J Health Tech Assess 2016;4(2):35-43 ISSN 2288-5811 Copyright © 2016 The Korean Association for Health Technology Assessment
서 론
의약품 사용 오류(medication error)는 유해 사례(adverse event)와 함께 환자 안전을 위협하는 주요한 요인이다. 중환 자실의 의약품 사용 오류 발생률에 관하여 체계적으로 문헌 을 고찰한 연구에 따르면, 1000 patient-days당 8.1~2344건 의 의약품 사용 오류가 발생한 것으로 나타났다.1) 이렇게 의 약품 사용 오류의 발생 편차가 큰 이유 중 하나로, 의약품 사 용 오류의 현황 연구에서 사용되는 유해 사례와 의약품 사 용오류에 대한 표준화된 정의가 없다는 점이 제시되었다. 이 처럼, 의약품 사용 오류의 현황을 정확하게 파악하기 위해서 는 표준화된 정의가 반드시 필요하다.
또한 의약품 사용 오류를 원인, 유형, 심각도 등에 따라 분 류하게 되면, 의약품 사용 오류가 발생한 단계와 그 심각도 를 알 수 있다. 이를 통해 의약품 사용 과정을 개선하거나 의
약품 사용 오류의 재발을 최소화할 방안을 개발할 수 있으 므로, 효과적으로 의약품 사용 오류를 감소시키기 위해서는 표준화된 분류 유형이 마련되어야 한다.2)
현재 우리나라에서는 의약품 사용 오류를 지칭하는 용어 조차 통일되지 못하여 의약전문가 사이에서 의약품 사용 과 오, 투약 오류 등 다양한 용어로 지칭되고 있다.2-4) 의약품 사용 오류의 국문 정의는 보건복지부의 “의약품 사용 과오 (medication error) 예방을 위한 가이드라인”에 다음과 같이 제시되어 있다.
“의료전문인, 환자, 소비자의 관리하에 의약품 투여가 진 행될 때에 부적절한 의약품 사용이 이루어지거나 환자에게 해가 되는 모든 예방이 가능한 사건.”5)
보건복지부의 정의는 미국 National Coordinating Council for Medication Error Reporting and Prevention(이하, NCC MERP)의 정의를 국문으로 번역한 것이다. 함께 제시된 의
The Analysis of Definition and Types for Medication Error Used in Foreign Countries
Siin Kim, Sola Han, and Hae Sun Suh
College of Pharmacy, Pusan National University, Busan, Korea
의약품 사용 오류의 정의 및 분류 유형에 대한 국외 현황 분석
부산대학교 약학대학
김시인·한솔아·서혜선
Received October 16, 2015 Revised November 21, 2016 Accepted November 29, 2016 Address for Correspondence:
Hae Sun Suh College of Pharmacy, Pusan National University, 2 Busandaehak-ro, 63beon-gil, Geumjeong-gu, Busan 46241, Korea Tel: +82-51-510-2528
Fax: +82-51-513-6754 E-mail: [email protected]
Objectives: To analyze the current status of definition and types of medication error used in sev- eral countries. Methods: Systematic search and analyses were performed to investigate the defini- tion and types of medication error used in patient safety organizations in several countries includ- ing the United States, Europe, Australia, New Zealand, and Korea. Results: Twenty three organizations suggested a definition or a type of medication error. The most widely used definition for medication error was that of the National Coordinating Council for Medication Error Reporting and Preven- tion (NCC MERP). Types of medication error highly varied by organization. Types were classified by severity criteria, process criteria, activity criteria, and responsible person criteria. Severity and activ- ity criteria were used most frequently. The Ministry of Health & Welfare in Korea uses the definition of the NCC MERP, and the criteria suggested by the American Society of Health-System Pharma- cists for the types of medication error. Conclusion: Definitions of medication error are generally similar in most patient safety organizations, whereas types of medication error varied by organiza- tion. In part, this variation results from classification criteria for medication error.
Key Words Medication errors · Patient safety organization.
Review Article
JoHTA
약품 사용 오류의 분류 유형은 다음과 같다.
“처방 오류, 투여 누락, 투여시간 오류, 미승인 의약품 투 여, 용량 오류, 투여 방법 오류, 부적절한 의약품 모니터링, 유효기한 경과 의약품 투여, 환자의 복약이행 오류, 기타.”5)
2007년에 발간된 보건복지부 가이드라인은 의약품 사용
오류와 관련된 기본 개념, 예방 지침, 처리 지침 등을 자세히 다루고 있다. 현재 이 가이드라인 외에 국내 유관기관에서 의약품 사용 오류에 대해 자세히 고찰한 자료는 없다. 하지 만 실제 임상현장에서 보건복지부 가이드라인의 활용도는 크게 높지 않으며, 요양기관이 자체적으로 의약품 사용 오류
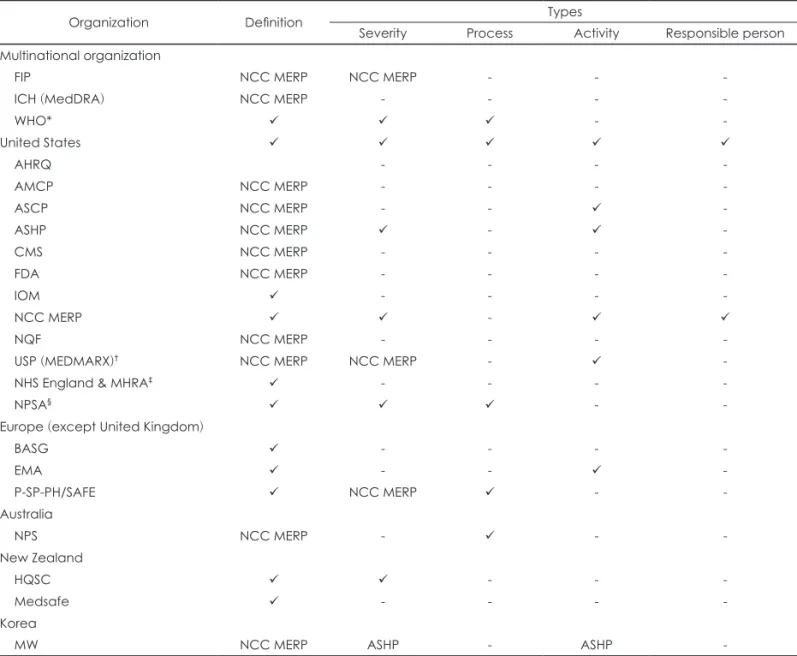
Table 1. Definitions and types of medication error suggested by patient safety organizations
Organization Definition Types
Severity Process Activity Responsible person Multinational organization
FIP NCC MERP NCC MERP - - -
ICH (MedDRA) NCC MERP - - - -
WHO* - -
United States
AHRQ - - - -
AMCP NCC MERP - - - -
ASCP NCC MERP - - -
ASHP NCC MERP - -
CMS NCC MERP - - - -
FDA NCC MERP - - - -
IOM - - - -
NCC MERP -
NQF NCC MERP - - - -
USP (MEDMARX)† NCC MERP NCC MERP - -
NHS England & MHRA‡ - - - -
NPSA§ - -
Europe (except United Kingdom)
BASG - - - -
EMA - - -
P-SP-PH/SAFE NCC MERP - -
Australia
NPS NCC MERP - - -
New Zealand
HQSC - - -
Medsafe - - - -
Korea
MW NCC MERP ASHP - ASHP -
The mark “” means that the organization suggests a definition or a type of medication error, corresponding to the column.
