CASE REPORT
대장 절제술 후 발생한 회장 정맥류 출혈을 캡슐 내시경으로 진단한 1예
박창준, 이봉은, 전혜경, 김광하, 송근암, 고상화1, 이소정2, 박도윤2
부산대학교 의학전문대학원 내과학교실, 외과학교실1, 병리학교실2
Case of Bleeding Ileal Varices after a Colectomy Diagnosed by Capsule Endoscopy
Chang Joon Park, Bong Eun Lee, Hye Kyung Jeon, Gwang Ha Kim, Geun Am Song, Sang Hwa Ko1, So Jeong Lee2 and Do Youn Park2 Departments of Internal Medicine, Surgery1 and Pathology2, Pusan National University School of Medicine, Busan, Korea
We report a case of bleeding ileal varices associated with intra-abdominal adhesions after colectomy which was successfully diag- nosed using capsule endoscopy. A 77-year-old woman visited the emergency department for several episodes of melena. She had a medical history of neoadjuvant chemo-radiation therapy and subsequent surgery for rectal cancer 6 years previously. Conventional diagnostic examinations including upper endoscopy, colonoscopy, and abdominal computed tomography could not detect any bleed- ing focus, however, following capsule endoscopy revealed venous dilatations with some fresh blood in the distal ileum, indicating bleeding ileal varices. The patient underwent exploratory laparotomy and the affected ileum was successfully resected. No further gastrointestinal bleeding occurred during the 6 months follow-up. Small intestinal varices are important differential for obscure gas- trointestinal bleeding especially in patients with a history of abdominal surgery in the absence of liver cirrhosis, and capsule endos- copy can be a good option for diagnosing small intestinal varices. (Korean J Gastroenterol 2018;71:349-353)
Key Words: Gastrointestinal hemorrhage; Capsule endoscopy
Received February 14, 2018. Revised March 21, 2018. Accepted March 28, 2018.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2018. Korean Society of Gastroenterology.
교신저자: 이봉은, 49241, 부산시 서구 구덕로 179, 부산대학교 의학전문대학원 내과학교실
Correspondence to: Bong Eun Lee, Department of Internal Medicine, Pusan National University School of Medicine, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea.
Tel: +82-51-240-7869, Fax: +82-51-244-8180, E-mail: [email protected]
Financial support: This work was supported by a Pusan National University Hospital Clinical Research Grant (2017).
Conflict of interest: None.
INTRODUCTION
The term “ectopic varices” is defined as large portosyste- mic venous collateral structures occurring anywhere in the abdominal cavity, except in the gastroesophageal region.1 Small intestinal varices, usually associated with portal hy- pertension secondary to liver cirrhosis or previous abdomi- nal surgery,2 are an uncommon cause of obscure gastro- intestinal bleeding (OGIB).3 Anatomically, these lesions are difficult to detect by conventional upper endoscopy and colo-
noscopy,4,5 and a diagnosis is even more difficult when physi- cians do not consider the existence of small intestinal varices in a differential diagnosis of OGIB. On the other hand, bleed- ing from small intestinal varices can be massive and life- threatening; therefore, early identification and taking appro- priate action are critical. Recently, advances in diagnostic methods, such as capsule endoscopy, deep enteroscopy, and radiographic imaging have made it possible to detect OGIB more effectively.3 In particular, capsule endoscopy is a useful noninvasive procedure for detecting small intestinal
Fig. 2. Capsule endoscopy showed bluish venous dilation with bloody intestinal fluids in the distal ileum.
A B C
Fig. 1. Colonoscopy showed dark blood retention in the entire colon, originating from oral side of the ileocecal valve. (A) Transverse colon.
(B) Ileocecal valce. (C) Terminal ileum.
bleeding.6
This paper reports a case of bleeding ileal varices asso- ciated with intra-abdominal adhesions after a colectomy, which was diagnosed successfully using capsule endoscopy.
