Abstract
Purpose: The aim of this study was to investigate bone tissue reaction according to different implant surfaces by measurement of bone implant contact (BIC) ratio and bone area ratio in ovariectomized rats.
Materials and Methods: Sprague-Dawley female rats underwent ovariectomy for osteoporosis. After 8 weeks, 4-types implants (machined, Resorbable Blasted Media, Cellnest surface and Calcium Meta Phosphate-coated) were inserted into the medial side of the tibia. Unthreaded cylindrical-type implants (Ø1.2 mm, L2.0 mm, Osstem Co., Busan, Korea) were used. Rats were sacrificed at 2 and 4 weeks after implantation. Specimens were harvested and histomorphometric evaluations were performed by measurement of the BIC ratio and bone area ratio using the Kappa image base control program (Kappa Opto-electronic. Germany). Statistical analysis of each variable was evaluated by the ANOVA test using the SAS (ver. 9.1, SAS Institute, USA) for Windows.
Results: According to the method of surface treatment, the difference in early ossification for the implant was observed. Surface treated implants showed a significantly higher compact bone contact ratio compared with the machined implant at 2 and 4 weeks after implantation. Surface treated implants demonstrated a significantly higher marrow bone contact ratio compared with machined implants at 4 weeks after implantation. Surface treated implants showed a significantly higher compact bone area ratio compared with machined implants at 4 weeks after implantation.
Conclusion: In bones of poor quality, surface treated implants will provide greater stability compared with machined implants.
Key Words: coated materials, implant, osteoporosis
Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats
Jeong-Yol Lee1, Hyun-Joo Oh1, Sun-Jong Kim2, Sang-Wan Shin1
1Department of Dental Prosthetics, Korea University Medical Center, Institute for Clinical Dental Research, Graduate School of Clinical Dentistry, Korea University, Seoul, Korea
2Department of Oral & Maxillofacial Surgery, School of Medicine, Ehwa Womans University, Seoul, Korea
Reprint requests: Sang-Wan Shin
Department of Dental Prosthetics, Korea University Guro Hospital, Institute for Clinical Dental Research, Graduate School of Clinical Dentistry, Korea University, 148 Gurodong-ro, Guro-gu, Seoul 152-703, Korea
Tel: 82-2-2626-1922, Fax: 82-2-866-1499 E-mail: [email protected]
Received for publication: September 19, 2012 Accepted for publication: September 24, 2012
Copyright © 2012. The Korean Academy of Oral & Maxillofacial Implantology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
increase more, and the need for dental implantation in patients with osteoporosis or poor bone quality will increase as the elderly population increases. Although implant surfaces are being treated with various meth- ods to increase the implant success rate, few studies have investigated the differences between various sur- face treatment techniques for osteoporosis patients. As such, this study was conducted to identify which of the four surface treatment techniques are effective for implant osseo-integration in the jaw bone, by histo- morphometrically observing the bone tissue reaction in rats in which osteoporosis was induced.
II Materials and Methods
1. Preparation of the test animals
16 female Sprague-Dawley rats aged 16 weeks (mean weight: 260 g each) were acclimated for 2 weeks or more and then used. After the pretreatment of the rats with 0.05 mg/kg of atropine (Yuhan Co., Seoul, Korea), 7.5 mg/kg of zoletile (Virbac, Carros, France) was intraperitoneally injected to induce general anes- thesia.
After making an incision in the peritoneal cavity, the ovary was taken out, and then the center of the uterine tube was ligated using a suture and the ovary was resected (Fig. 1). In the normal control group, after general anesthesia was administered, an equivalent amount of fat tissue was removed from near the ovary.
Then after the ovary was ligated and put back in the peritoneal cavity, the ovary was sutured and disinfected.
I Introduction
Osteoporosis is a disease that continuously increases the risk of fracture and decreases the bone volume while changing the bone microstructure1,2. The decreased bone volume decreases the bone-implant contact (BIC) area, which may make implant osseo-integration unsuccessful3. When osteo- porosis occurs in the jaw bone, it can be more serious in the maxilla than in the mandible4-6. Degeneration of the jaw bone, which is attributable to either osteopo- rosis or aging, is accompanied by increased porosity of the cortical bone and decreased density of the cancel- lous bone, as well as increased risk of vertical bone resorption in the jaw bone due to periodontal infection or odontoptosis7. Thus, in osteoporosis patients, osseo-integration, a necessary factor for successful dental implantation, may not be achieved8-12.