Among these, if any definition or type of an organization was completely same with that of another organization, the cell was marked as the name of organization considered to be origin of the concept. If the organization didn’t suggest any definition or type, corresponding to the column, the cell was marked as “-”. *WHO suggests the type for patient safety incident which is a su- perordinate concept to a medication error. Patient safety incident is defined as an event of circumstance that could have re- sulted, or did result, in unnecessary harm to a patient, †USP launched MEDMARX in 1998, and transferred all rights, ownership and management of the MEDMARX to Quantros in 2008, ‡NHS England and the MHRA jointly issued two patient safety alerts; one of them dealt with medication error, §NPSA suggests the type for patient safety incident which is a superordinate concept to a medication error. AHRQ: Agency for Healthcare Research and Quality’s, AMCP: Academy of Managed Care Pharmacy, ASCP:
American Society of Consultant Pharmacists, ASHP: American Society of Health-System Pharmacists, BASG: Austrian Federal Of- fice for Safety in Health Care (Bundesamt für Sicherheit im Gesundheitswesen), CMS: Centers for Medicare & Medicaid Services, EMA: European Medicines Agency, FDA: US Food and Drug Administration, FIP: International Pharmaceutical Federation, HQSC:
Health Quality & Safety Commission, ICH: International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use, IOM: Institute of Medicine, MHRA: Medicines and Healthcare products Regulatory Agency, MW: Ministry of Health & Welfare, NCC MERP: National Coordinating Council for Medication Error Reporting and Prevention, NHS:
National Health Service, NPS: National Prescribing Service Limited, NPSA: National Patient Safety Agency, P-SP-PH/SAFE: Expert Group on Safe Medication Practices, USP: US Pharmacopeial Convention, WHO: World Health Organization, NQF: National Qual- ity Forum
와 관련된 지침을 규정하여 사용하고 있는 경우가 많다.6) 이 연구에서는 국외에서 사용하고 있는 의약품 사용 오류 의 정의 및 분류 유형을 검토하여 우리나라에서 사용하기 적합한 의약품 사용 오류의 정의 및 분류 유형을 제안하는 데 필요한 기초 근거를 마련하고자 한다.
방 법
국외에서 사용하고 있는 의약품 사용 오류의 정의 및 분류
유형을 파악하기 위해 국외의 환자 안전(patient safety) 기관 에서 사용하고 있는 정의 및 분류 유형을 조사하였다. 조사 국가는 환자 안전 보고 시스템이 비교적 잘 구성되어, 유해 사례와 의약품 사용 오류의 수집을 활발히 하고 있는 미국, 유럽, 호주, 뉴질랜드로 한정하였고,6) 우리나라와의 비교를 위해 국내 기관도 조사하였다.
구글 웹사이트에서 키워드 검색을 시행하여 최대한 광범 위하게 자료를 수집하였다. 사용된 키워드는 “medication error”, “medication error defined”, “medication error defini- Table 2. Definitions of medication error classified according to keywords for definition
Organization Definition
‘Event’
HQSC “Medication errors are defined as any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional or patient.”7)
NCC MERP “A medication error is any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer.”8)
‘Failure’
WHO “A failure in the treatment process that leads to, or has the potential to lead to, harm to the patient.”9)
‘Error’
AHRQ “A medication error refers to an error (of commission or omission) at any step along the pathway that begins when a clinician prescribes a medication and ends when the patient actually receives the medication.”10) BASG “Medication errors are unintentional errors in the prescribing, dispensing, administration or monitoring of
a medicine while under the control of a healthcare professional, patient or consumer.”11) EMA “Medication error refers to any unintentional error in the prescribing, dispensing, or administration
of a medicinal product while in the control of the healthcare professional, patient or consumer.”12,13) IOM “Any error occurring in the medication-use process (Bates et al., 1995a). Examples include wrong dosage
prescribed, wrong dosage administered for a prescribed medication, or failure to give (by the provider) or take (by the patient) a medication.”14)
Medsafe “Any unintentional error in the process of prescribing, preparing, dispensing, administering or clinical monitoring of a medicine or vaccine while under the control of a healthcare professional, patient or consumer.”15)
‘Mistake’
EMA “Medication errors are unintended mistakes in the prescribing, dispensing and administration of a medicine that could cause harm to a patient.”16)
‘Deviation’
P-SP-PH/SAFE “A medication error is any deviation from ordinary standards of care appropriate for the time of the medicine therapy of a patient. A medication error is a non-intentional omission or failed activity related to the medication use system, which can be the cause of a risk or of an adverse event reaching the patient.”17)
‘Incident’
NHS England &
MHRA*
“Medication errors are any PSI†s where there has been an error in the process of prescribing, preparing, dispensing, administering, monitoring or providing advice on medicines.”18)
NPSA “Medication errors can be defined as patient safety incidents involving medicines in which there has been an error in the process of prescribing, dispensing, preparing, administering, monitoring, or providing medicine advice, regardless of whether any harm occurred.”19)
*NHS England and the MHRA jointly issued two patient safety alerts; one of them dealt with medication error, †PSI was defined as any unintended or unexpected incident, which could have or did lead to harm for one or more patients receiving NHS care.