CASE REPORT
A 77-year-old woman visited the emergency department due to several episodes of melena and abdominal pain. She had a medical history of neoadjuvant chemo-radiation ther- apy and a subsequent low anterior resection for rectal cancer 6 years previously. Upon admission, her blood pressure was 90/60 mmHg and pulse rate was 85/min. The initial hemo- globin level in the emergency department was 9.9 g/dL, in- dicating an abrupt decline compared to the level of hemoglo- bin (12.5 g/dL) measured at the general surgery department 2 weeks earlier. The other initial laboratory tests revealed the
following: white blood count, 8,080/μL; platelet count, 97,000/μL; prothrombin time, 12.0 sec (international nor- malized ratio: 1.04); blood urea nitrogen, 26.4 mg/dL; crea- tinine, 0.60 mg/dL; serum albumin, 3.3 g/dL; total bilirubin, 2.35 mg/dL; direct bilirubin, 0.69 mg/dL; serum aspartate aminotransaminase 34 IU/L; serum alanine amino- transaminase 35 IU/L. The serological markers for previous or current hepatitis B and C infections were negative, and there was no prior history of alcohol abuse. Conventional di- agnostic examinations, including upper endoscopy, colono- scopy, and abdominal computed tomography (CT), were per- formed to evaluate the bleeding focus. Upper endoscopy showed no evidence of bleeding. The colonoscopy revealed dark blood retention in the entire colon, originating from the oral side of the ileocecal valve (Fig. 1). Abdominal CT angiog- raphy did not show any obvious bleeding. On the other hand, the patient presented with recurrent massive melena, and
A B
C D E
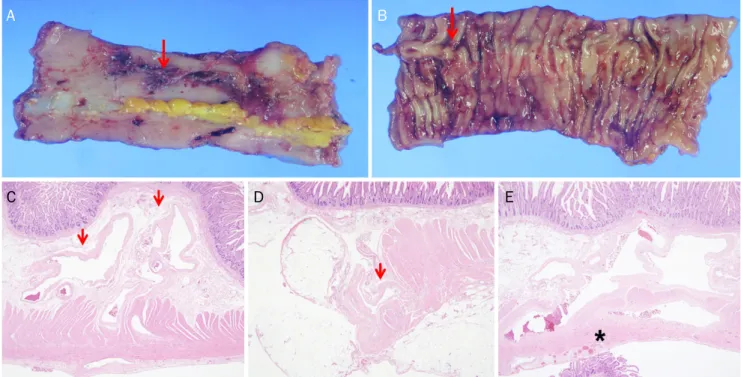
Fig. 4. Histopathology findings. (A, B) Gross findings of the resected ileum showed a well-defined tortuous, engorged vascular structure (red arrows) on the serosal (A) and mucosal (B) surface. (C, D) On a microscopic examination, submucosa (C, H&E, ×40) and subserosa (D, H&E, ×40) showed irregularly dilated venous structures (red arrows). (E) Fibrous bands (star) around the dilated tortuous varices were observed on the subserosa (H&E, ×40).
Fig. 3. Abdominal computed tomography revealed venous dilatation on the ileum (red arrows) adjacent to the uterus.
her anemia worsened despite conservative treatment with blood transfusions. Subsequent angiography for the superior mesenteric artery was performed but no bleeding focus could be found. The patient then underwent capsule endoscopy.
The results showed no evidence of active bleeding or retained blood in the duodenum, jejunum, and proximal ileum; how- ever, bluish distended vascular lesions along with newly emerged bloody intestinal fluids were detected in the distal ileum, suggestive of bleeding ileal varices (Fig. 2). Therefore,
the previous abdominal CT images were reviewed again, which revealed ileal varices adjacent to the uterus associated with a previous colectomy but no evidence of radiologic liver cirrhosis (Fig. 3). An exploratory laparotomy was performed, which revealed a small intestine adhered to the uterus with calcification and variceal changes. Adhesiolysis of the small intestine from the pelvic cavity and subsequent resection of the affected ileum were performed. The resected ileum had a tortuous, engorged vascular structure on the serosal and
mucosal surface (Fig. 4A, B). A microscopic examination re- vealed irregularly dilated vascular proliferation from the sub- mucosa to subserosa and subserosal fibrous bands (Fig.
4C-E). No further melena was observed after surgery and the patient was discharged home on the 17th postoperative day.
At the 6-month follow-up, the patient was stable with no fur- ther complications.
