 종인 beta-globin이 검출되어 Mycoplasma 증폭에 적 당한 검체임을 알 수 있다. 127명 중 49명 (38.5%)에 서 U. urealyticum이 증폭 되었으며, 127명 중 7명 (5.51%)에서 M. genitalium에 양성이었다. 그러나 U.
urealytium과 M. genitalium이 동시에 검출된 여성은
없었다.
고 찰
1898년 Nocard와 Roux
6가 가축으로부터 처음 mycoplasmas 분리하였으며, 사람에 있어서는 Dienes 와 Edsall
10가 Bartholin 선 농양 환자로부터 처음 분 리한 이후로 다양한 Mycoplasma가 분리 보고되었다.
유전자 증폭법 (polymerase chain reaction)과 염기서 열 분석법 (sequencing and clustering)으로 분류한
Mycoplasma는 현재까지 약 100종 이상의 균이 존재함이 확인되었으며, 사람에서는 총 15종이 보고되어 있으며 그 중 9종이 비뇨생식기에서 발견된다. 요로 생식기에서 검출되는 Mycoplasma는 U. urealyuticum,
M. hominis, M. genitalium이 비교적 흔하게 검출되고있으며, M. fermentans, M. penetrans, M. pneumoniae,
M. primatum, M. spermatophilum 등이 비교적 드물게검출되고 있다. 이 중 U. urealyticum은 다양하게 분화 하여 biovar 1 및 2로 분류되고 그 안에는 약 14개의 다양한 serovars가 보고되고 있다.
6,11Mycoplasma는 Mollicutes 계통 세균으로 그 크기는 1um 이하로 매우 작고, 구성하는 핵산의 크기는 0.58
∼1.38 megabases (MB)로 매우 간편하여 생존하기 위
해서는 진핵세포에 기생하고, 진핵 세포에서 일정한
영양분을 제공 받아야 생존 가능한 세균이다. 또한
특이하게 세포벽이 없고 진핵세포의 콜레스테롤로 부터 얻어진 풍부한 sterol로 구성된 세포막을 가지 고 있어 β-lactam계 항생제에 약제내성을 지니고 있 다.
6,12 Mycoplasma에 의한 인체 감염을 이해하기 위해서는 기본적으로 Mycoplasma의 병인을 이해하여 야 한다. 전술한 것과 같이 Mycoplasma는 크기가 작 고, 단백질을 합성할 수 있는 DNA의 량이 적어 생 존을 위한 모든 영양분을 자신이 합성하여 사용할 수 없어, 필수 영양분을 숙주 세포로부터 얻어 사용 하여야 하고 숙주 세포가 죽으면 자신도 생존할 수 가 없다. 또한 독립적이고 튼튼한 세포벽이 없어 주 위 환경의 변화나 삼투압의 변화 등이 발생하면 생 존할 수가 없다. 하지만 숙주 세포 안으로 들어가 성공적인 생존을 위한 교두보가 마련된다면
Mycoplasma는 마치 공생 (symbiosis)과 비슷하게 숙주 세포를 죽이지 않고 장기간에 영양분을 제공받는
다.
6,11-14그러한 이유로 특히 U. urealyticum와 M.
hominis는 비교적 병원성이 약하며 발병에는 숙주의
요인이나 환경적 요인이 크게 작용하며, 감염된 환 자 뿐만 아니라 건강인에서도 분리되고 있으므로 병 원성에 관해서는 불분명한 점이 많다. 하지만 증상 이 있는 환자에서 증상이 없는 사람에 비해 많은 수 의 Mycoplasma가 비뇨생식기에서 검출된다. 또한 병 원균이 존재할 수 없는 태반이나 양수막 등에서 발 견되며 이러한 균 존재는 산모나 태아에게 해가 될 수 있다. 그리고 역학적으로 성교를 시작하기 시작 하는 사춘기부터 Mycoplasma 감염률이 증가하는 동 시에 임질이나 C. trachomatis 감염이 있는 환자에서
Mycoplasma의 감염률이 높다. 이러한 상기 사실들을고려한다면 일부 Mycoplasma나 환자의 상태에 따라 병원성이 있을 것으로 추정된다.