AHRQ: Agency for Healthcare Research and Quality’s, BASG: Austrian Federal Office for Safety in Health Care (Bundesamt für Si- cherheit im Gesundheitswesen), EMA: European Medicines Agency, HQSC: Health Quality & Safety Commission, MHRA: Medi- cines and Healthcare products Regulatory Agency, NCC MERP: National Coordinating Council for Medication Error Reporting and Prevention, NHS: National Health Service, NPSA: National Patient Safety Agency, PSI: patient safety incident, P-SP-PH/SAFE:
Expert Group on Safe Medication Practices, WHO: World Health Organization, IOM: Institute of Medicine
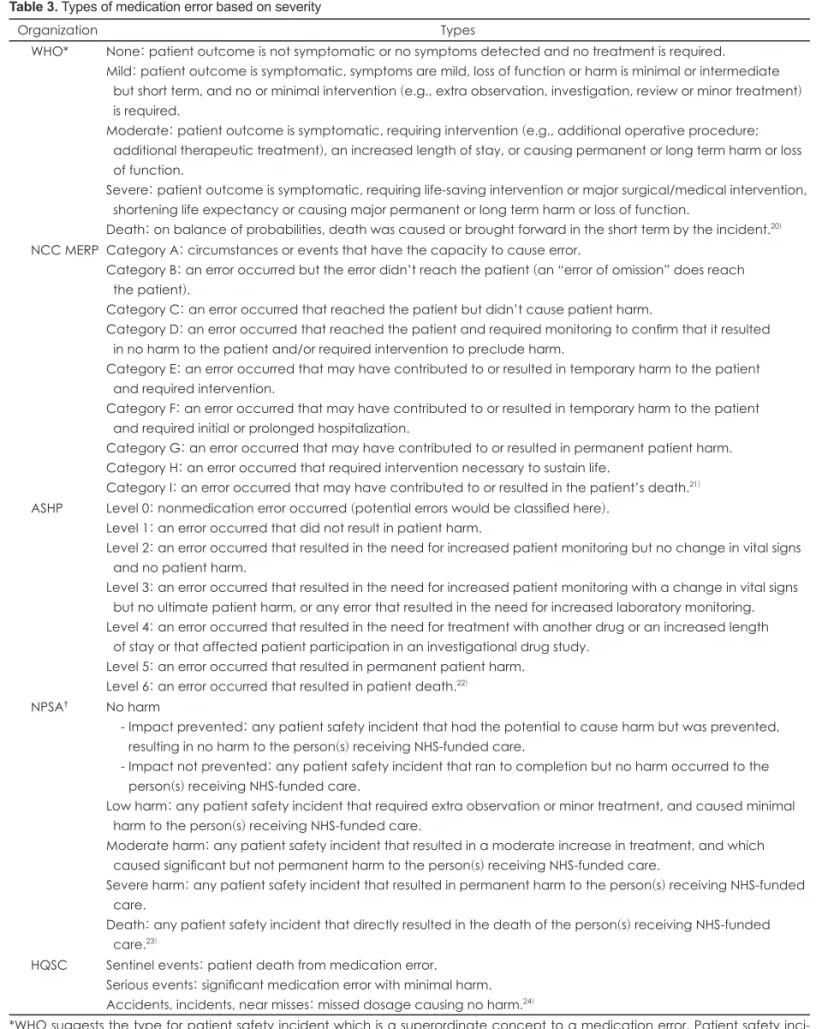
Table 3. Types of medication error based on severity
Organization Types
WHO* None: patient outcome is not symptomatic or no symptoms detected and no treatment is required.
Mild: patient outcome is symptomatic, symptoms are mild, loss of function or harm is minimal or intermediate but short term, and no or minimal intervention (e.g., extra observation, investigation, review or minor treatment) is required.
Moderate: patient outcome is symptomatic, requiring intervention (e.g., additional operative procedure;
additional therapeutic treatment), an increased length of stay, or causing permanent or long term harm or loss of function.
Severe: patient outcome is symptomatic, requiring life-saving intervention or major surgical/medical intervention, shortening life expectancy or causing major permanent or long term harm or loss of function.
Death: on balance of probabilities, death was caused or brought forward in the short term by the incident.20) NCC MERP Category A: circumstances or events that have the capacity to cause error.
Category B: an error occurred but the error didn’t reach the patient (an “error of omission” does reach the patient).
Category C: an error occurred that reached the patient but didn’t cause patient harm.
Category D: an error occurred that reached the patient and required monitoring to confirm that it resulted in no harm to the patient and/or required intervention to preclude harm.
Category E: an error occurred that may have contributed to or resulted in temporary harm to the patient and required intervention.
Category F: an error occurred that may have contributed to or resulted in temporary harm to the patient and required initial or prolonged hospitalization.
Category G: an error occurred that may have contributed to or resulted in permanent patient harm.
Category H: an error occurred that required intervention necessary to sustain life.
Category I: an error occurred that may have contributed to or resulted in the patient’s death.21) ASHP Level 0: nonmedication error occurred (potential errors would be classified here).
Level 1: an error occurred that did not result in patient harm.
Level 2: an error occurred that resulted in the need for increased patient monitoring but no change in vital signs and no patient harm.
