Background : Treatment experiences with antiviral agents against MERS-CoV (Middle East Respiratory Syndrome Coronavirus) infection are limited, and there is lack of information regarding adverse drug reactions (ADRs) in this patient group. In 2015, we evaluated the ADRs of antiviral treatment against MERS-CoV infections in one tertiary teaching hospital in South Korea.
Methods : Between May 20th and July 20th 2015, a retrospective chart review was conducted to evaluate any ADRs. We focused on three antiviral agents: ribavirin, peginterferon alpha2a and lopinavir/ritonavir. Laboratory data and clinical implications of ADRs were collected through elec- tronic medical records. The ADRs were evaluated and cross checked by three independent pharma- cists.
Results : Totally, 28 patients were evaluated, and 15 ADRs were detected. Ribavirin was the most causative agent. Hematologic ADRs were the maximum reported, and nausea/vomiting was second ranked. Seven ADRs were scored as Grade 3 severity of ADRs, as per the CTCAE ver. 4.0; the causative drug was discontinued in 9 cases. Causality scores using WHO-UMC and Naranjo scale
중동 호흡기 증후군 치료에 사용한 항바이러스제의 약물이상반응 발현양상 분석
박소진, 손유민, 박효정
�, 인용원, 이수미, 이용석, 이영미 삼성서울병원 약제부
Evaluation of Adverse Drug Reaction of Antiviral Therapy for Middle East Respiratory Syndrome Coronavirus Infection
So Jin Park, You Min Sohn, Hyo Jung Park
�, Yong Won In, Su Mi Lee, Yong Seok Lee and Young Mee Lee
Department of Pharmaceutical Services, Samsung Medical Center, 81 Irwon-ro, Gangnam-gu, Seoul, 06351, Republic of Korea
투고일자 2016.12.30; 심사완료일자 2017.1.26; 게재확정일자 2017.6.10
�교신저자 박효정 Tel:02-3410-6091 E-mail:[email protected]
Original Article
indicated that most of the ADR cases had a ‘possible’relationship.
Conclusion : ADR patterns of the three drugs evaluated for MERS-CoV patients were mostly similar with the limited existing reports.
[Key words] MERS-CoV, ADR (adverse drug reaction), Antiviral therapy
연구배경
2015년 중동호흡기 증후군(Middle East Respiratory Syndrome, MERS) 유행 시 삼성서울병원 입원환자의 치료제로 사용된 항바이러스제는 대한감염학회 지침에 따라 ribavirin, pegylated interferon alpha2a, lopinavir/ritonavir로 구성되었다.
1)MERS에 대해 확 립된 치료제가 아직 없는 만큼 상기 약제들의 사용경험 이 제한적이고, 약제 각각의 monograph 에 기술된 약 물 이상반응(adverse drug reaction, ADR) 정보는 대 부분 C형 간염이나 후천성 면역결핍증후군(HIV) 환자 군을 대상으로 하고 있다.일부 급성 호흡기 증후군 (severe acute respiratory syndrome, SARS) 환자 군에서 상기 약제들의 약물 이상반응 발현양상이 논문 으로 보고되어있지만, MERS 환자에서의 사례보고는 매우 드물다.
2)-7)따라서 본 연구에서 ribavirin, pegy- lated interferon alpha2a, lopinavir/ritonavir을 MERS 치료에 사용하였을 때, 약물 이상반응 발현 양 상을 분석해보고, 기존의 약제사용에서 보고된 약물 이 상반응 양상과의 차이를 확인해 봄으로써, 추후 유사한 임상상황에서 약물 이상반응 평가와 해석에 도움이 되 고자 하였다.
연구방법 1. 분석 대상
본 연구는 삼성서울병원 입원환자 중 2015.05.20~
2015.07.20 사이의 기간에 ribavirin(바이라미드
�200 mg, 일성신약), peginterferon alpha2a (페가시 스 주
�180 mcg 프로클릭, 또는 페가시스프리필드 주
�135 mcg, 로슈), lopinavir/ritonavir(칼레트라정
�200/50 mg, 한국애브비) 3제가 모두 처방되었던 환자 명단을 바탕으로 투여일수는 관계없이 투약력이 한번 이라도 있고 약물이상반응을 평가할 수 있을만 한 의무 기록이 존재하면 연구대상에 포함시켰다. 평가 불가한 정도의 기록 미비, 전자차트 열람이 금지된 환자와, 적 응증이 MERS 의심 또는 확진이 아닌 다른 virus 감염 이 확실한 경우(human immunodeficiency virus 등) 는 분석대상에서 제외하였다. MERS 확진은 상병명에 MERS 가 포함되어 있고, PCR 2회 이상 양성인 경우 로 정의하였다.
2. 자료 수집
3제 약제를 사용한 전체 환자 명단과 각 환자에 대한 약물 투약력, 혈액을 포함한 각종 검사결과, 기저질환, 임상경과, 약물이상반응 발현내용 등에 관한 모든 사항 은 삼성서울병원 통합의료시스템을 통해 수집하였다.
