Case Report
원고 접수일 2013년 1월 24일, 원고 수정일 2013년 2월 22일, 게재 확정일 2013년 3월 26일
책임저자 고승오
(561-756) 전주시 덕진구 백제대로 567, 전북대학교 치의학전문대학원 구강악안면 외과학교실
Tel: 063-250-2113, Fax: 063-250-2089, E-mail: [email protected]
RECEIVED January 24, 2013, REVISED February 22, 2013, ACCEPTED March 26, 2013
Correspondence to Seung-O Ko
Department of Oral and Maxillofacial Surgery, School of Dentistry, Jeonbuk National University
567 Baekje-daero, Deokjin-gu, Jeonju 561-756, Korea
Tel: 82-63-250-2113, Fax: 82-63-250-2089, E-mail: [email protected]
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
치성 낭종으로부터 유래된 원발성 골내 편평상피세포 암종:
증례보고
김태광1,2ㆍ이선재1ㆍ임대호1ㆍ백진아1ㆍ신효근1ㆍ고승오1,2
1전북대학교 치의학전문대학원 구강악안면외과학교실, 구강생체과학연구소, BK21사업,
2전북대학교 임상의학연구소, 전북대학교병원 의생명연구원
Abstract
Primary Intraosseous Squamous Cell Carcinoma Arising from Odontogenic Cyst: A Case Report
Tae-Kwang Kim
1,2, Sun-Jae Lee
1, Dae-Ho Leem
1, Jin-A Baek
1, Hyo-Keun Shin
1, Seung-O Ko
1,21
Department of Oral and Maxillofacial Surgery, School of Dentistry, Jeonbuk National University, Institute of Oral Bio-Science, Brain Korea 21 Project,
2Research Institute of Clinical Medicine, Chonbuk National University,
Biomedical Research Institute, Chonbuk National University Hospital
Primary intraosseous squamous cell carcinoma (PIOSCC) is a rare form arising within the jaws. PIOSCC is not related to the oral mucosa, presumably developing from remnants of the odontogenic epithelium. Because odontogenic cyst epithelium often transforms malignantly into PIOSCC, it could be misdiagnosed as odontogenic cyst based on a relatively ill-defined radiolucent lesion. Therefore, definite diagnosis is established from histological examination of biopsy samples taken during cyst enucleation in many cases. The present study is reported with a case of patient complaining of discomfort on his mandible.