Level 3: an error occurred that resulted in the need for increased patient monitoring with a change in vital signs but no ultimate patient harm, or any error that resulted in the need for increased laboratory monitoring.
Level 4: an error occurred that resulted in the need for treatment with another drug or an increased length of stay or that affected patient participation in an investigational drug study.
Level 5: an error occurred that resulted in permanent patient harm.
Level 6: an error occurred that resulted in patient death.22) NPSA† No harm
- Impact prevented: any patient safety incident that had the potential to cause harm but was prevented, resulting in no harm to the person(s) receiving NHS-funded care.
- Impact not prevented: any patient safety incident that ran to completion but no harm occurred to the person(s) receiving NHS-funded care.
Low harm: any patient safety incident that required extra observation or minor treatment, and caused minimal harm to the person(s) receiving NHS-funded care.
Moderate harm: any patient safety incident that resulted in a moderate increase in treatment, and which caused significant but not permanent harm to the person(s) receiving NHS-funded care.
Severe harm: any patient safety incident that resulted in permanent harm to the person(s) receiving NHS-funded care.
Death: any patient safety incident that directly resulted in the death of the person(s) receiving NHS-funded care.23)
HQSC Sentinel events: patient death from medication error.
Serious events: significant medication error with minimal harm.
Accidents, incidents, near misses: missed dosage causing no harm.24)
*WHO suggests the type for patient safety incident which is a superordinate concept to a medication error. Patient safety inci- dent is defined as an event of circumstance that could have resulted, or did result, in unnecessary harm to a patient, †NPSA sug- gests the type for patient safety incident which is a superordinate concept to a medication error. ASHP: American Society of Health-System Pharmacists, HQSC: Health Quality & Safety Commission, NCC MERP: National Coordinating Council for Medica- tion Error Reporting and Prevention, NHS: National Health Service, NPSA: National Patient Safety Agency, WHO: World Health Or- ganization
tion”, “medication error category”, “medication error categ- orized”, “medication error classification”, “medication error classified”, “medication error type”, “medication error glos- sary”, “medication error taxonomy”, “medication error level of harm”이었다. 국내 기관 조사를 위해서는 “medication error”, “의약품 사용 과오”를 키워드로 사용하였다. 웹에서 키워드를 그대로 검색하거나 기관명 또는 국가명을 조합하 여 검색하였다. 검색 결과 중에서 환자 안전 기관과 연관된 자료만 추려내기 위해, 특정 환자 안전 기관의 웹사이트 내 에 직접적으로 게시되어 있는 글이나, 직접적으로 게시되어 있지는 않았지만 문서 내에 기관명이 명확히 기재되어 있는 자료만 수집하였다. 추가로, 특정 기관의 웹사이트에 링크되 어 있는 다른 유관 기관의 웹사이트, 또는 특정 기관이 만든 자료에 인용 또는 소개되어 있는 자료와 웹페이지도 찾아보 았다. 검색된 자료 중 기관의 출처가 분명하지 않은 자료나 의약품 사용 오류의 정의 및 분류 유형에 대한 내용을 추출 해 낼 수 없는 자료는 모두 배제하였다. 자료 수집은 2015년 6월 1일부터 2015년 9월 22일까지 시행되었다.
결 과
국외 및 우리나라의 환자 안전 기관 중에서 의약품 사용 오류의 정의 및 분류 유형을 제시하고 있는 기관은 총 23개 였다. 국가별로는 다국적 기관이 3개, 미국 기관이 10개, 영 국을 제외한 유럽 기관이 3개, 영국 기관이 3개, 호주 기관이 1개, 뉴질랜드 기관이 2개, 우리나라 기관이 1개였다.
조사된 환자 안전 기관들이 제시하고 있는 의약품 사용 오류의 정의 및 분류 유형은 다양하였으며, 특히 분류 유형은
의약품 사용 오류를 분류하는 기준에 따라 심각도(severity) 기준, 절차(process) 기준, 행위(activity) 기준, 주체(responsi- ble person) 기준으로 나눌 수 있었다. 기관마다 네 가지 기 준 중 일부를 이용하여 의약품 사용 오류의 분류 유형을 제 시하였고, 분류 유형을 제시하지 않은 기관도 있었다. 환자 안전 기관별로 의약품 사용 오류의 정의 및 분류 유형의 제 시 여부를 정리한 결과는 표 1과 같다.
의약품 사용 오류의 정의
조사된 23개의 환자 안전 기관들은 모두 의약품 사용 오류 의 정의를 제시하고 있었다. 이 중 여러 기관에서 가장 널리 쓰이고 있는 것은 NCC MERP의 정의였다(표 1). NCC MERP와 동일한 정의를 제외하면, 환자 안전 기관들은 다양 한 키워드를 사용하여 의약품 사용 오류를 정의하고 있었고, 주로 많이 사용되는 키워드는 “event”와 “error”였다(표 2).
의약품 사용 오류의 분류 유형
환자 안전 기관에서 제시하는 의약품 사용 오류의 분류 유 형은 심각도 기준과 행위 기준으로 분류한 유형이 가장 많았 으며, 심각도 기준 유형 중에서는 NCC MERP의 유형이 가 장 널리 사용되고 있었다(표 1).
심각도 기준 유형
총 9개의 기관에서 심각도 기준 유형을 제시하고 있었으 며, 이 중 다른 기관과 동일한 유형을 제시하는 경우를 제외 하면 5개의 기관이 서로 다른 유형을 제시하고 있었다(표 3).