Studies have reported that implant-bone integration was influenced by the bone condition, the patient’s age, the position of implant in the jaw bone, and the implant type and surface treatment method4,11-13. Implants are currently being treated in clinical practice using various surface treatment methods such as sandblasting with a large grit and acid etching14, anodic oxidation15, hydroxy apatite (HA) coating16,17, use of resorbable blasting media (RBM)18, Cellnest sur- face treatment19, and calcium meta phosphate (CMP) coating19.
As the clinical success rate of implants gains credi- bility, implant-based restoration is expected to
2. Preparation of the implants
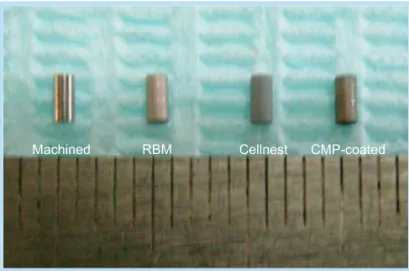
The unthreaded cylindrical-type implants (Osstem Co., Busan, Korea) were prepared as follows. The length and diameter of the implants were 2.0 mm and 1.2 mm, respectively; machined-, RBM-, Cellnest-, and CMP-coated-surface implants were used; and their surface roughness was measured as 1.69 mm using the probe (diameter: 2 μm) of a contact surface roughness measurement tester (SV-3000S4, Mitutoyo, Kanagawa, Japan) (Fig. 2).
3. Placement of the implants
As estrogen deficiency is induced within seven days after the resection of the ovary2 and the osteoporotic changes occurs two weeks after the resection, ovari- ectomy was performed to sufficiently induce osteopo- rosis, and the implants were placed eight weeks after the resection. In the control group that did not under- go ovariectomy, the implants were placed at the same
time point.
After general anesthesia was induced, using the typical procedure, two implants per type of implant were placed on the anterior surface of the proximal tibia in the control group, and three implants per type of implant in the ovariectomy group (the ovariectomy group was divided into the two-weeks subgroup and the four-weeks subgroup) (Table 1).
Two and four weeks after the implantation, the rats were sacrificed using cervical dislocation, after which tissue specimens were collected. At the time of the sacrifice, a blood sample was taken and the alkaline phosphatase (ALP) level in the blood was measured.
The blood ALP levels of the control group and the ovariectomy group were compared to see if they had any significant difference.
4. Observation methods
1) Preparation of the non-calcified specimens The implants and bone tissues collected from the Fig. 1. Ovariectomy of the experimental rat.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
Fig. 2. Photograph of the experimental implants. RBM:
resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
areas around the implants were fixed in 10% neutral buffered formalin for 48 hours or more, and then specimens were made using the general procedure.
Then the specimens were stained with H&E, and then observed with an optic microscope. For the histomor- phometric analysis, the digital images of the speci- mens that were taken using a digital camera (Kappa Dx30, Kappa Opto-electronics, Gleichen, Germany) affixed to an optic microscope (Olympus BX51, Olympus Co., Tokyo, Japan) were transferred to a computer. Then the relevant parameters of the speci-
mens were quantified using the Kappa Image Base Control 2,3,5 image analysis software (Kappa Opto- electronics).
The bone-implant direct contact ratio of each implant was measured at ×100 magnification, after which the mean of the bone-implant direct contact ratio was calculated and converted into a percentage.
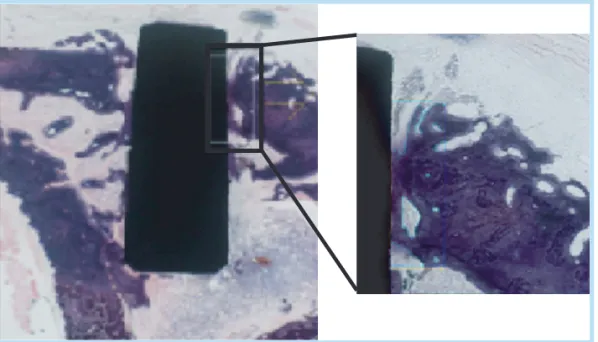
For the mineralized bone ratio, the area of the miner- alized bone within 200 μm of the lateral side of the implant was measured under ×100 magnification and converted into a percentage (Fig. 3).
