<접수일:2007년 10월 29일, 심사통과일:2007년 11월 29일>
※통신저자:이 수 곤
서울시 서대문구 신촌동 134 연세대학교 의과대학 내과학교실
Tel:02) 2228-1947, Fax:02) 393-6884, E-mail:[email protected]
Kikuchi병에 동반된 성인형 스틸병 1예
연세대학교 의과대학 내과학교실, 병리학교실*
강은진ㆍ최상태ㆍ이상원ㆍ정상윤ㆍ손명균ㆍ이광훈ㆍ양우익*ㆍ박용범ㆍ이수곤
= Abstract =
Kikuchi-Fujimoto's Disease with Adult Onset Still's Disease
Eun-Jin Kang, M.D., Sang Tae Choi, M.D., Sang-Won Lee, M.D., Sang Youn Jung, M.D., Myoung Kyun Son, M.D., Kwang-Hoon Lee, M.D., Woo Ick Yang, M.D.*,
Yong Beom Park, M.D., Soo-Kon Lee, M.D.
Division of Rheumatology, Department of Internal Medicine, Department of Pathology*, Yonsei University College of Medicine, Seoul, Korea
Kikuchi-Fujimoto’s disease (KFD), or histiocytic necrotizing lymphadenitis, is a rare benign and self-limiting disease. KFD are confused with systemic autoimmune disease as they present with localized lymphadenopathy, fever, fatigue, arthritis, leukopenia. Furthermore as KFD can occur associated with other autoimmune disease, we need to diagnose carefully. Here, we describe a case of 27-year-old female patient, diagnosed as KFD, who subsequently developed adult onset Still’s disesase (AOSD). As far as we know, this is the first case of KFD with AOSD in Korea.
Key Words: Kikuchi-Fujimoto’s disease, AOSD, Lymphadenopathy
서 론
Kikuchi병(Kikuchi-Fujimoto's disease)은 주로 젊은
여성에서 호발하며 림프절 종대, 발열, 관절통, 백혈 구 감소를 특징으로 하는 질환으로 대부분 자연 치 유되는 경과를 보이는 것으로 알려져 있다 (1). 발병 원인은 뚜렷하지 않으나 여러 가지 바이러스 감염과
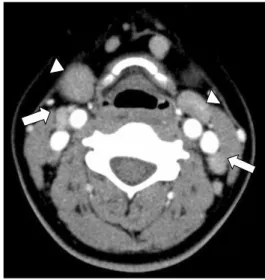
Fig. 1. Neck computed tomography scan shows mild hyperplasia of lingular tonsils (arrow head) and multiple lymphadenopathies (arrow) bilaterally.
전신홍반루푸스, 다발성 근육염, 혼합 결체조직 질 환, 성인형 스틸병등의 자가면역질환과의 연관성이 제기되고 있다 (2-7). 증상이 비특이적이므로 Epstein- Barr virus (EBV) 감염, 식혈증후군, 전신홍반루푸스, 성인형 스틸병 등과의 감별이 중요하며 때로는 이러 한 질병과 동반되어 발현되는 경우도 있다 (8). 그러 나 국내에서는 성인형 스틸병에서 동반된 증례는 보 고된 바가 없었다. 저자들은 경부 림프절 종대와 발 열을 주소로 내원하여 Kikuchi병으로 진단되었으나 경과중 성인형 스틸병이 병발된 증례를 경험하였기 에 문헌고찰과 함께 보고하고자 한다.
증 례
환 자: 27세 여자 주 소: 경부 종물, 발열
과거력 및 현병력: 2년 전 타병원에서 피부발진을 동반한 다발성 관절통을 주소로 혈청음성 류마티스 관절염 의심하에 2개월간의 항말라리아제제, 저용량 스테로이드 복용 후 호전되었던 과거력이 있던 환자 로 이후 증상 없이 지내다 내원 3일 전부터 경부종 물과 발열, 피부발진, 양측 무릎 관절통이 발생하여 본원에 외래경유하여 입원하였다.
신체 검사 소견: 체온 39.3도, 맥박수 74회/분, 호 흡수 24회/분, 혈압 110/70 mmHg이었고 급성 병색 이었으며 의식은 명료하였다. 공막에 황달은 없었으 며 결막은 창백하지 않았다. 양측 하악골 하부에 압 통을 동반한 1 cm 크기의, 단단하게 만져지는 종물 이 촉지되었고 얼굴과 하지에 발열 시 동반되는 홍 반성의 반점상 구진이 관찰되었다. 흉부 청진에서 호흡음은 깨끗하였고, 심음은 규칙적이었으며 심잡 음은 청진되지 않았다. 복부는 부드럽고 편평하였으 며 장음은 항진되지 않았다. 사지에 함요 부종은 관 찰되지 않았으나 양측 무릎의 압통이 관찰되었다.