심각도 기준 유형들은 주로 오류(error)의 발생 여부와 위해 (harm)의 발생 여부 및 정도에 따라 의약품 사용 오류를 분
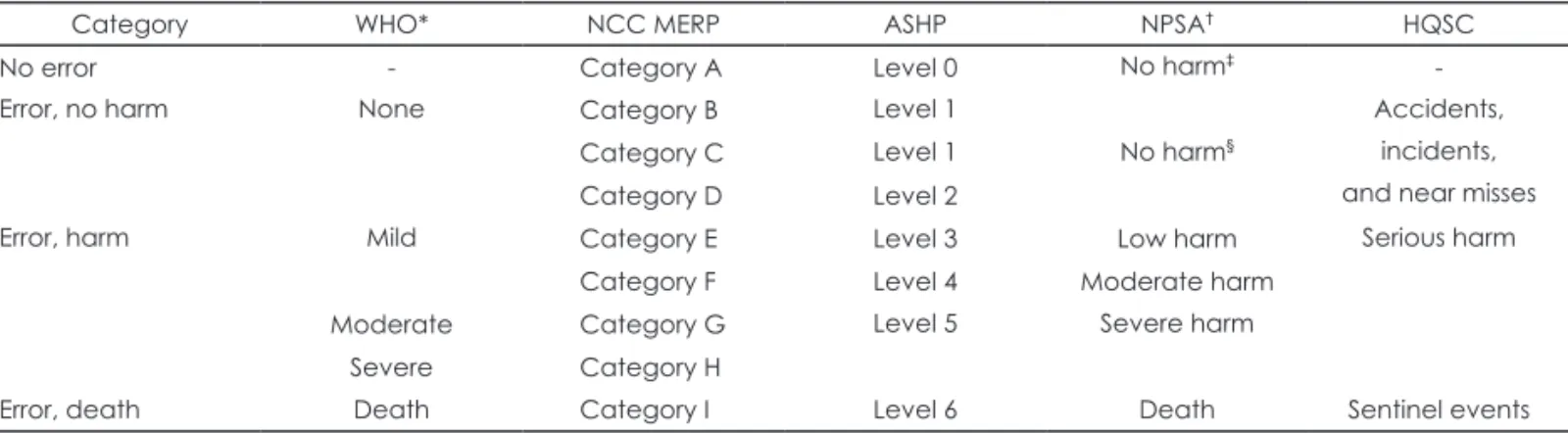
Table 4. Comparison between types of medication error based on severity
Category WHO* NCC MERP ASHP NPSA† HQSC
No error - Category A Level 0 No harm‡ -
Error, no harm None Category B Level 1 Accidents,
incidents, and near misses
Category C Level 1 No harm§
Category D Level 2
Error, harm Mild Category E Level 3 Low harm Serious harm
Category F Level 4 Moderate harm
Moderate Category G Level 5 Severe harm
Severe Category H
Error, death Death Category I Level 6 Death Sentinel events
*WHO suggests the type for patient safety incident which is a superordinate concept to a medication error. Patient safety inci- dent is defined as an event of circumstance that could have resulted, or did result, in unnecessary harm to a patient, †NPSA sug- gests the type for patient safety incident which is a superordinate concept to a medication error, ‡This means “Impact prevent- ed: any patient safety incident that had the potential to cause harm but was prevented, resulting in no harm to the person(s) receiving NHS-funded care”, §This means “Impact not prevented: any patient safety incident that ran to completion but no harm occurred to the person(s) receiving NHS-funded care”. ASHP: American Society of Health-System Pharmacists, HQSC: Health Quality & Safety Commission, NCC MERP: National Coordinating Council for Medication Error Reporting and Prevention, NHS:
National Health Service, NPSA: National Patient Safety Agency, WHO: World Health Organization
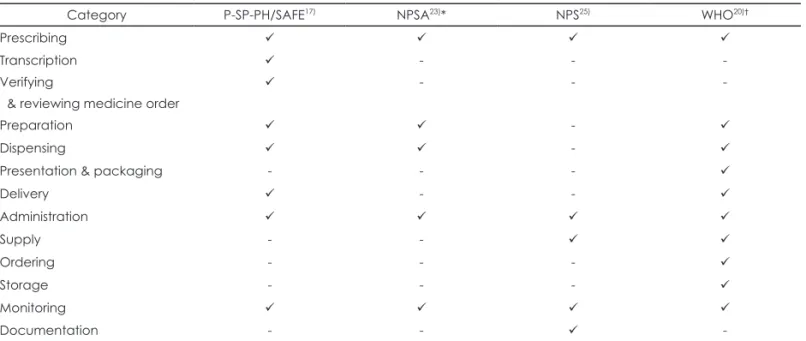
Table 5. Comparison between types of medication error based on process
Category P-SP-PH/SAFE17) NPSA23)* NPS25) WHO20)†
Prescribing
Transcription - - -
Verifying
& reviewing medicine order
- - -
Preparation -
Dispensing -
Presentation & packaging - - -
Delivery - -
Administration
Supply - -
Ordering - - -
Storage - - -
Monitoring
Documentation - - -
The mark “” means that the organization suggests a process, corresponding to the row. If the organization didn’t suggest a pro- cess, corresponding to the row, the cell was marked as “-”. *NPSA suggests the type for patient safety incident which is a superor- dinate concept to a medication error, †WHO suggests the type for patient safety incident which is a superordinate concept to a medication error. Patient safety incident is defined as an event of circumstance that could have resulted, or did result, in unnec- essary harm to a patient. NPS: National Prescribing Service Limited, NPSA: National Patient Safety Agency, P-SP-PH/SAFE: Expert Group on Safe Medication Practices, WHO: World Health Organization
Table 6. Comparison between types of medication error based on activity
Category ASCP26) ASHP22) EMA (GVP)12) NCC MERP27) USP
(MEDMARX)28)*
Prescribing error - -
Preparation error - - -
Dispensing error - - - -
Omission error - -
Dosing error†
Wrong dosage form
Wrong drug -
Unauthorized drug error - -
Wrong technique -
Wrong route of administration -
Wrong rate - - -
Wrong duration - - - -
Wrong time -
Deteriorated drug -
Wrong patient - -
Monitoring error - -
Compliance error - - -
Potential error - - - -
Mislabeling - - - -
Other -
The mark “” means that the organization suggests an activity, corresponding to the row. If the organization didn’t suggest an activity, corresponding to the row, the cell was marked as “-”. *USP launched MEDMARX in 1998, and transferred all rights, owner- ship and management of the MEDMARX to Quantros in 2008, †Dosing error includes “Improper dose”, “Improper quantity”,
“Wrong strength/concentration” and “Extra dose”. ASCP: American Society of Consultant Pharmacists, ASHP: American Society of Health-System Pharmacists, GVP: Good Pharmacovigilance Practices, NCC MERP: National Coordinating Council for Medica- tion Error Reporting and Prevention, USP: US Pharmacopeial Convention, EMA: European Medicines Agency
류하고 있었다. 즉, 모든 유형은 크게 “no error”, “error, no harm”, “error, harm”, “error, death”로 범주화되며, 위해의 정도에 따라 유형이 조금 더 세분화되는 방식이었다(표 4).