He was diagnosed as a putative dentigerous cyst and underwent a cyst enucleation treatment. After definite diagnosis as PIOSCC was established based on histologic findings, partial mandible resection and mandible reconstruction were performed.
Up to the present, 10 months follow up of the patient showed satisfactory healing without recurrence and abnormal findings;
thereby, we are reporting this case with literature review.
Key words: Squamous cell carcinoma, Odontogenic cysts, Mandible
서 론
원발성 골내암종(primary intraosseous carcinoma, PIOC)
은 악골에 생기는 질환으로 구강 내 점막과는 관련 없이 치성
상피 잔사로부터 유래된다고 알려져 있다[1,2]. 이 질환은 Loos가
1913년 “Central maxillary epidermoid carcinoma”라는 이름
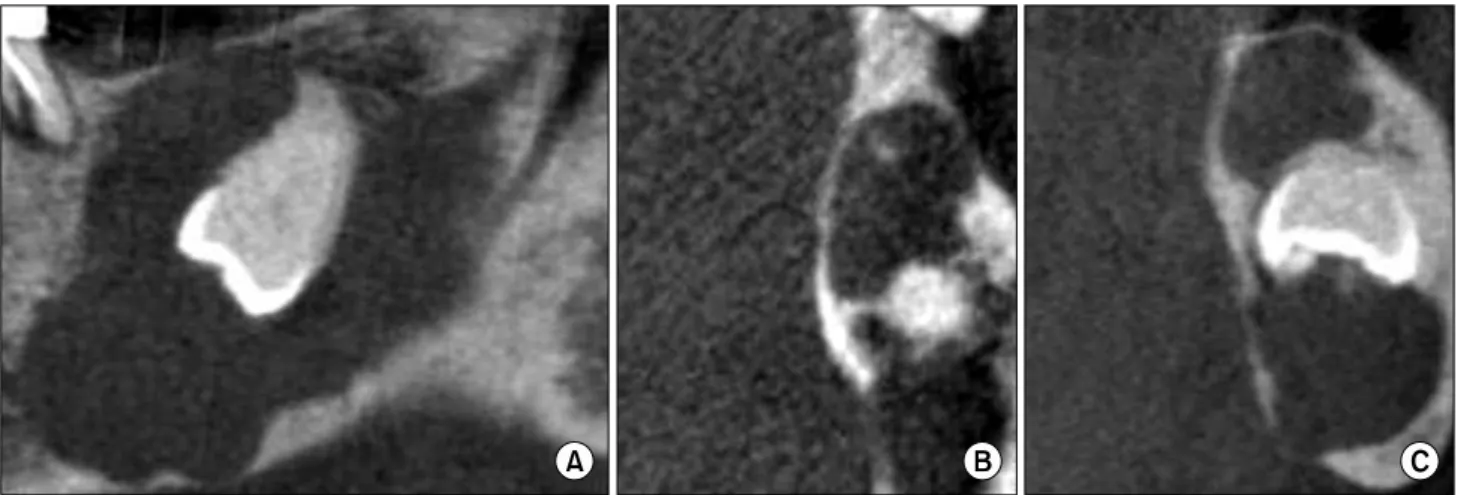
Fig. 2. Preoperative cone beam computed tomography (CBCT) views. (A) CT shows bone destruction on lower border of the mandible,
and the left inferior alveolar nerve is involved within the lesion. (B, C) CT shows perforation of lingual cortical bone.Fig. 1. Preoperative panoramic view. Ill-defined radiolucent lesion
(about 25×25 mm), including #38 impacted tooth on the left lower posterior mandible.으로 처음 보고하였으며, 이후 여러 학자들에 의해서 소개되어 오면서 용어에 있어 변화가 있었고, PIOC라는 용어는 Pindborg 등[3]이 1972년 세계보건기구(World Health Organization, WHO)에서 처음 발표하였다. Eversole 등[4]은 원발성 골내 편평 상피세포 암종(primary intraosseous squamous cell carcino- ma, PIOSCC)이라는 용어를 2005년 처음 사용하였으며 세 가지 형태인 (1) type 1: 고형 종양(solid tumor), (2) type 2: 치성 낭종으로부터 유래된 암종, (3) type 3: 치성 종양과 연관된 암종 으로 분류하였다.
본 증례는 좌측 하악 구치부의 지속된 불편감을 주소로 내원한 환자에서 임상 및 방사선학적 검사상 함치성 낭종으로 추정 진단 하고 낭종 적출술을 시행하였으나, 조직검사 결과 PIOSCC로 최 종 진단하고 하악골 부분 절제술 및 하악골 재건술을 시행한 후 경과관찰 중인 성인 환자 1예에 관하여 문헌고찰과 함께 보고 하고자 한다.