DISCUSSION
The authors encountered a patient with recurrent massive gastrointestinal (GI) bleeding from the ileal varices caused by previous abdominal surgery without liver cirrhosis. The initial upper endoscopy and colonoscopy did not reveal the bleed- ing focus, but the colonoscopy findings were indicative of small intestinal bleeding. Abdominal CT was performed ac- cording to the protocol for the detection of GI arterial bleeding, and a subsequent CT reading was focused on arterial bleed- ing, which led to the missed ileal varices as a bleeding cause.
Owing to the continued massive bleeding, angiography of su- perior mesenteric artery was performed as a next step but it failed to find any bleeding lesions. Indeed, small intestinal varices were not included in the differential diagnosis of OGIB because there was no evidence of liver cirrhosis, which is usu- ally considered a cause of varices. Hence, the diagnosis of bleeding ileal varices was delayed until the patient under- went capsule endoscopy.
OGIB is defined as persistent or recurrent bleeding from the GI tract after negative primary upper and lower endos- copies,4,5 and represents approximately 5% of those patients with all GI bleeding.7 With the introduction of capsule endos- copy and deep enteroscopy, the majority of patients with OGIB were found to have sources of bleeding located in the small intestine.8 Small intestinal bleeding can result from var- ious conditions, such as vascular, inflammatory, iatrogenic, tumorous, or diverticular disorders.7,9 A detailed medical his- tory, including comorbidities, prior history of cancer, radiation therapy or abdominal surgery, or any prescriptions, such as aspirin or non-steroidal anti-inflammatory drugs, needs to be taken when small intestinal diseases are suspected.7 Although ectopic varices are rare causes of small intestinal bleeding,3 they can cause massive GI bleeding with a high risk of rupture. Small intestinal varices distal to the duodenum, usually present with sudden, profuse melena or hema-
tochezia, or intraperitoneal bleeding,2,10 and they are also found in patients with chronic anemia or as a positive result for stool occult blood.2 Therefore, it is important to suspect the existence of small intestinal varices as a source of OGIB if a patient has the predisposing risk factors for ectopic varices. Most commonly, ectopic varices are caused by portal hypertension in the context of pre-existing liver cirrhosis or portal vein thrombosis.1 A study of 37 patients with liver cir- rhosis who underwent capsule endoscopy revealed 8.1% to have small intestinal varices.11 Other etiologies independent of portal hypertension include familial varices, intra-abdomi- nal adhesions from previous surgery, arteriovenous fistula secondary to trauma, mesenteric vein thrombosis, and lym- phoid hyperplasia.2 The formation of ileal varices is often the result of collateral circulation through postoperative adhe- sions between the ileum and abdominal wall or other organ.1,12,13 A triad of portal hypertension, hematochezia without hematemesis, and prior abdominal surgery charac- terize the hemorrhage from small intestinal varices.14 On the other hand, bleeding ectopic varices, particularly ileal vari- ces, cannot be diagnosed easily at an early stage. Because of their rarity, these lesions are often not included in a differ- ential diagnosis for OGIB, regardless of whether there is por- tal hypertension or not. The clinical suspicion for small in- testinal varices is critical for diagnosis, and developing tech- niques, such as capsule endoscopy and deep enteroscopy, may identify these lesions successfully. According to the guidelines of small intestinal bleeding, capsule endoscopy should be considered as a first-line procedure for small in- testinal evaluation if there is no obvious bleeding focus on the second-look examinations, such as upper endoscopy and colonoscopy.3 In the present case, capsule endoscopy suc- cessfully diagnosed the bleeding ileal varices. Thus, capsule endoscopy is a good option for diagnosing small intestinal varices non-invasively.
The treatment for bleeding ectopic varices has not been es- tablished clearly. Because of the infrequency of these le- sions, only a few case reports and small case series exist.
Therefore, the management of bleeding ectopic varices de- pends on the etiology and patient’s status,12 and may require a multidisciplinary team of gastroentero-hepatologists, sur- geons, and interventional radiologists. In most cases re- ported previously, surgery, such as a segmental resection or a shunt operation, has been the preferred treatment, and ap-
pears to successfully control the bleeding of small intestinal varices.15 On the other hand, not all patients can undergo sur- gery because of their poor medical condition. For such pa- tients, percutaneous treatment with interventional radio- logical techniques can be considered because it is less invasive. Recently, with the advancements in technology, in- terventional radiologic techniques (e.g., balloon-occluded retrograde transvenous obliteration,16 transjugular intra- hepatic portosystemic shunt,17 and percutaneous trans- hepatic sclerotherapy18) and endoscopic techniques (e.g., in- jection of a sclerosant solution via deep enteroscopy19) have been used to treat ileal variceal bleeding. In the present case, the patient was managed successfully with surgical treat- ment including adhesiolysis and resection of the affected ileum.