절차 기준 유형
총 4개의 기관에서 절차 기준 유형을 제시하고 있었다(표 5). 절차 기준 유형들을 비교해 본 결과, 처방, 조제, 투여, 모 니터링이라는 공통된 흐름 속에서 각각의 절차를 조금 더 세분화하여 제시하고 있었다.
행위 기준 유형
총 6개의 기관에서 행위 기준 유형을 제시하고 있었으며, 이 중 다른 기관과 동일한 유형을 제시하는 경우를 제외하 면 5개의 기관이 서로 다른 유형을 제시하고 있었다(표 6).
행위 기준 유형 중 일부는 절차 개념과 혼재되어 있어, 엄격 히 행위만을 기준으로 하였다고 보기 힘든 유형도 있었다.
또한 행위의 특성상 포괄하는 범주가 다양하여 심각도나 절 차 기준에 비해 유형 간의 비교가 용이하지 않았다.
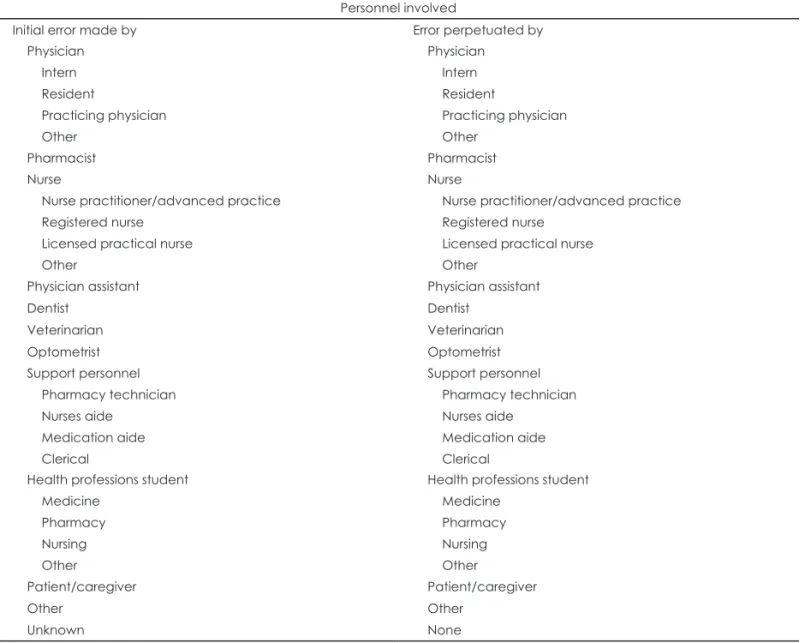
주체 기준 유형
주체 기준 유형을 제시하고 있는 기관은 NCC MERP가 유일하였다. NCC MERP는 오류를 처음 만든 주체와 영속 시킨(perpetuated) 주체를 구분하여 제시하였다(표 7).27)
고 찰
국외의 환자 안전 기관에서 사용하고 있는 의약품 사용 오 류의 정의는 대체로 NCC MERP의 정의가 널리 사용되고 있었으며, 서로 다른 정의들 간에서도 개념상의 큰 차이는 없 었다. 다만 실제 임상사례에 적용하여 의약품 사용 오류를 판 단할 때 정의만으로는 판단하기 힘든 경우가 많고, 평가자 간 의 일치도(agreement)가 낮다는 문제가 있다. NCC MERP29)
Table 7. Types of medication error based on responsible person
Personnel involved
Initial error made by Error perpetuated by
Physician Intern Resident
Practicing physician Other
Physician Intern Resident
Practicing physician Other
Pharmacist Pharmacist
Nurse
Nurse practitioner/advanced practice Registered nurse
Licensed practical nurse Other
Nurse
Nurse practitioner/advanced practice Registered nurse
Licensed practical nurse Other
Physician assistant Physician assistant
Dentist Dentist
Veterinarian Veterinarian
Optometrist Optometrist
Support personnel Pharmacy technician Nurses aide
Medication aide Clerical
Support personnel Pharmacy technician Nurses aide
Medication aide Clerical Health professions student
Medicine Pharmacy Nursing Other
Health professions student Medicine
Pharmacy Nursing Other
Patient/caregiver Patient/caregiver
Other Other
Unknown None
가 제안한 알고리즘을 사용함으로써 이와 같은 문제를 어느 정도 해소할 수 있을 것으로 보인다. 그러나 이 알고리즘은 환자에게 위해가 발생한 경우에 대해서만 의약품 사용 오류 의 여부를 판단하고 있어, 환자에게 위해가 발생하지 않은 경우는 아우르지 못한다는 한계점을 가진다.
의약품 사용 오류의 분류 유형은 환자 안전 기관마다 다양 하게 제시하고 있었다. 때문에 의약품 사용 오류의 현황을 분 석한 연구들도 저마다 다른 유형을 사용해 왔다. 사실 분류 유형이 다양한 것은 분류 기준 자체가 심각도, 절차, 행동, 주 체 등으로 다양하기 때문인데, 이 중 한가지 분류 기준만 사 용하여서는 의약품 사용 오류의 정확한 현황을 파악하기 어 렵다. NCC MERP27)에서는 “taxonomy”를 통해 의약품 사 용 오류에 대해 표준화된 용어로 가능한 한 많은 자료를 수 집할 수 있도록 유도하고 있다. 이처럼, 하나의 의약품 사용 오류 사례에 대해 다양한 분류 기준을 사용하여 여러 측면 에서 정보를 수집하는 것이 가장 이상적이나, 동일한 분류 기준 내에서는 통일된 유형을 사용할 필요가 있을 것이다.