증례보고
74세 남자 환자로 2012년 4월에 좌측 하악 구치부의 불편감과 local clinic에서 촬영한 파노라마 방사선 사진에서 좌측 하악골에 방사선 투과성 병소가 관찰되어 이에 대한 제거를 위해 전북대학 교 치과병원 구강악안면외과에 내원하였다. 전신병력으로 고혈압 진단하에 약물 복용 중이었으며, 기왕력으로 약 4년 전부터 지속 된 #36 치아의 통증이 지속되어 local clinic에서 신경치료를 진행하였으나, 불편감이 해소되지 않았다. 임상적으로는 구강 내 특이소견은 발견되지 않았으나, 방사선학적으로 좌측 하악 구치 부에 #38 치아 매복을 동반한 약 25×25 mm 크기의 비교적 경계가 고르지 못한 방사선 투과성 병소가 관찰되어 함치성 낭종 으로 추정 진단하였다. 진단 시 악성종양은 전혀 고려하지 않았고 재발성이 있는 범랑아세포종이나 각화낭성치성종양 등의 양성종 양 가능성 또한 적어 보였다. 협측 치밀골 천공 소견도 관찰되지 않아서 침습적인 절개 생검을 생략하고 낭종 적출술을 한 후에 최종적으로 조직검사를 하기로 계획하였다(Fig. 1, 2). 전신마취 하에 #36, 38 치아 발거 및 낭종 적출술을 시행하였으며, 적출해 낸 병소는 피막화(encapsulation)가 잘 되어 있었고 주위 골과 비교적 명확한 경계를 지니고 있었으며 다른 특이 소견은 관찰되 지 않았다(Fig. 3). 적출한 낭종을 조직검사를 의뢰하였으며 조직 검사 결과, 25배율 조직 사진상 우측으로는 cyst 양상의 epithelial lining이 관찰되지만, 좌측의 경우 우측 하방 부위에서 epithelial lining이 전형적이지 못하고 변이가 되고 있는 것이 관찰되었으며, 좌측 전반에 걸쳐 cancer cell들이 관찰되는 것을 볼 수 있었다.
또한, 50배율 사진상에서도 cancer cell들이 전반적으로 분포하
고, cell들 사이 염증세포들도 관찰되었으며, 중앙부위의 cancer
cell에서 keratinization되어 있는 것이 관찰되고 있어 Eversole
의 분류에 따라 PIOSCC type 2, well differentiated type으로
최종 진단하였다(Fig. 4).
Fig. 5. Second preoperative photograph. Wax-up for making resin
block using rapid prototyping model.Fig. 4. Histopathologic examination (H&E; (A) ×25, (B) ×50). (A) At this figure, the area defined with black arrows shows typical epithelial
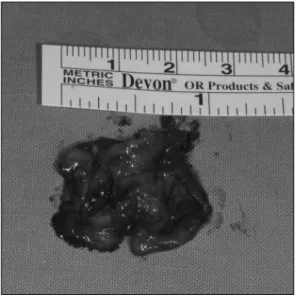
lining like cystic lesion, but the another area with white arrows represent atypical epithelial lining and cancer cells. (B) The figure shows generally cancer cells with keratinizations.Fig. 3. Intraoperative photograph. Mass removed from mandible.
악성종양에 따르는 2차 수술이 필요하게 되었고 먼저 인접 연조직 및 림프절로의 이환 여부를 판단하기 위해 술 전에 mag- netic resonance imaging (MRI)과 positron emission tomog- raphy-computed tomography (FET-CT)를 촬영하였으며 검사 결과 인접 연조직 및 림프절 전이는 없었다. 치료계획으로 부분 하악골 절제술 및 하악골 재건을 시행하기로 결정하였고 추가적인 경부청소술이나 술 후 방사선치료 등은 시행하지 않기로 하였다.
하악골 재건은 방사선 소견 및 rapid prototyping (RP) model상 재건에 필요한 골의 길이가 약 6 cm 정도로 판단되어 비혈행화 장골을 이용하기로 결정하였으며, RP model에서 절제할 하악골 부위 및 재건에 필요한 장골의 크기 및 형태를 미리 설정하여 레진 블록을 제작하였다(Fig. 5). 1차 수술 후 약 2주 후에 2차
수술을 시행하였다. 술 전 촬영한 cone beam computed to-
mography 영상에서 일부 설측 피질골 천공 소견이 관찰되어
(Fig. 2) 술중 인접 연조직과 악하 림프절을 일부 절제하여 동결
절편 조직검사(frozen section biopsy)를 시행하였으며, 모두
특이소견이 발견되지 않았고 계획대로 경부청소술은 시행하지
않았다. 병소에 이환된 좌측 하악골을 병소 경계로부터 약 1 cm
정도의 safety margin을 설정하여 절제하였으며, 술 후 하악 과두
의 위치가 변하는 것을 막고 수술 시간을 단축하기 위해서 술
전 RP model상에서 하악골 형태에 맞게 미리 구부려 놓은 man-
dible reconstruction plate를 위치시켜 고정한 후 하악골 절제술
시행하였다. 술 전 제작한 레진 블록을 이용하여 전방 장골능에서
채취하였고 결손부에 맞게 일부 조정한 다음 plate를 이용하여
고정하였다(Fig. 6). 술 후 10개월인 현재까지 재발 및 전이 소견
은 보이지 않고 있고, 이식한 골흡수 소견도 거의 보이지 않는
상태로 골생착이 잘 이루어진 양상이 관찰되고 있다(Fig. 7).