15-17지금까지 보고된 논문에 의하면 Mycoplasma는 다 양한 질환들을 일으키는데 남성에서는 요도염, 전립 선염, 부고환염 등과 그 합병증으로 불임 등의 비뇨 생식기 질환이 보고되고 있으며, 여성에서는 Bartholin 선 농양, 골반염, 습관성 유산 및 사산, 조기 분만으로 인한 저체중아 등이 보고되고 있다.
15-18전 술한 것과 같이 Mycoplasma는 숙주세포가 없으면 생 존할 수가 없어 배양을 위해서는 영양분을 공급하는 vero-cell (kidney epithelial cells from African green
monkey)같은 공급세포 (feeder cell)가 필요하다. 이러 한 공급세포에서도 느린 대사를 하기 때문에 성공적 인 배양을 위해서는 수개월 혹은 1∼2년이 걸리기도 한다. 또한 크기가 1um 이하로 작기 때문에 배양해서 형태학적으로 진단하는 것은 매우 어렵다. 이러한 단 점을 극복하기 위해, 최근에 개발된 유전자 증폭법이 나 일부 Mycoplasma 핵산과 교잡할 수 있는 탐침자 를 이용하거나 효소면역검사법 등이 개발되었다.
19,21특히 최근 연구와 진단목적으로 많이 쓰이는 유전자 증폭법은 Mycoplasma 속의 동정에 있어 배양방법과 비교하면, 84∼89%의 민감도와 95∼98%의 특이도를 나타내고, 24시간이내에 빠른 결과를 내고, 유전자의 염기서열을 분석하여 아형 구별을 할 수 있어 많이 사용되고 있다.
19,20저자가 증폭한 염기서열은 MgPa 유전자로 이는 M. genitalium이 성공적인 숙주세포 침 투를 위한 부착 단백질 (adhesion protein)을 만드는 유전자로 M. genitalium 종에 일치하는 유전자 염기서 열을 가진다. 또한 U. urealyticum을 진단하기 위해 사 용된 염기서열은 urease을 만드는 핵산으로 U.
urealyticum이 공통적으로 가지고 있는 염기서열이
다.
6,11,12Mycoplasma 검출은 성별 및 연령에 따라, 검
출장소에 따라 다양하게 보고되고 있다. 즉 Furr 등
22은 젊은 연령군에서 더 많이 Mycoplasma가 검출되었 으며, U. urealyticum이 M. hominis보다는 약 4배 이상 더 많은 빈도를 나타냈다고 보고하였다. 하지만 저자 의 연구에서는 U. urealyticum이 M. hominis 보다 약 7 배 많았다. 이러한 차이는 연구 대상의 차이, 즉 성매 개질환의 전파에 중요한 역할을 할 것으로 추정되는 여성 성매매자의 특징이라고 생각할 수 있으나 본 연 구의 대상군이 작다는 것도 고려하여야 할 것이다.
또한 저자의 연구에서 대상군의 특수성을 고려한다
면 U, urealyticum의 빈도는 38.5%로 다른 집단과 비
교하여 높지 않았다. 생각할 수 있는 이유로 본 연구
의 대상군은 모두 임질이나 C. trachomatis의 감염된
사람은 제외하고 비임균성-비 클라미디아 표본만을
대상으로 하였다는 점이다. 전술한 것과 같이
Mycoplasma의 감염은 임질이나 클라미디아 감염과혼합감염이 많은 점을 고려하면 실제로는 알려진 감
염자 수는 높게 밝혀질 것으로 생각한다.
결 론
상기 결과로 1개지역의 여성 성매매자들의 U.
urealyticum의 중합효소연쇄반응 양성률은 38.5%, M.
genitalium은 5.51% 정도로 나타났다. 향후 임상적
의미를 평가하기 위해서는 검사결과와 임상증상과 의 관련성 등에 대한 조사가 지속적으로 필요할 것 으로 생각한다.