2000년, Institute of Medicine의 보고서 “to err is human”30) 이후로 의약품 사용 오류에 대한 국제적인 관심은 날로 높아 졌으며, 환자 안전 기관에서는 의약품 사용 오류에 대한 정 의, 분류 유형, 예방 방안, 현황 등의 정보를 지속적으로 축 적 및 업데이트 해왔다. 미국과 유럽의 경우, 의약품 사용 오 류에 관한 정보를 국가적으로 수집하여 통합 및 관리함으로 써 해당 정보를 이용한 의약품 사용 오류 연구가 활발히 수 행되고 있다. 그러나 우리나라의 경우, 의료기관평가인증제 의 실시와 더불어 의료기관 내부적으로만 의약품 사용 오류 관련 정보를 수집하고, 국가적인 보고체계는 수립되어 있지 않기 때문에 의약품 사용 오류를 분석한 연구 역시 매우 저 조한 실정이다. 식품의약품안전처와 한국의약품안전관리원 이 협조 체계를 구축하여 의약품 유해 사례와 관련된 정보 를 수집 및 관리하고 있으나, 유해 사례와 의약품 사용 오류 는 동일한 개념이 아니므로 순수한 의약품 사용 오류 정보 를 추출해 내는 데에는 한계가 있다.2,6)
우리나라의 실정에 대해 국외의 환자 안전 기관이 주는 시 사점은 국내 의약품 사용 오류에 관한 정보 수집 및 연구를 담 당하는 기관을 확립할 필요성이 있다는 것이다. 담당 기관은 국가 기관 또는 민간 단체의 형태로, 우리나라의 임상 상황에 알맞은 의약품 사용 오류의 정의와 분류 유형을 제시하고 원 인 분석 및 감소 방안에 대한 연구를 지속적으로 수행해야 한 다. 이러한 연구는 반드시 임상 현장의 파악을 우선적으로 수 행하여 실용성 있는 연구 결과가 도출되도록 해야 하며, 정부 는 제도적으로 연구 결과의 확산을 도와야 할 것이다.
이 연구의 제한점은 미국, 유럽, 호주, 뉴질랜드로 조사 국
가를 한정하였기 때문에 기타 국가에서 사용하고 있는 의약 품 사용 오류의 정의 및 분류 유형을 파악하지 못하였다는 점 과 조사 국가 중에서도 자료 수집의 한계로 미처 검토하지 못 한 자료가 있을 가능성이 있다는 점이다. 대부분의 환자 안전 기관에서는 의약품 사용 오류와 관련된 정보를 지속적으로 업데이트하고 있으므로, 향후 이에 대한 지속적인 검토를 통 해 국제적인 추세를 파악해야 할 것이다.
결 론
이 연구는 미국, 유럽, 호주, 뉴질랜드에서 사용하고 있는 의약품 사용 오류의 정의 및 분류 유형을 조사하였고, 조사 된 정의와 분류 유형을 비교 분석하였다. 의약품 사용 오류의 정의는 NCC MERP의 정의가 가장 널리 사용되고 있었으 며, 대체로 유사한 개념을 나타내고 있었다. 이에 비해 의약 품 사용 오류의 분류 유형은 기관별로 다양하게 제시하고 있 었으며, 이는 의약품 사용 오류를 분류하는 데 사용된 기준이 다양한 것에 일부 기인한 것으로 보인다. 의약품 사용 오류 의 분류 유형은 심각도 기준, 절차 기준, 행위 기준, 주체 기 준으로 나눌 수 있었으며, 이 중 심각도와 행위 기준 유형이 가장 많이 사용되고 있었다. 아직까지 우리나라에서는 의약 품 사용오류에 대해서 논의가 활발히 되고 있지는 않지만, 최근 들어 이에 대한 관심이 증대되는 것을 고려한다면, 향 후 우리나라에서 사용할 의약품 사용 오류의 분류 유형에 대해서 미리 고민하여 같은 기준을 사용하도록 하는 것이 추 후 효율적인 제도 정착이나 환자 안전을 개선하기 위하여 필 요할 것으로 보인다.
Acknowledgments
본 연구는 2015년도 식품의약품안전처의 연구개발비(15172의약 안118)로 수행되었으며 이에 감사드립니다.
REFERENCES
1) Wilmer A, Louie K, Dodek P, Wong H, Ayas N. Incidence of medi- cation errors and adverse drug events in the ICU: a systematic review.
Qual Saf Health Care 2010;19:e7.
2) Koo BK. Patient safety management in the medication use process:
prevention and management of medication error. J Korean Med Assoc 2012;55:835-842.
3) Kim EK, Lee SY, Eom MR. DICS behavior pattern and medication errors by nurses. J Korean Acad Nurs Adm 2013;19:28-38.
4) Kang MK, Yoon SH, Heo YS, Kim HS, Song YC. Prevention of Med- ication Errors by Pharmacists’ Intervention of Chemotherapy. Korean Soc Health Syst Pharm 2011;28:288-295.
5) Ministry of Health and Welfare, Guidelines for preventing medica- tion error. Gwacheon: Ministry of Health and Welfare;2008.
6) Ministry of Food and Drug Safety. Development of education mate- rials to ensure medication safety and prevent medication error. Cheon- gju: Ministry of Food and Drug Safety;2015.
7) Health Quality & Safety Commission New Zealand. Alerts. Available
from: https://www.hqsc.govt.nz/our-programmes/medication-safety/
projects/alerts/. Accessed September 22, 2015.