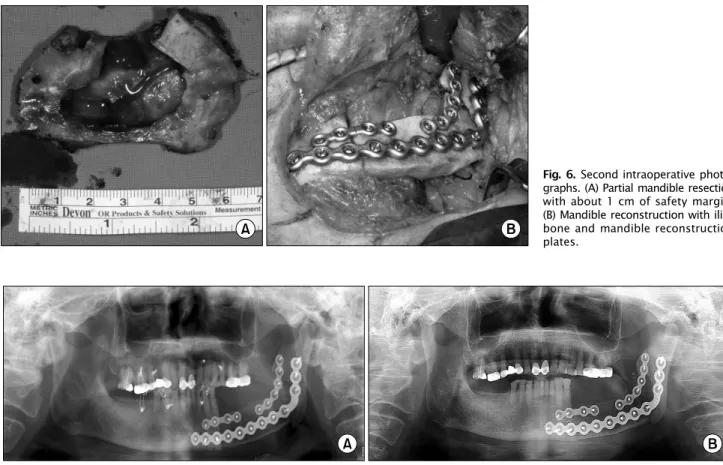
Fig. 7. Postoperative panoramic views. (A) Postoperative 1 month, (B) postoperative 10 months.
Fig. 6. Second intraoperative photo-
graphs. (A) Partial mandible resection with about 1 cm of safety margin.(B) Mandible reconstruction with iliac bone and mandible reconstruction plates.
고 찰
PIOSCC는 드문 질환으로 악골에서만 발생한다고 알려져 있으 며, 이는 PIOSCC가 상피세포 기원이나 다른 골격계 내에서는 상피세포가 발견되지 않고 있기 때문이다[5,6]. 이러한 상피세포 로는 잔존 법랑 상피, 매복 치아 주위의 잔존 법랑 상피, 치주인대 내의 malassez 상피 잔사, 잔존 치판 등으로부터 유래되는 것으로 추정된다[7,8]. 또한, PIOSCC는 이전에 존재하던 치성 낭종이나 법랑모세포종이 악성으로 변이되면서도 발생할 수도 있다고 알려 져 있다[9].
PIOSCC의 유병률을 살펴보면, 4∼81세의 다양한 연령대에서 발생하지만 연령이 증가할수록 발생 빈도 또한 증가하며, 여성보 다는 남성에서 높은 발생 빈도를 보이고, 대부분의 경우 하악 구치부에서 발생한다고 알려져 있다[7]. PIOSCC가 이러한 유병 률을 보이는 데에는 명확하지는 않지만 낭종의 경우 남성에게서 호발하며, 하악 구치부에서 호발하는 것과도 어느 정도 연관이 있을 수 있다고 추정해 볼 수 있다[2,10]. Van der Waal 등[11]은 292명의 구강암 환자들 중에서 치성 낭종에서 기인한 편평상피세 포 암종 환자 5명(1.8%)을 보고하였으며, Otten 등[12]은 371명 의 구강암종 환자 중에서 PIOSCC 환자 5명(1.6%)을 보고하였으 나 이 중 2명만이 치성 낭종과 관련 있었다고 하였다.
임상적 특징으로는 통증, 부종, 협 또는 설(구개)측 피질골의 천공, 만성 상악동 관(chronic sinus tract) 등이 나타날 수 있으 며, 통증은 하치조 신경이 병소에 이환되어 있는 경우 주로 나타난 다[13,14]. 하지만 이러한 특징들은 2차 감염을 동반한 낭성 병소 에서도 관찰될 수 있으며, 뚜렷한 증상이 없는 경우도 보고되고 있다[10].