Table 1. Types of experimental implants and numbers of harvested specimens
Implant Control Ovariectomy
Total
2 weeks 2 weeks 4 weeks
Machined-surface 2 3 3 8
RBM-surface 2 3 3 8
Cellnest-surface 2 3 3 8
CMP-coated 2 3 3 8
RBM: resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats. Implantology 2012
Fig. 3. Image analysis of a non- decalcificied tissue with the implant (H&E, ×100). The demarcated area was calibrated with the Kappa Image Base Control 2,3,5 program (Kappa Opto-electronics, Germany).
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats. Implantology 2012
2) Preparation of the calcified specimens
After the collected tissues that included the speci- mens were fixed in the formalin and decalcified using a 10% EDTA solution, they were embedded in paraffin and stained with H&E.
3) Histological findings
The differences in the overall bone tissue and the change in the bone marrow between the control group and the experiment group were compared using the calcified specimens to observe the histological change that occurred when osteoporosis was induced via ovariectomy, and the process of formation of new bones on the interface of the implant and the bone, and the shape of the newly formed bone, were observed using an optic microscope to identify the effects of osteoporosis on the implant osseo-integra- tion. In addition, the differences in the processes of ossification of the different surface treatment methods were compared via microscopic observation.
4) Statistics
For the histomorphometric analysis, one-way ANOVA was performed; and to determine the differ- ences between the groups, Duncan’s Multiple Range Test for Ratios was performed using SAS (ver. 9.1, SAS Institute, Cary, NC, USA). The differences were considered statistically significant at p<0.05.
III Results
1. Biochemical analysis
At the time of sacrifice of the animals, blood samples were taken and the blood ALP level was measured. The mean blood ALP level in the control group was 75 IU/L, and in the ovariectomy group, 91.8 IU/L.
2. Histological findings
Two weeks after the implantation, in the control group that did not undergo ovariectomy, bone remod- eling was active. In the compact bone areas, most of the newly formed bones were directly connected to the surface of the implant. In the cancellous bone, most of the surfaces of the implant covered the newly formed bones, the trabeculae were compact, and a reticular structure was observed (Fig. 4).
In contrast, in the ovariectomy group wherein osteo- porosis was induced, parts of the surface of the implant were connected to the newly formed bones in
Fig. 4. Histological specimen of the normal rats two weeks after the implantation of the CMP-coated-surface implant (H&E, ×40).
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
the compact bones, and bone resorption was observed.
In the cancellous bones, parts of the newly formed bones on the surface of the implant were thin, myeloid tissues were rare, and the reticular structures were underdeveloped. Yellow bone marrow that was rich in adipocytes was also observed (Fig. 5).
In the four-week subgroup, parts of the surface of the implant were connected to the newly formed bones and compared with the two-week subgroup, in which more newly formed bones were observed than on the surface of the implant in the cancellous bone areas.
The four-week and two-week subgroups did not sig- nificantly differ. Reticular bone structures were rarely observed, and yellow bone marrow was observed.
The processes of ossification in the various surface treatment methods differed (Figs. 6, 7). Two weeks after the implantation, in the machined-surface implant, new bones were being formed in the compact bone toward the surface of the implant, but direct contact between the newly formed bones and the implant was rare or was observed only in some areas.
In the cancellous bone, thin layers of newly formed bones were observed on the surface of the implant, and a microgap was observed in most parts of the interface of the newly formed bones and the surface of the implant. In the RBM-surface implant, newly formed bones that were similar to those on the machined- surface implant were observed in the compact bone, but microgaps were rarely observed between the sur- face of the implant and the newly formed bone. In the cancellous bone, early ossification was found to have started on the surface of the implant. In the Cellnest- surface implant, the newly formed bone was in close contact with the surface of the implant in the compact
Fig. 6. Histological findings for the non-decalcified specimen two weeks after the implantation (osteoporotic groups, H&E, ×100). RBM: resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats. Implantology 2012
Fig. 5. Histological specimen of the osteoporotic rats two weeks after the implantation of the RBM-surface implant (H&E, ×40).