검사실 소견: 말초 혈액 검사에서 백혈구 6,540/
mL (호중구 74.7%), 혈색소 10.1 g/dL, 혈소판 318,000/
mL이었으며, 일반화학 검사상 AST 17 IU/L, ALT 9 IU/L, ferritin 266 ng/mL (정상치: 10∼291), LDH 459 IU/L (정상치: 225∼455)이었다. C-반응단백은 6.1 mg/
dL (정상치: 0∼0.8), 적혈구침강속도는 86 mm/hr (정 상치: 0∼20)이었다. 혈액배양 검사와 요배양 검사는
음성이었다. 바이러스에 대한 혈정학적 검사에서 HBs Ag 음성, anti-HBs 양성, anti-HCV 음성이었으며, CMV (cytomegalovirus) IgM, anti-HIV, EBV-VCA (viral cap- sid antigen) IgM, EBV-EA (early antigen) IgM 항체 모두 음성이었다. 면역학적 검사에서 항핵항체 양성 (1:160, speckled type), 루푸스항응고인자 양성 소견 을 보였으며 항dsDNA 항체 음성, 항Sm 항체 음성, 항cardiolipin 항체 음성, 류마티스인자 음성, 항CCP 항체(anti-cyclic citrullinated peptide antibody)는 음성 이었다. 골수검사는 정상소견을 보였다.
방사선학적 소견: 경부 컴퓨터단층촬영에서 양측 경부에 1∼2 cm 크기의 다발성 림프절 종대 소견과 경도의 편도비대 소견이 관찰되었다(그림 1).
병리학적 소견: 왼쪽 경부 림프절의 조직검사에서 핵붕괴 물질과 섬유소양 물질로 구성된 호산성의 괴 사 영역이 관찰되었으며 그 주변으로 다수의 단핵구 침윤과 림프구, 조직구의 증식이 관찰되었다. 호중구 나 형질세포의 침윤은 없었다(그림 2).
치료 및 경과: 경부 조직검사에서 Kikuchi병으로 진단되어 meloxicam 투여를 시작하였으나 39도 이상 의 간헐적인 발열은 2주 이상 지속되었고 관절통도 양측 무릎, 양측 팔꿈치, 양측 손목, 양측 어깨로 이 동하면서 악화되는 소견을 보였다. 인후통과 함께
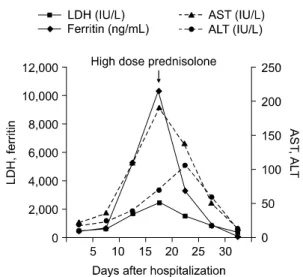
Fig. 3. Changes of liver function tests and serum ferritin level during the course of treatment. LDH: lactate dehydrogenase, AST: aspartate aminotransferase, ALT: alanine aminotransferase.
Fig. 2. Lymph node biopsy shows necrotizing lesion composed of various histiocytes, plasmacytoid monocytes and lymphoid cells with karyor- rhectic nuclear debris (H&E, original magni- fication ×200).
발열시 동반되는 홍반성 반점상 구진도 지속되었으 며 백혈구 12,210/mL (호중구 87.8%), AST 203 IU/L, ALT 105 IU/L, ferritin 10,323 ng/mL, LDH 2470 IU/
L, C-반응단백 11.9 mg/dL, 적혈구침강속도도 120 mm/
hr로 증가 양상을 보였다. 1주일 이상 지속된 39도 이상의 발열, 2주일 이상 지속된 다발성 관절통, 발 열시 동반된 피부발진, 백혈구 증가증, 간기능 이상 의 양상을 종합해볼 때 Yamaguchi 등에 의한 성인 형 스틸병의 진단기준에 합당한 소견보여 Kikuchi병 에 동반된 성인형 스틸병으로 진단하였다 (9). 고용 량의 경구용 스테로이드(prednisolone 60 mg/day)와 메토트렉세이트 7.5 mg/주를 투여 시작하였으며 이 후 발열, 관절통, 피부 발진, 림프절 종대 소견이 호 전되었다. 검사소견도 AST 13 IU/L, ALT 13 IU/L, LDH 347 IU/L, ferritin 25.8 ng/mL, C-반응단백 0.128 mg/dL, 적혈구침강속도 11 mm/hr로 호전되어 퇴원 후 메토트렉세이트 10 mg/주까지 증량한 뒤 추적 관 찰 중이다(그림 3).