방사선학적으로는 비교적 경계가 불명확한 방사선 투과성 병소 가 관찰되며, 약 60%는 잔류낭 또는 치근단낭, 약 40%는 함치성 낭 또는 각화낭성 치성 종양과 관련되어 있다[2]. 따라서 종종 일반적인 치성 병소로 잘못 진단하고 발치, 근관 치료, 낭종 적출 술 등을 시행하게 되며, 이후 조직 검사를 통해 정확한 진단이 이루어지고 나서야 올바른 치료를 시행하게 된다[13].
WHO에 의한 하악골에 발생한 PIOSCC와 감별해야 할 질환으
로는 악골에 침윤된 점막형 편평상피세포 암종, 신체 내 타 부위로
부터 전이된 악골 종양(jaw bone tumor), 법랑모세포암종
(ameloblastic carcinoma), 악성 법랑모세포종(malignant ame-
loblastoma), 만성 골수염 등이 있다[6,15]. 일반적으로는 구강
내 특이소견을 나타내지 않는 경우가 대부분이나 구강 내 점막에
궤양이 존재할 시 구강 점막에서 발생한 것인지 또는 악골 내에서부
터 발생한 것인지 감별하기 위해서는 골파괴의 정도를 확인해야
하는데, 골파괴 범위가 구강 점막 궤양보다 더 넓을 경우에는
병소가 악골 내에서 발생한 것으로 추정할 수 있다[6].
PIOSCC 치료에 대한 접근은 암종의 크기를 통해 결정할 수 있지만[16], 외과적 절제술을 1차적인 치료법으로 추천하고 있으 며, 임상 및 방사선학적으로 경부 림프절 전이가 의심될 때에는 경부청소술을 시행해야 한다[1]. 만약 병소의 범위가 너무 크거나 병소를 완전히 제거하지 못하는 경우에는 추가적으로 방사선 요법 또는 항암 화학요법을 고려할 수 있다[6,17]. Bodner 등[2]은 1938년부터 2010년까지 발표된 논문에서 PIOSCC 환자 116예를 정리하였는데, 53명(46%)은 외과적 절제술만 시행하였고, 44명 (38%)은 외과적 절제술과 방사선 요법, 7명(6%)은 외과적 절제 술과 항암 화학 요법, 7명(6%)은 외과적 절제술, 방사선 요법, 항암 화학 요법을 병행하였으며, 4명(4%)은 방사선 요법만 시행 하였다고 보고하였다. 경부 림프절 전이에 대해서는 Suei 등[18]
은 33명 중 13명(39.4%)에서 림프절 전이가 있었다고 보고하였 고, Zwetyenga 등[17]은 36명 중 10명(28%)이었다고 보고하였 다. 본 증례의 경우 술 전 촬영한 MRI 및 PET-CT상에서 그리고 술중 시행한 동결 절편 조직 검사에서도 인접 연조직 및 림프절로 의 전이 소견은 관찰되지 않아 경부청소술은 시행하지 않고 하악 골 절제술 및 재건술을 시행하였으며, 술 후 추가적인 방사선 요법 또는 항암 화학 요법은 시행하지 않았다.