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
bone, and the ossification was found to have pro- gressed on the surface of the implant. In addition, in the areas where ossification did not occur, character-
istics of the pre-ossification phase were observed. In the cancellous bone, ossification was in progress on the surface of the implant. In the CMP-coated-
Fig. 7. Histological findings for the non-decalcified specimen (osteoporotic groups, H&E, ×1.25). RBM: resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats. Implantology 2012
surface implant, ossification was found to have started around the particles that were attached to or detached from the surface of the implant and in progress on the surface of the implant in both the bone and the can- cellous bone, and no foreign body reaction was observed. The histological findings four weeks after the implantation showed that the ossification was slightly more progressive than two weeks after the implantation.
3. Histomorphometric analysis
1) BIC ratios in the compact bone
Two weeks after the implantation, the BIC ratios in the machined-, RBM-, Cellnest-, and CMP-coated- surface implants were 0.05%, 0.23%, 0.35%, and 0.26%, respectively, and the BIC ratios of the machined-surface and surface-treated implants sig- nificantly differed (p=0.0155). Four weeks after the implantation, the BIC ratios of the machined-, RBM-, Cellnest-, and CMP-coated-surface implants were 0.06%, 0.45%, 0.39%, and 0.58%, respectively, and the
BIC ratios of the machined-surface and surface- treated implants significantly differed (p=0.0212), unlike those of the surface-treated implants (Table 2, Fig. 8).
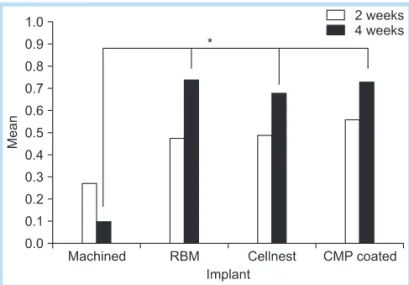
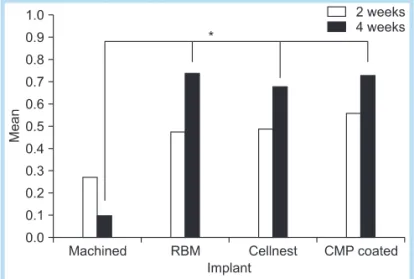
2) BIC ratios in the cancellous bone
In the two-week subgroup, the BIC ratios in the machined-, RBM-, Cellnest-, and CMP-coated- surface implants were 0.27%, 0.48%, 0.49%, and 0.56%, respectively, and the BIC ratios of the machined-surface and surface-treated implants did not significantly differ (p=0.4826).
In the four-week subgroup, the BIC ratios in the machined-, RBM-, Cellnest-, and CMP-coated- surface implants were 0.10%, 0.74%, 0.68%, and 0.73%, respectively, and the BIC ratios of the machined-surface and surface-treated implants sig- nificantly differed (p=0.0063) (Table 3, Fig. 9).
Table 2. Compact bone contact ratios of the implants
Implant 2 weeks 4 weeks
Machined-surface 0.05 0.06
RBM-surface 0.23* 0.45*
Cellnest-surface 0.35* 0.39*
CMP-coated-surface 0.26* 0.58*
*Significant difference at the 0.05 level between groups. RBM: resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
Fig. 8. Cortical bone contact ratios of the implants. RBM:
resorbable blasting media, CMP: calcium meta phosphate.
*Significant difference at the 0.05 level between groups.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
3) Bone area ratios in the cancellous bone
In the two-week subgroup, the bone area ratios in the area within 200 μm of the surface of the implant in the machined-, RBM-, Cellnest-, and CMP- coated-surface implants were 0.68%, 0.68%, 0.69%, and 0.67%, respectively, and the bone area ratios of the different surface-treated implants did not signifi- cantly differ (p=0.9989). In the four-week subgroup,
the bone ratios in the machined-, RBM-, Cellnest-, and CMP-coated-surface implants were 0.53%, 0.84%, 0.76%, and 0.73%, respectively, and the bone ratios of the machined-surface and surface-treated implants significantly differed (p=0.0369) (Table 4, Fig. 10).
Table 3. Marrow bone contact ratios of the implants
Implant 2 weeks 4 weeks
Machined-surface 0.27 0.10
RBM-surface 0.48 0.74*
Cellnest-surface 0.49 0.68*
CMP-coated-surface 0.56 0.73*
*Significant difference at the 0.05 level between groups. RBM: resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
Table 4. Compact bone area ratios of the implants
Implant 2 weeks 4 weeks
Machined-surface 0.68 0.53
RBM-surface 0.68 0.84*
Cellnest-surface 0.69 0.76*
CMP-coated-surface 0.67 0.73*
*Significant difference at the 0.05 level between groups. RBM: resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
Fig. 9. Marrow bone contact ratio of the implants. RBM:
resorbable blasting media, CMP: calcium meta phosphate.