약물이상반응을 인지하기 위한 검사결과 항목으로는 hemoglobin (Hgb), white blood cell (WBC), absolute neutrophil count (ANC), platelet (PLT), reticulocyte, total bilirubin, aspartate transami- nase (AST), alanine transaminase (ALT), gam- maglutamyl transferase (GGT), triglyceride, amylase, lipase, glucose level, lactate dehydro- genase (LD), serum creatinine (Scr)을 필수적으로 검토하여 비정상적인 수치 보고가 있는지 확인하였고 이외의 혈액검사결과 수치 및 각종 검사 결과를 해석하 여 약제와 연관성이 있는 유의한 변화가 있는지 분석하 였다.
아나필락시스 증상, 피부 및 피하조직, 정신신경계,
심혈관계, 호흡기계 이상반응은 검사 결과로 인지가 어 려운 경우가 많아 전자의무기록 상의 의사 경과기록 및 간호기록, 그리고 약무기록에 약물 이상반응 관련 언급 을 중점적으로 재평가 하였다. 위장관계 이상반응은 대 변 횟수 및 양상과 오심, 구토 기록을 수집하였다.
본 연구는 후향적 연구이나, MERS 유행기간 이었던 연구대상 기간 중에 약사가 매일 중환자의학과의 MERS 환자 진료 회진에 참석하여 의료진과 논의한 내 용 등을 실시간으로 기록한 약무 기록이 있어 이를 함 께 참고하였다. 연구 진행에 필요한 모든 절차는 삼성 서울병원 기관윤리심의사무국의 허가를 받았으며 후향 적 연구로 동의서 면제로 진행되었다(IRB No. 2015-
11-142).
3. 분석 항목 및 방법
분석대상 환자군 중 약물이상반응이 나타난 비율을 산정하였고 세부적으로 약제별, 증상별 분포와 허가사
항
8)-11)기 반영 여부를 정리하였다. 하나의 약물이상반
응 증상에 둘 이상의 약제를 원인약제로 의심할 수 있 으므로 중복산정을 허용하였다. 또한 약물이상반응 의 심 건에 대해서 World Health Organization- Uppsala Monitoring Centre(WHO-UMC) scale,
12)Naranjo scale
13)을 이용하여 인과성 평가를 시행하였
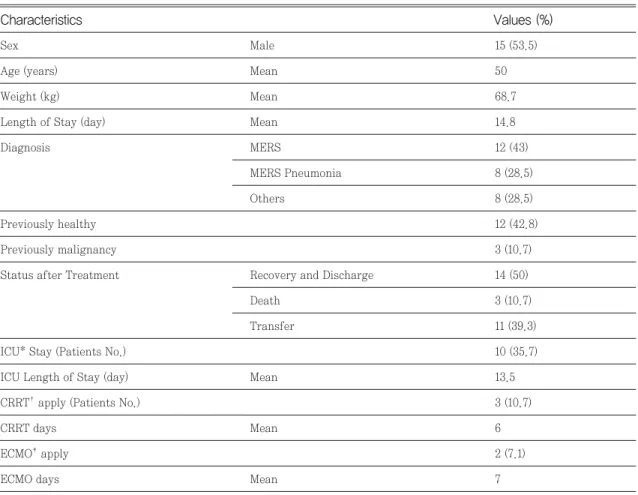
*ICU: Intensive Care Unit,
�CRRT: Continuous Renal Replacement Therapy,
�ECMO: Extra-Corporeal Membrane Oxygenation
Sex Male 15 (53.5)
Age (years) Mean 50
Weight (kg) Mean 68.7
Length of Stay (day) Mean 14.8
Diagnosis MERS 12 (43)
MERS Pneumonia 8 (28.5)
Others 8 (28.5)
Previously healthy 12 (42.8)
Previously malignancy 3 (10.7)
Status after Treatment Recovery and Discharge 14 (50)
Death 3 (10.7)
Transfer 11 (39.3)
ICU* Stay (Patients No.) 10 (35.7)
ICU Length of Stay (day) Mean 13.5
CRRT�apply (Patients No.) 3 (10.7)
CRRT days Mean 6
ECMO�apply 2 (7.1)
ECMO days Mean 7
Values (%) Characteristics
Table 1. Baseline characteristics of patients (n=28)
고 증상의 중증도는 미국 국립 보건원에서 발행하는 Common Terminology Criteria for Adverse Events (CTCAE) version 4.0
14)을 기준으로 분류하였 다. 약물이상반응을 인지한 후 조치와 총 약물 이상반
응 건수 중 중환자실에서 발생한 건수를 구분하였다.