In conclusion, small intestinal varices are important in a differential diagnosis for OGIB, particularly in patients with a history of abdominal surgery. Moreover, capsule endoscopy can be a good option for diagnosing small intestinal varices.
Although surgical resection is an essential treatment for small intestinal varices associated with intra-abdominal ad- hesions after previous surgery, radiologic interventions can be considered as an alternative option for patients in a poor medical condition.
REFERENCES
1. Lebrec D, Benhamou JP. Ectopic varices in portal hypertension.
Clin Gastroenterol 1985;14:105-121.
2. Helmy A, Al Kahtani K, Al Fadda M. Updates in the pathogenesis, diagnosis and management of ectopic varices. Hepatol Int 2008;2:322-334.
3. Gerson LB, Fidler JL, Cave DR, Leighton JA. ACG clinical guideline:
diagnosis and management of small bowel bleeding. Am J Gastroenterol 2015;110:1265-1287.
4. Raju GS, Gerson L, Das A, Lewis B, American Gastroenterological Association. American Gastroenterological Association (AGA) in- stitute technical review on obscure gastrointestinal bleeding.
Gastroenterology 2007;133:1697-1717.
5. Zuckerman GR, Prakash C, Askin MP, Lewis BS. AGA technical re- view on the evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology 2000;118:201-221.
6. Iddan G, Meron G, Glukhovsky A, Swan P. Wireless capsule endoscopy. Nature 2000;405:417.
7. Ohmiya N, Nakagawa Y, Nagasaka M, et al. Obscure gastro- intestinal bleeding: diagnosis and treatment. Dig Endosc 2015;27:285-294.
8. Pasha SF, Leighton JA, Das A, et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin Gastroenterol Hepatol 2008;6:671-676.
9. Pennazio M, Eisen G, Goldfarb N, ICCE. ICCE consensus for obscure gastrointestinal bleeding. Endoscopy 2005;37:1046-1050.
10. Sato T, Akaike J, Toyota J, Karino Y, Ohmura T. Clinicopathological features and treatment of ectopic varices with portal hypertension. Int J Hepatol 2011;2011:960720.
11. De Palma GD, Rega M, Masone S, et al. Mucosal abnormalities of the small bowel in patients with cirrhosis and portal hyper- tension: a capsule endoscopy study. Gastrointest Endosc 2005;62:529-534.
12. Norton ID, Andrews JC, Kamath PS. Management of ectopic varices. Hepatology 1998;28:1154-1158.
13. Philips CA, Arora A, Shetty R, Kasana V. A comprehensive review of portosystemic collaterals in cirrhosis: historical aspects, anat- omy, and classifications. Int J Hepatol 2016;2016:6170243.
14. Cappell MS, Price JB. Characterization of the syndrome of small and large intestinal variceal bleeding. Dig Dis Sci 1987;32:422-427.
15. Kobayashi K, Yamaguchi J, Mizoe A, et al. Successful treatment of bleeding due to ileal varices in a patient with hepatocellular carcinoma. Eur J Gastroenterol Hepatol 2001;13:63-66.
16. Sato T, Yamazaki K, Toyota J, Karino Y, Ohmura T, Akaike J. Ileal varices treated with balloon-occluded retrograde transvenous obliteration. Gastroenterology Res 2009;2:122-125.
17. Castagna E, Cardellicchio A, Pulitanò R, Manca A, Fenoglio L.
Bleeding ileal varices: a rare cause of chronic anemia in liver cirrhosis. Intern Emerg Med 2011;6:271-273.
18. Iguchi T, Yabushita K, Sakaguchi K, et al. Percutaneous trans- hepatic sclerotherapy for bleeding ileal varices associated with portal hypertension and previous abdominal surgery. Jpn J Radiol 2010;28:169-172.
19. Traina M, Tarantino I, Barresi L, Mocciaro F. Variceal bleeding from ileum identified and treated by single balloon enteroscopy.
World J Gastroenterol 2009;15:1904-1905.