*Significant difference at the 0.05 level between groups.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
Fig. 10. Compact bone area ratios of the implants. RBM:
resorbable blasting media, CMP: calcium meta phosphate.
*Significant difference at the 0.05 level between groups.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
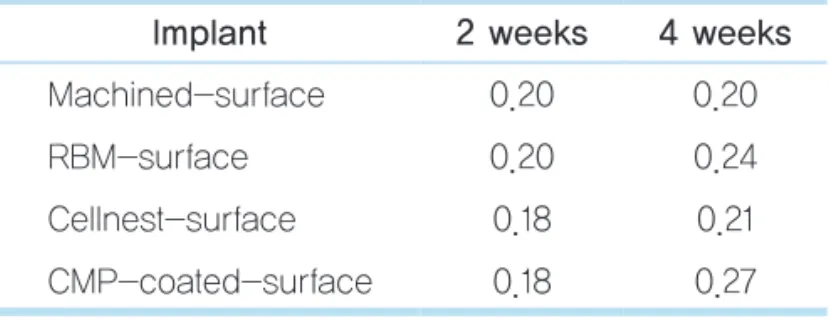
4) Bone area ratios in the cancellous bone
In the two-week subgroup, the bone area ratios in the machined-, RBM-, Cellnest-, and CMP-coated- surface implants were 0.20%, 0.20%, 0.18%, and 0.18%, respectively, and the bone area ratios of the machined-surface and surface-treated implants did not significantly differ (p=0.9844). In the four-week subgroup, the bone area ratios in the machined-, RBM-, Cellnest-, and CMP-coated-surface implants were 0.20%, 0.24%, 0.21%, and 0.27%, respectively,
and the bone area ratios of the various groups did not significantly differ, as in the two-week subgroup (p=0.7485) (Table 5, Fig. 11).
IV DISCUSSION
Osteoporosis is caused by the activation of the bone turnover due to the decreased gonadal steroids. In osteoporosis, the bone turnover is more intensive than the bone resorption, which leads to bone loss20. When the bone regeneration increases, the differentiation of osteoblasts increases. Proteins that reflect such increased proliferation include bone-specific alkaline phosphatase (BSAP) and osteocalcin21.
From a biological viewpoint, most studies that inves- tigated and analyzed osteoblasts measured the activity of ALP as a marker of the early phase of differentia- tion22,23. In this study, the blood ALP level was mea- sured to investigate the induction of osteoporosis. The mean ALP level in the normal control group was 76 IU/L, and in the group wherein osteoporosis was induced, 91.8 IU/L. These figures indicate increased activity of the osteoblasts that reflect bone regenera- tion. It is believed that this increased activity of the osteoblasts suggests increasing bone turnover due to osteoporosis. In the rats that underwent ovariectomy, mature bones developed poorly and fracture healing was delayed. These were because the estrogen defi- ciency due to the ovariectomy influenced the bone marrow stem cells, which deformed the osteoblasts and the osteoclasts and reduced the maximum bone Table 5. Marrow bone area ratios of the implants
Implant 2 weeks 4 weeks
Machined-surface 0.20 0.20
RBM-surface 0.20 0.24
Cellnest-surface 0.18 0.21
CMP-coated-surface 0.18 0.27
RBM: resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
Fig. 11. Marrow bone area ratios of the implants. RBM:
resorbable blasting media, CMP: calcium meta phosphate.
Jeong-Yol Lee et al. : Bone Tissue Reaction on Implant Surfaces in Osteoporotic Rats.
Implantology 2012
weight-bearing capability and reduced the bone vol- ume9. Numerous recent studies showed that in osteo- porosis, the amount of the cancellous bone around the implant and the contact between the implant and the newly formed bone could significantly decrease10,24,25. In this study, similar histological changes in the bone were observed two weeks after the implantation.
Compared with the normal control group, in the group where osteoporosis was induced, the amount of newly formed bone on the interface of the implant and the bone was small and osteoporotic deformation was observed in the newly formed bone tissues. Besides, the BIC ratio and the bone density around the implant decreased. Thus, it is believed that osteoporosis could be a risk factor for the initial stability of an implant, which is the most important factor of the success of an implant. In various edentulous jaws, the bone quantity and quality are important for achieving a satisfactory success rate in implant treatment26. Jaffin and Berman27 reported that in the type IV bone, the failure rate increased to up to 40% in the five-year follow-up due to the delayed initial stability because of the lack of close contact between the implant and the bone on account of the wide area of the medullary cavity.