약물이상반응으로 판단한 경우에는 의심 약제 투여 시작일로부터 첫 증상발현까지 걸리는 시간, 검사결과 로 알 수 있는 경우 가장 악화되는 시점, 검사 수치 등
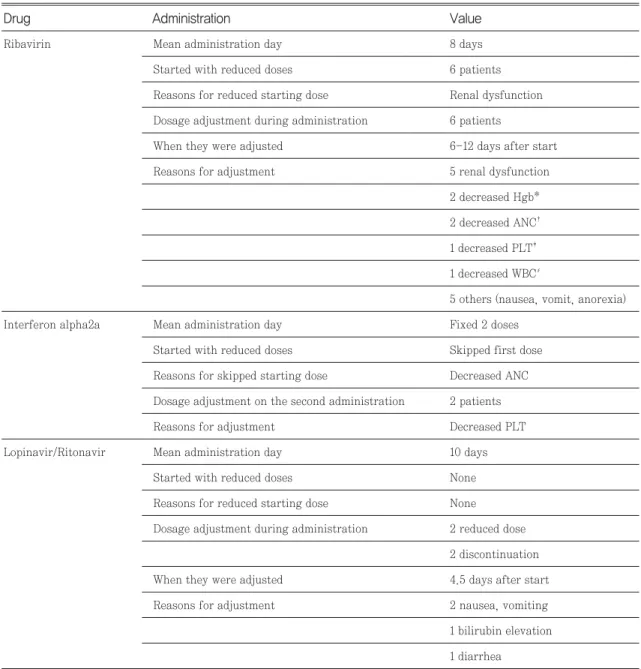
*Hgb: Hemoglobin,
�ANC: Absolute Neutrophil Count,
�PLT: Platelet,
∮WBC: White Blood Cell
Ribavirin Mean administration day 8 days
Started with reduced doses 6 patients
Reasons for reduced starting dose Renal dysfunction Dosage adjustment during administration 6 patients
When they were adjusted 6-12 days after start
Reasons for adjustment 5 renal dysfunction
2 decreased Hgb*
2 decreased ANC� 1 decreased PLT� 1 decreased WBC∮
5 others (nausea, vomit, anorexia)
Interferon alpha2a Mean administration day Fixed 2 doses
Started with reduced doses Skipped first dose Reasons for skipped starting dose Decreased ANC Dosage adjustment on the second administration 2 patients
Reasons for adjustment Decreased PLT
Lopinavir/Ritonavir Mean administration day 10 days
Started with reduced doses None
Reasons for reduced starting dose None Dosage adjustment during administration 2 reduced dose
2 discontinuation
When they were adjusted 4.5 days after start
Reasons for adjustment 2 nausea, vomiting
1 bilirubin elevation 1 diarrhea
Administration Value
Drug
Table 2. Administration of antiviral agents and regimen modification patterns (n=28)
이 기저치에 비해 가장 악화된 정도(기저치 대비의 WBC 감소폭 등), 약제 감량 또는 중단으로부터 증상 회복세로 돌아서기까지 걸리는 시간 등을 기술하고자
하였다.
본 연구에서는 적은 연구대상 환자수로 인해, 별도의 통계검정 등은 사용하지 않았고 모든 결과는 기술적으
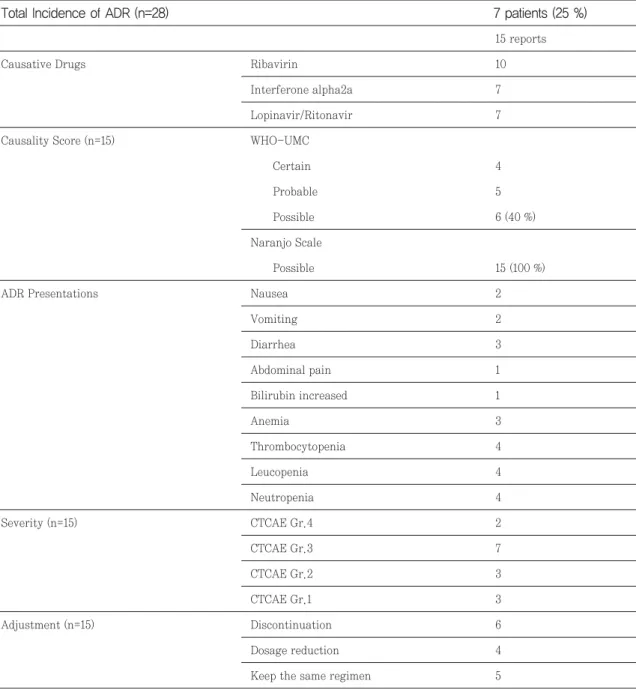
*WHO-UMC: World Health Organization-Uppsala Monitoring Centre,
�CTCAE: Common Terminology Criteria for Adverse Events
15 reports
Causative Drugs Ribavirin 10
Interferone alpha2a 7
Lopinavir/Ritonavir 7
Causality Score (n=15) WHO-UMC
Certain 4
Probable 5
Possible 6 (40 %)
Naranjo Scale
Possible 15 (100 %)
ADR Presentations Nausea 2
Vomiting 2
Diarrhea 3
Abdominal pain 1
Bilirubin increased 1
Anemia 3
Thrombocytopenia 4
Leucopenia 4
Neutropenia 4
Severity (n=15) CTCAE Gr.4 2
CTCAE Gr.3 7
CTCAE Gr.2 3
CTCAE Gr.1 3
Adjustment (n=15) Discontinuation 6
Dosage reduction 4
Keep the same regimen 5