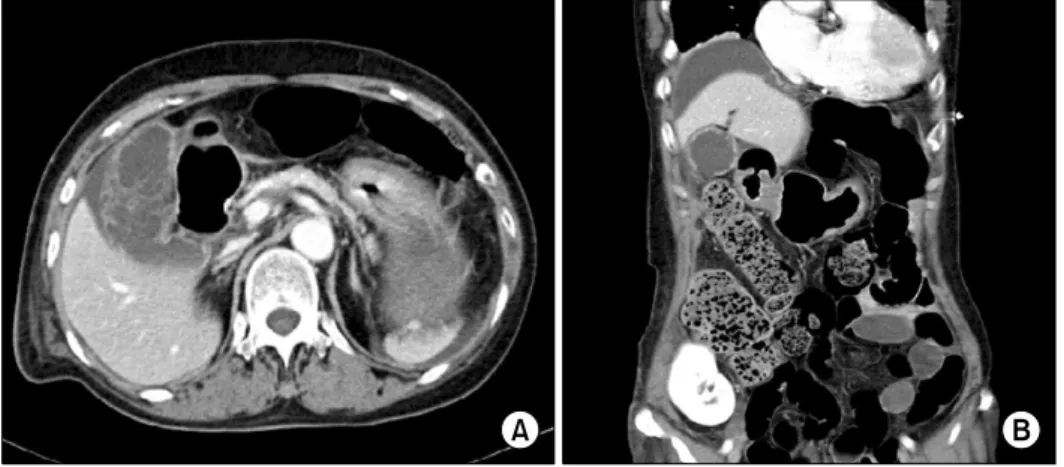
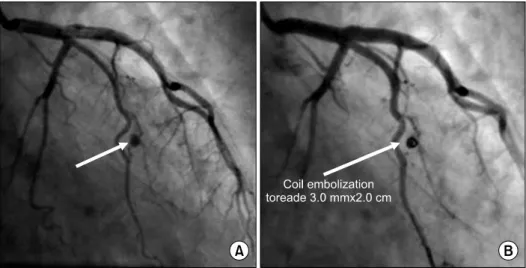
Acalculous Gallbladder Perforation and Coronary Artery Aneurysm after Kidney Transplantation
5
0
0
전체 글
(2)
(3)
(4)
(5)
수치
관련 문서
Chronic kidney disease (partial update): Early identification and management of chronic kidney disease in adults in primary and secondary care (Clinical
Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in
Purpose: This study was designed to evaluate the clinical characteristics and the treatment of colonoscopic perforation and the availability of
• Select one of the elemental technologies of Smart City and describe the current level of this technology, the direction of future technology development, and the urban space to
Article 14 (Allowances, etc,) The members who attend a meeting of the Deliberative Committee and a person who is required to attend the meeting to make
Methods: We conducted a retrospective analysis of clinical records of obese children who visited to Chosun university hospital between January 2013 and February 2014 due to
Polypoid lesions of the gallbladder; Report of 111 cases with surgical reference to operative indication.. Polypoid lesion of GB: Indication of carcinoma
Background: Incidence of complications related extracorporeal membrane oxygenation (ECMO) support as a bridge to lung transplantation (BTT) and its association with the