Glauser et al.28 reported that soft bones are affected more by the implant design and the surface treatment.
To improve the success rate of implants in sites with poor bone quality and quantity, studies have been performed on implant surface treatment methods and surface characteristics29-31. The implant surface has been regarded as important for achieving osseo-inte- gration11, and intensive efforts have been made since the 1980s to improve the implant surface so as to
achieve initial stability and a favorable BIC ratio32,33. Buser et al.33 reported that a difference in the sur- face characteristics could lead to a difference in the contact between the host cells and the surrounding substrates, which could adversely affect the clinical outcomes. Davies34 reported that the implant surface treatment methods influenced the cellular activities of the osseous tissues around the implant. Larsson et al.35 reported that the surface roughness was closely correlated with the bone formation, and that a surface roughness of about 1.5 μm resulted in the best bone reaction36. In this study, the surface roughness values of the machined-, RBM-, Cellnest-, and CMP-coated- surface implants were 0.2, 1.2, 0.8, and 1.0 μm, respectively, and the roughness values of the anodic- oxidized- and Cellnest-surface implants differed from those reported by Larsson et al.35 but had a high BIC ratio. In this study, the characteristics of the initial process of ossification that resulted from the surface treatment methods and the slow bone formation due to osteoporosis were well-shown. In the 1.2 μm RBM implant, the initial ossification was found to have started on the rough surface of the implant. In partic- ular, in the cancellous bone, the osteoid formation started on the rough surface of the implant, and it was well-observed that as the ossification proceeded, the osteoids fused together to form new bones on the implant surface. Thus, it is believed that in osteoporo- sis, implants with suitable roughness can be more advantageous for the adhesion of oseteocytes, and the increase in the bone formation due to a rough surface was greater in the cancellous bone than in the compact bone. In this study, in the machined-surface implants,
microgaps were observed in the interface of the newly formed bone and the implant in many parts of the compact and cancellous bones, and this is attributed to the low wettability of the machined-surface implant.
Zechner et al.37 also implanted machined-, anodic- oxidized-, and HA-coated-surface implants, observed the histological changes in the bone tissues, and reported that in the machined-surface implants, the BIC had a finger-like (pseudopoidal) pattern and a microgap between the implant and the newly formed bone, although in the rough-surface implants, a broad-based (wallpaper-like) BIC was observed with- out a microgap. In this study, the anodic-oxidized- and Cellnest-surface implants showed ossification patterns that were similar to that reported by Zechner et al.37, and particularly showed thin and long ossifi- cation in progress on the surface of the implant in the cancellous bone. This is considered similar to the wall- paper-like patterns reported by Zechner et al.37 The CMP-coated surface was first treated with the RBM surface treatment method and then coated with calci- um metaphosphate. In the CMP-coated surface in this study, the ossification started around the coated par- ticles both in the compact bone and the cancellous bone, and proceeded on the surface of the implant. In this ossification, it was as if the histological findings on the anodic-oxidized- or Cellnest-surface implants were added to the histological findings on the RBM- surface implant.
In addition, in many parts of the CMP-coated- surface implants, red blood cells were observed, which was considered to have been due to the bioactivity capacity of calcium potassium and calcium metaphos-
phate. The test showed that the BIC ratio was lower in the machined-surface implant than in the surface- treated implants, and that the BIC ratios in the can- cellous bones in the machined-surface and surface- treated implants did not significantly differ two weeks after the implantation but significantly differed four weeks after the implantation. It is believed that in osteoporosis, surface-treated implants could be help- ful for osseo-integration because the amount of new bones in contact with the surface of the implant increases more in surface-treated implants than in machined-surface implants, and that this beneficial effect will increase over the time after the implanta- tion. The bone area ratios of the machined-surface and surface-treated implants significantly differed only in the compact bone four weeks after the implan- tation (p<0.05). This is deemed to be because the test periods in this study were relatively short (two and four weeks) and the bone formation was slow due to osteoporosis. Piattelli et al.38 performed a test to com- pare the bone reactions of machined- and RBM- surface implants, and reported that the bone contact was statistically greater with the RBM-surface implants than with the machined-surface implants.