REFERENCES
1. Groseclose SL, Zaidi AA, DeLisle SJ, Levine WC, St Louis ME. Estimated incidence and prevalence of gen- ital Chlamydia trachomatis infections in the United States, 1996. Sex Transm Dis 1999;26:339-44
2. Stamm WE. Chlamydia trachomatis infections of the adult. In: Holmes KK, Sparling PF, Mardh P, Lemon SM, Stamm WE, Piot P, editors. Sexually transmitted diseases. 3rd ed. New York: McGraw-Hill; 1999;407-22 3. Munday PE, Thomas BJ, Johnson AP, Altman DG,
Robinson DT. Clinical and microbiological study of non-gonococcal urethritis with particular reference to non-chlamydial disease. Br J Vener Dis 1981;57:327-33 4. Bowie WR. Urethritis in male. In: Holmes KK, Mardh
PA, Sparling PF, Wiesner PJ, editors. Sexually trans- mitted disease. 2nd eds. New York: McGraw-Hill;
1989;627-39
5. Stamm WE, Hicks CB, Martin DH, Leone P, Hook EW 3rd, Cooper RH, et al. Azithromycin for empirical treatment of the nongonococcal urethritis syndrome in men. A randomized double-blind study. JAMA 1995;274:545-9
6. Razin S, Yogev D, Naot Y. Molecular biology and pathogenicity of mycoplasmas. Microbiol Mol Biol Rev 1998;62:1094-156
7. Ingham HR, MacFarlane WV, Hale JH, Selkon JB, Codd AA. Controlled study of the prevalence of T strain mycoplasmata in male with non-gonococcal urethritis. Br J Vener Dis 1966;42:269-71
8. Jensen JS. Mycoplasma genitalium: the aetiological agent of urethritis and other sexually transmitted diseases. J Eur Acad Dermatol Venereol 2004;18:1-11
9. Lee GH, Sohng IH. Cryptic Plasmid Amplification of Chlamydia trachomatis at a Korean Health Center for Female Commercial Sex Workers. Korean J Urol 2006;47:37-41
10. Dienes L, Edsall G. Observation on the L-orgarnism of Klineberger. Proc Soc Exp Biol Med 1937;36:740-4 11. Johansson KE, Pettersson B. Taxonomy of Mollicutes.
In: Razin S, Herrmann R, editors. Molecular Biology and Pathogenicity of Mycoplasmas. New York: Kluwer Academic/Plenum; 2002;1-30
12. Fraser CM, Gocayne JD, White O, Adams MD, Clayton RA, Fleischmann RD, et al. The minimal gene complement of Mycoplasma genitalium. Science 1995;270:397-403
13. Razin S, Hayflick L. Highlights of mycoplasma re- search-an historical perspective. Biologicals 2010;38:183-90 14. Rosengarten R, Citti C, Glew M, Lischewski A,
Droesse M, Much P, et al. Host-pathogen interactions in mycoplasma pathogenesis: virulence and survival strategies of minimalist prokaryotes. Int J Med Microbiol 2000;290:15-25
15. Taylor-Robinson D, McCormack WM. The genital mycoplasmas (first of two parts). N Engl J Med 1980;302:1003-10
16. Taylor-Robinson D. Genital mycoplasma infections.
Clin Lab Med 1989;9:501-23
17. Kafetzis DA, Skevaki CL, Skouteri V, Gavrili S, Peppa K, Kostalos C, et al. Maternal genital colonization with Ureaplasma urealyticum promotes preterm delivery: as- sociation of the respiratory colonization of premature infants with chronic lung disease and increased mortality. Clin Infect Dis 2004;39:1113-22
18. Couldwell DL, Gidding HF, Freedman EV, McKechnie ML, Biggs K, Sintchenko V, et al. Ureaplasma ure- alyticum is significantly associated with non-gon- ococcal urethritis in heterosexual Sydney men. Int J STD AIDS 2010;21:337-41
19. Hartmann M. Genital mycoplasmas. J Dtsch Dermatol Ges 2009;7:371-7
20. Maeda S, Deguchi T, Ishiko H, Matsumoto T, Naito S, Kumon H, et al. Detection of Mycoplasma geni- talium, Mycoplasma hominis, Ureaplasma parvum (biovar 1) and Ureaplasma urealyticum (biovar 2) in patients with non-gonococcal urethritis using polymer- ase chain reaction-microtiter plate hybridization. Int J
Urol 2004;11:750-4
21. Furr PM, Taylor-Robinson D. Microimmunofluorescence technique for detection of antibody to Mycoplasma genitalium. J Clin Pathol 1984;37:1072-4
22. Furr PM, Taylor-Robinson D. Prevalence and sig- nificance of Mycoplasma hominis and Ureaplasma ure- alyticum in the urines of a non-venereal disease population. Epidemiol Infect 1987;98:353-9