종양, 감염 및 심한 외상으로 인한 하악골 결손부의 재건 시 장골은 광범위한 골결손부에서도 사용될 수 있을 만큼 많은 양의 골채취가 가능하고 골질이 악골과 유사하기 때문에 하악골 재건술 에 많이 이용되어 왔으며, 여러 연구에서 혈행화 장골 이식술의 높은 생착 성공률을 보고하고 있다[19,20]. 하지만 비혈행화 장골 이식술의 경우에도 비교적 높은 생착 성공률을 보이면서 수술 시간 및 치유 기간의 감소, 상대적으로 적은 술 후 합병증 등의 장점을 지니고 있어 하악골 이식술 시 1차 선택 방법으로 사용할 수 있다. 하지만 Chen 등[21]은 골이식편의 길이가 이식 후 성공 률에 영향을 줄 수 있다고 하였으며, 이식편의 길이가 6 cm 이상 이 되면 실패율이 증가하며 혈행화 골이식의 적응증이 될 수 있다고 보고하였다. 그러나 Choi 등[22]은 하악골의 결손부위가 6 cm 이상인 경우에도 수술의 간편성과 수술시간의 단축, 환자의 술 후 회복기간, 술 후 합병증 가능성 등을 고려해볼 때 비혈행화 장골 이식술은 여전히 예지성 있는 치료방법이라고 하였다. 본 증례의 경우 술 전 방사선 검사 소견과 RP model을 이용한 분석 결과 하악골 절제 후, 약 6 cm 크기의 골이식술이 요구된다 고 판단하였으며, 수술 시간의 단축과 환자의 회복 기간의 감소 및 술 후 발생할 수 있는 합병증을 고려하여 비혈행화 장골 이식술 을 계획하였으며, 술 후 10개월인 현재까지 방사선 소견상 골흡수 가 거의 없이 매우 성공적인 골 생착을 보이고 있다.
Bodner 등[2]은 또한 조직 병리학적으로도 분석하였는데 car- cinoma in situ 4명(3%), well differentiated squamous cell carcinoma (SCC) 53명(45%), moderately differentiated SCC
47명(40%), Poorly differentiated SCC 8명(7%), 기타 4명(3%) 으로 well 또는 moderately differentiated SCC가 85%를 차지 한다고 보고하였다. 예후는 비교적 좋지 못한 편인데 2년 생존율 은 53∼63%로 보고되고 있으며, 5년 생존율은 30∼40%로 보고 되고 있다[1,2,12,18,23,24].
방사선 소견상 악골 내에 국한된 낭종으로 예비 진단된 경우 그 침습성 때문에 술 전 절개 생검을 하지 않은 상태에서 낭종 적출술을 하는 경우가 많이 있고, 경우에 따라서는 술 후 생검이 생략되거나 소홀하게 관리되는 경우도 간혹 발생할 수 있다.
Tomomatsu 등[25]과 Myoung 등[26]은 각화낭성치성종양과 같 은 재발률이 높은 병소의 경우 수술 전 생검을 통해 확정 진단을 거쳐 적절한 수술법을 결정할 것을 추천하였다. Choi 등[27]은 방사선상으로 각화낭성치성종양이 의심되는 경우에도 단방성이 병소인 경우에는 침습적인 술 전 절개 생검을 생략하는 것도 고려할 수 있다고 하였다. 본 증례의 경우 임상 및 방사선 소견상 악성 종양은 전혀 고려하지 않았고 범랑아세포종이나 각화낭성치 성종양 등 재발성이 있는 양성종양의 가능성 또한 적어 보였으며 협측 치밀골 천공 소견도 관찰되지 않아서 침습적인 술 전 절개 생검을 생략하고 낭종 적출술을 한 후에 최종적으로 조직검사를 하기로 계획하였다. 하지만 이러한 낭종으로부터 유래되어 악성 종양이 발생될 가능성이 없지 않다는 것을 술자들은 기억해야 할 것이며 이러한 사실을 염두에 두고 술 전 절개 생검도 고려해야 하고 술 전 절개 생검을 하지는 않더라도 적출술 후 최종 생검을 반드시 해야 하며, 그 결과도 주의 깊게 살펴볼 필요가 있다.
본 증례는 좌측 하악 구치부의 불편감을 주소로 내원한 환자를 대상으로 임상 및 방사선학적 검사를 통해 함치성 낭종으로 추정 진단하고 낭종 적출술을 시행하였으나, 조직검사 결과 PIOSCC로 최종 진단하고 부분 하악골 절제술 및 재건술을 시행한 증례로 술 후 10개월이 지난 현재까지 재발 및 특이소견은 보이지 않고 있으며 이에 대해 문헌 고찰과 함께 보고하는 바이다.
Acknowledgements
This paper was supported by Fund of Chonbuk National University Hospital Research Institute of Clinical Medicine.
References