The RBM-surface implants that were used in this study were roughened by spraying hydroxyapatite powder with a high pressure onto the machined sur- face of the titanium. Two and four weeks after the implantation, the BIC ratios in the compact and can- cellous bones were higher with the RBM-surface implants than with the machined-surface implants. In particular, the BIC ratios with the RBM-surface implants considerably increased in the cancellous bone
two and four weeks after the implantation. Thus, RBM-surface implants are believed to be helpful for maintaining the implants in the cancellous bone. The BIC ratios of the Cellnest- and machined-surface implants did not show any difference two weeks after their implantation, but significantly increased four weeks after their implantation. Thus, they were expected to contribute to the stability of the implants.
In addition, the CMP-coated-surface implants also resulted in higher BIC ratios and bone area ratios than the machined-surface implants. Two weeks after the implantation of the CMP-coated-surface implants, the BIC ratio in the cancellous bone became higher than that with the other surface-treated implants, though not significantly, which suggests that in osteoporosis, such bioactive surfaces as CMP-coated surfaces are likely to induce faster bone growth than other surface treatment methods. Taken together, although this study has such limitations as a small number of speci- mens per group and different types and sizes of implants from those used in clinical practice, it showed that surface-treated implants can be more helpful for ensuring long-term stability of implants than machined-surface implants in patients with poor bone quality. It is particularly believed that in osteoporosis patients, surface-treated implants can be more advantageous for the initial osseointegration.
참고문헌
1. Eddy DM, Johnston CC, Cummings SR, et al. Osteoporosis: review of
the evidence for prevention, diagnosis, and treatment and cost- effectiveness analysis. Status report. Osteoporos Int. 1998; 4(suppl):
1-80.
2. Eastell R. Treatment of postmenopausal osteoporosis. N Engl J Med.
1998; 338: 736-746.
3. Yamazaki M, Shirota T, Tokugawa Y, et al. Bone reactions to titanium screw implants in ovariectomized animals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87: 411-418.
4. Hohlweg-Majert B, Schmelzeisen R, Pfeiffer BM, et al. Significance of osteoporosis in craniomaxillofacial surgery: a review of the literature.
Osteoporos Int. 2006; 17: 167-179.
5. White SC. Oral radiographic predictors of osteoporosis.
Dentomaxillofac Radiol. 2002; 31: 84-92.
6. von Wowern N, Kollerup G. Symptomatic osteoporosis: a risk factor for residual ridge reduction of the jaws. J Prosthet Dent. 1992; 67: 656-660.
7. Bryant SR. The effects of age, jaw site, and bone condition on oral implant outcomes. Int J Prosthodont. 1998; 11: 470-490.
8. Okamura A, Ayukawa Y, Iyama S, et al. Effect of the difference of bone turnover on peri-titanium implant osteogenesis in ovariectomized rats. J Biomed Mater Res A. 2004; 70: 497-505.
9. Ozawa S, Ogawa T, Iida K, et al. Ovariectomy hinders the early stage of bone-implant integration: histomorphometric, biomechanical, and molecular analyses. Bone. 2002; 30: 137-143.
10. Qi MC, Zhou XQ, Hu J, et al. Oestrogen replacement therapy promotes bone healing around dental implants in osteoporotic rats. Int J Oral Maxillofac Surg. 2004; 33: 279-285.
11. Albrektsson T, Brånemark PI, Hansson HA, et al. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop Scand. 1981; 52: 155- 170.
12. Sennerby L, Thomsen P, Ericson LE. Early bone tissue responsed to titanium implants inserted in rabbit cortical and cancellous bone. Int J Oral Maxillofac Implants. 1992; 7: 62-71.
13. Wennerberg A, Albrektsson T, Andersson B. Design and surface characteristics of 13 commercially available oral implant systems. Int J Oral Maxillofac Implants. 1993; 8: 622-633.
14. Albrektsson T, Wennerberg A. Oral implant surfaces: part 2--review focusing on clinical knowledge of different surfaces. Int J Prosthodont.
2004; 17: 544-564.
15. Larsson C, Thomsen P, Aronsson BO, et al. Bone response to surface- modified titanium implants: studies on the early tissue response to
machined and electropolished implants with different oxide thicknesses.
Biomaterials. 1996; 17: 605-616.