고 찰
Kikuchi병은 경부 림프절 종대, 발열, 백혈구 감소 증, 인후통, 적혈구침강속도 상승을 보이고 30세 미 만의 젊은 여성에서 호발하는 질환으로 1972년 Ki-
kuchi와 Fujimoto에 의해 처음 보고되었다. 남녀의 비율은 2∼4:1로 여성에서 더 호발하며 대부분 자연 치유되는 경향이 있는 것으로 알려져 있고 재발율은 3∼5%로 알려져 있다. 환자의 80% 이상이 무증상의 림프절 종대 혹은 발열을 동반한 림프절 종대를 보 이고 경부 림프절을 가장 흔히 침범하는 것으로 알 려져 있다. 검사실 소견에서 백혈구 감소증이 약 50%에서 보이는 것으로 보고되고 있으며 Kikuchi병 의 진단을 위한 생화학 또는 혈청학적 검사는 없으 며, 정확한 진단을 위해서는 조직학적 생검이 필수 적이다 (3,10).
발병원인에 대해서는 아직 명확히 밝혀진 바는 없 지만 EBV, human herpes virus (HHV)-6, HHV-8, HIV, CMV, parvovirus B19, Yersinia, Brucella species 등과 의 연관성이 제기된 바 있으며 이는 감염에 의한 조 직구과 T림프구의 증강된 면역반응으로 유발되는 것으로 설명하고 있다 (2,3). 자가면역 기전에 의한 발생 가능성도 제시되고 있는데 전신홍반루푸스, 다 발성 근육염, 혼합 결체조직 질환, 항인지질 증후군, 성인형 스틸병과의 연관성이 보고된바 있다 (4-7).
특히 전신홍반루푸스가 진단되기 이전, 동시 혹은 진단이후 Kikuchi병의 동반 발생이 보고되어 Kikuchi 병의 진단 시 전신홍반루푸스에 대한 진단적 접근
Table 1. Cases of Kikuchi-Fujimoto's disease (KFD) with adult onset Still's disease (AOSD)
Reference Sex/age Diagnosis of AOSD Lymphadenopathy Treatment Prognosis Ohta et al (7) M/41 Arthralgia, fever, rash, sore throat, Cervical, axillary NSAID Improved
abnormal LFT, splenomegaly inguinal prednisolone (50 mg/day)
M/19 Arthralgia, fever, leukocytosis, Cervical NSAID Improved abnormal LFT, hepatosplenomegaly prednisolone
F/14 Arthralgia, fever, rash, leukocytosis, Cervical Prednisolone Improved sore throat, hepatomegaly (30 mg/day)
Lyberatos et al (14) M/18 Arthralgia, fever, rash, leukocytosis, Generalized Prednisolone Improved abnormal LFT, hepatosplenomegay
F/47 Arthralgia, fever, rash, sore throat Cervical, axillary Aspirin Improved Cousin et al (15) M/32 Arthralgia, fever, rash, leukocytosis, Cervical, axillary Prednisolone Improved
ANA(−), RF(−) inguinal (60 mg/day)
Our patient F/27 Arthralgia, fever, rash, leukocytosis, Cervical Prednisolone Improved sore throat, abnormal LFT, ANA(+) (60 mg/day)
및 추적 관찰이 필요하다고 보고하고 있고 Ohta 등 은 Kikuchi병, 성인형 스틸병, 전신홍반루푸스가 림 프구친화성 바이러스에 의한 숙주의 면역 변화에 따 른 동일한 병인기전을 가진 질환임을 주장하기도 하 였다 (4,11).
본 증례는 경부 림프절 종대의 조직검사상 아급성 괴사성 림프절염 소견을 보여 Kikuchi병으로 진단하 였으며 이는 부피질 과형성, 혈관의 증식 및 면역모 세포 반응을 보이는 성인형 스틸병의 조직 소견과는 차이를 보였다 (10,12). 임상적으로도 경부 림프절 종 대 이외에 Kikuchi병에서 나타나는 미열의 양상보다 는 39도 이상의 고열양상을 보였으며 (13), 고열 시 동반되었다 사라지는 홍반성 반점양 구진, 2주 이상 지속된 다발성 관절통을 보였고, 검사상에서도 80%
이상이 호중구를 이루는 백혈구 증가증, 간기능 검 사 상승, 10,000 ng/mL 이상의 ferritin 상승이 동반되 어 Kikuchi병에 동반된 성인형 스틸병으로 진단하였 다. 항핵항체 양성, 루푸스 항응고인자 양성 소견을 보여 전신홍반루푸스와의 동반 가능성을 의심하였으 나 구강궤양, 광과민성, 나비모양 홍반, 장막염등의 임상양상이 관찰되지 않았고, 혈액검사상에서도 백 혈구 감소증 보다는 백혈구 증가증 소견을 보였고 항dsDNA 항체, 항Sm 항체에서 모두 음성 소견을 보여 전신홍반루푸스의 진단기준을 만족하지는 못하 였다.