8) National Coordinating Council for Medication Error Reporting and Prevention. Medication Error Definition. Available from: http://www.
nccmerp.org/about-medication-errors. Accessed September 22, 2015.
9) World Health Organization. Reporting and Learning Systems for Medication Errors: The Role of Pharmacovigilance Centres. Avail- able from: http://apps.who.int/medicinedocs/documents/s21625en/
s21625en.pdf. Accessed September 22, 2015.
10) Agency for Healthcare Research and Quality. Medication errors.
Available from: http://psnet.ahrq.gov/primer.aspx?primerID=23. Ac- cessed September 22, 2015.
11) Austrian Federal Office for Safety in Health Care, Austrian Medicines and Medical Devices Agency. Medication errors. Available from:
http://www.basg.gv.at/en/pharmacovigilance/medication-errors/. Ac- cessed September 22, 2015.
12) European Medicines Agency. Guideline on good pharmacovigilance practices (GVP) Module V - Risk management systems (Rev 1). Avail- able from: http://www.ema.europa.eu/docs/en_GB/document_library/
Scientific_guideline/2012/06/WC500129134.pdf. Accessed Septem- ber 22, 2015.
13) European Medicines Agency. Guideline on good pharmacovigilance practices (GVP) Module VI - Management and reporting of adverse reactions to medicinal products (Rev 1). Available from: http://www.
ema.europa.eu/docs/en_GB/document_library/Scientific_guide- line/2014/09/WC500172402.pdf. Accessed September 22, 2015.
14) Aspden P, Wolcott JA, Bootman JL, Cronenwett LR. Preventing medi- cation errors. Washington, DC: The National Academies Press;2007.
pp.50-104.
15) MEDSAFE (New Zealand Medicines and Medical Devices Safety Authority). Guideline on the Regulation of Therapeutic Products in New Zealand - part 8: Pharmacovigilance (Edition 2.0). Available from: http://www.medsafe.govt.nz/regulatory/Guideline/GRTPNZ/
part-8-pharmacovigilance.pdf. Accessed September 22, 2015.
16) European Medicines Agency. Medication errors. Available from:
http://www.ema.europa.eu/ema/index.jsp?curl=pages/special_topics/
general/general_content_000570.jsp. Accessed September 22, 2015.
17) Airaksinen M, Otero M, Schmitt E, Cousins D, Gustafsen I, Hartmann M, et al. Creation of a better medication safety culture in Europe:
Building up safe medication practices. Available from: http://www.
coe.int/t/e/social_cohesion/soc-sp/Medication%20safety%20cul- ture%20report%20E.pdf. Accessed September 22, 2015.
18) National Health Service England. Improving medication error inci- dent reporting and learning. Available from: http://www.england.nhs.
uk/wp-content/uploads/2014/03/psa-sup-info-med-error.pdf. Accessed September 22, 2015.
19) National Health Service Berkshire East. Good Practice Guidance 10:
Handling of medication errors, incidents and near misses in Care Homes. Available from: http://www.windsorascotmaidenheadccg.
nhs.uk/download/care_home_guidance/10.%20Good%20Prac-
tice%20Guidance%2010.%20medication%20error%20report- ing%20in%20care%20homes.pdf. Accessed September 22, 2015.
20) World Health Organization. Conceptual Framework for the Interna- tional Classification for Patient Safety. Available from: http://www.
who.int/patientsafety/taxonomy/icps_full_report.pdf?ua=1. Accessed September 22, 2015.
21) National Coordinating Council for Medication Error Reporting and Prevention. NCC MERP Index for Categorizing Medication Errors.
Available from: http://www.nccmerp.org/sites/default/files/indexCol- or2001-06-12.pdf. Revised February 20, 2001. Accessed September 22, 2015.
22) American Society of Health-System Pharmacists. ASHP guidelines on preventing medication errors in hospitals. Am J Hosp Pharm 1993;
50:305-314.
23) National Patient Safety Agency. Safety in doses: medication safety incidents in the NHS. Available from: http://www.nrls.npsa.nhs.uk/
EasySiteWeb/getresource.axd?AssetID=61392.Accessed September 22, 2015.
24) Quality Improvement Committee. Serious and Sentinel Events in New Zealand Hospitals. Available from: http://www.hqsc.govt.nz/as- sets/Reportable-Events/Publications/Serious-and-Sentinel-Events- Report-2008-09.pdf. Accessed September 22, 2015.
25) National Prescribing Service Limited. Medication Safety in the Com- munity: A Review of the Literature. Available from: http://www.nps.
org.au/__data/assets/pdf_file/0008/71675/09060902_Meds_safety_
June_2009.pdf. Accessed September 22, 2015.
26) American Society of Consultant Pharmacists. Guidelines on Prevent- ing Medication Errors in Pharmacies and Long-term Care Facilities through Reporting and Evaluation. Available from: https://www.ascp.
com/resources/policy/upload/Gui97-Med%20Errors.pdf. Accessed September 22, 2015.
27) National Coordinating Council for Medication Error Reporting and Prevention. NCC MERP Taxonomy of Medication Errors. Available from: http://www.nccmerp.org/sites/default/files/taxonomy2001-07-31.
pdf. Accessed September 22, 2015.
28) Hicks RW, Becker SC, Cousins DD. MEDMARX data report. A re- port on the relationship of drug names and medication errors in re- sponse to the Institute of Medicine’s call for action. Available from:
http://www.labatecpharma.com/wp-content/uploads/2012/02/
2008MEDMARX-DataReport.pdf. 2008. Accessed September 22, 2015.
29) National Coordinating Council for Medication Error Reporting and Prevention. Contemporary View of Medication-Related Harm. A New Paradigm. Available from: http://www.nccmerp.org/sites/default/
files/nccmerp_fact_sheet_2015-02-v91.pdf. Accessed September 22, 2015.
30) Kohn LT, Corrigan JM, Donaldson MS. To err is human: building a Safer Health System. Washington, DC: National Academy Press;
2000.