16. Yoshinari M, Ohtsuka Y, Dérand T. Thin hydroxyapatite coating produced by the ion beam dynamic mixing method. Biomaterials. 1994;
15: 529-535.
17. LeGeros RZ. Properties of osteoconductive biomaterials: calcium phosphates. Clin Orthop Relat Res. 2002; 395: 81-98.
18. Lee H, Kim SG, Kim BK, et al. An animal study on CMP: calcium meta phosphate coated implant in rabbits. The Quintessence. 2004; 9: 1-6.
19. Chang DW, Park JB, Kwon YH, et al. Micromophometric change of implant surface conditioned with tetracycline-HCL: FBR(R) and CellNest surface. J Korean Acad Periodontol. 2006; 36: 717-729.
20. Riggs BL, Khosla S, Melton LJ 3rd. A unitary model for involutional osteoporosis: estrogen deficiency causes both type I and type II osteoporosis in postmenopausal women and contributes to bone loss in aging men. J Bone Miner Res. 1998; 13: 763-773.
21. Sørensen MG, Henriksen K, Schaller S, et al. Biochemical markers in preclinical models of osteoporosis. Biomarkers. 2007; 12: 266-286.
22. Midy V, Plouët J. Vasculotropin/vascular endothelial growth factor induces differentiation in cultured osteoblasts. Biochem Biophys Res Commun. 1994; 199: 380-386.
23. Shui C, Scutt A. Mild heat shock induces proliferation, alkaline phosphatase activity, and mineralization in human bone marrow stromal cells and Mg-63 cells in vitro. J Bone Miner Res. 2001; 16: 731-741.
24. Motohashi M, Shirota T, Tokugawa Y, et al. Bone reactions around hydroxyapatite-coated implants in ovariectomized rats. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87: 145-152.
25. Lugero GG, de Falco Caparbo V, Guzzo ML, et al. Histomorphometric evaluation of titanium implants in osteoporotic rabbits. Implant Dent.
2000; 9: 303-309.
26. Albrektsson T, Dahl E, Enbom L, et al. Osseointegrated oral implants. A Swedish multicenter study of 8139 consecutively inserted Nobelpharma implants. J Periodontol. 1988; 59: 287-296.
27. Jaffin RA, Berman CL. The excessive loss of Branemark fixtures in type
IV bone: a 5-year analysis. J Periodontol. 1991; 62: 2-4.
28. Glauser R, Portmann M, Ruhstaller P. Initial implant stability using different implant designs and surgical techniques. Applied Osseointegration Research. 2001; 2: 6-8.
29. Cooper LF. A role for surface topography in creating and maintaining bone at titanium endosseous implants. J Prosthet Dent. 2000; 84: 522- 534.
30. Gonshor A, Goveia G, Sotirakis E. A prospective, multicenter, 4-year study of the ACE Surgical resorbable blast media implant. J Oral Implantol. 2003; 29: 174-180.
31. Wheeler SL. Eight-year clinical retrospective study of titanium plasma- sprayed and hydroxyapatite-coated cylinder implants. Int J Oral Maxillofac Implants. 1996; 11: 340-350.
32. Gotfredsen K, Wennerberg A, Johansson C, et al. Anchorage of TiO2- blasted, HA-coated, and machined implants: an experimental study with rabbits. J Biomed Mater Res. 1995; 29: 1223-1231.
33. Buser D, Broggini N, Wieland M, et al. Enhanced bone apposition to a chemically modified SLA titanium surface. J Dent Res 2004; 83: 529- 533.
34. Davies JE. Mechanisms of endosseous integration. Int J Prosthodont.
1998; 11: 391-401.
35. Larsson C, Thomsen P, Lausmaa J, et al. Bone response to surface modified titanium implants: studies on electropolished implants with different oxide thicknesses and morphology. Biomaterials. 1994; 15:
1062-1074.
36. Albrektsson T, Wennerberg A. Oral implant surfaces: part 1--review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int J Prosthodont. 2004; 17: 536-543.
37. Zechner W, Tangl S, Fürst G, et al. Osseous healing characteristics of three different implant types. Clin Oral Implants Res. 2003; 14: 150-157.
38. Piattelli M, Scarano A, Paolantonio M, et al. Bone response to machined and resorbable blast material titanium implants: an experimental study in rabbits. J Oral Implantol. 2002; 28: 2-8.