Kikuchi병과 성인형 스틸병과의 연관성은 드물게
보고 되고 있는데, 발병 연령은 18세에서 47세, 경부 의 림프종물 양상이 가장 흔하였고, Lyberatos 등이 보고한 경우를 제외하고 모두 경구용 스테로이드 치 료후 호전을 보였다 (14,15) (표 1). 본 증례의 경우 도 발병 연령이 27세였으며 경부의 림프종물을 호소 하였고, 소염진통제 복용에도 호전 양상 관찰되지 않고 악화 소견 지속되어 고용량 경구용 스테로이드 치료와 메쏘트렉세이트 병용 요법을 시행하였다. 고 용량 경구용 스테로이드 치료 후에는 증상 호전 양 상을 보였으며, 혈액검사상에서도 급격한 ferritin의 감소 소견을 보였고 이후 LDH, AST, ALT의 정상화 를 관찰할수 있었다(그림 3). 진단 후 6개월 동안 저 용량 스테로이드(prednisolone 5 mg/일)와 메토트렉세 이트 10 mg/주를 복용하였으며, 재발의 양상 및 전 신홍반루푸스를 시사하는 소견은 관찰되지 않았으 나, 항핵항체와 루푸스 항응고인자에서 양성소견을 보였고 자가면역 기전과의 연관성을 고려할 때 향후 전신홍반루푸스로의 진행양상에 대한 추적 관찰이 필요하다.
요 약
본 저자들은 발열과 경부 림프절 종대를 주소로 내원하여 Kikuchi병에 동반된 성인형 스틸병으로 진 단된 증례를 경험하여 문헌고찰과 함께 보고하는 바 이다.
참고문헌
1) Kikuchi M. Lymphadenitis showing focal reticulum cell hyperplasia with nuclear debris and phagocytosis.
Acta Hematol Jpn 1972;35:379-80.
2) Charalabopoulos K, Papalimneou V, Charalabopoulos A, Chaidos A, Bai M, Bourantas K, et al. Kikuchi- Fujimoto disease in Greece. A study of four cases and review of the literature. In Vivo 2002;16:311-6.
3) Kucukardali Y, Solmazgul E, Kunter E, Oncul O, Yildirim S, Kaplan M. Kikuchi-Fujimoto disease:
analysis of 244 cases. Clin Rheumatol 2007;26:50-4.
4) Santana A, Lessa B, Galrao L, Lima I, Santiago M.
Kikuchi-Fujimoto's disease associated with systemic lupus erythematosus: case report and review of the literature. Clin Rheumatol 2005;24:60-3.
5) Wilkinson CE, Nichol F. Kikuchi-Fujimoto disease associated with polymyositis. Rheumatology (Oxford) 2000;39:1302-4.
6) Pallet N, Aaron L, Larousserie F, Therby A, Dupont B, Viard JP. Kikuchi-Fujimoto disease associated with mixed connective tissue disease. Scand J Rheumatol 2004;33:434-6.
7) Ohta A, Matsumoto Y, Ohta T, Kaneoka H, Yama- guchi M. Still's disease associated with necrotizing
lymphadenitis (Kikuchi's disease): report of 3 cases.
J Rheumatol 1988;15:981-3.
8) 조자경, 한석재, 배종엽, 정승혜, 김채기, 최정윤. 전신 성 홍반성 루푸스 환자에서 재발한 Kikuchi- Fujimoto disease. 대한내과학회지 2006; 70: 107-10.
9) Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, et al. Preliminary criteria for classification of adult Still's disease. J Rheumatol 1992;19:424-30.
10) 최정우, 이지혜, 이주한, 채양석, 김인선. The clinic- opathologic analysis of Kikuchi's lymphadenitis. 대한 병리학회지 2004; 38: 289-94.
11) Ohta A. Letter (reply to Lyberatos C.). J Rheumatol 1990;17:569.
12) Jeon YK, Paik JH, Park SS, Park OS, Kim YA, Kim JE, et al. Spectrum of lymph node pathology in adult onset Still's disease; analysis of 12 patients with onefollow up biopsy. J Clin Pathol 2004;57:1052-6.
13) Dorfman RF, Berry GJ. Kikuchi's histiocytic necro- tizing lymphadenitis: an analysis of 108 cases with emphasis on differential diagnosis. Semin Diagn Pathol 1988;5:329-45.
14) Lyberatos C. Two more cases of Still's disease and Kikuchi's. J Rheumatol 1990;17:568-9.
15) Cousin F, Grezard P, Roth B, Balme B, Gregoire- Bardel M, Perrot H. Kikuchi disease associated with Still disease. Int J Dermatol 1999;38:464-7.