Public perception of risk-reducing salpingectomy for preventing ovarian cancer
5
0
0
전체 글
(2)
(3)
(4)
(5)
수치
관련 문서
Given the unclear causal relevance of previously reported observational associations of risk factors in the aetiology of epithelial ovarian cancer, and limited exploration of
Also, a collaborative reanalysis of 45 epidemiologic studies on the role of oral contraceptives and the risk of ovarian cancer reported a significant reduction in serous
LN, lymph node; OV, ovary; SGOG, Shanghai Gynecologic Oncology Group; SOTO, searching an optimal chemo/anti-angiogenic therapy in platinum resistant ovarian cancer; SUNNY, study
Gynecologic Oncology, MD Anderson Cancer Center Orlando, 105 West Miller Street, Orlando, FL 32806, USA.. surgery, and vascular wall distortion from tumor compression. Perhaps
In the Table listing sister organizations in gynecologic oncology and their leaders, the International Gynecologic Cancer Society (President,
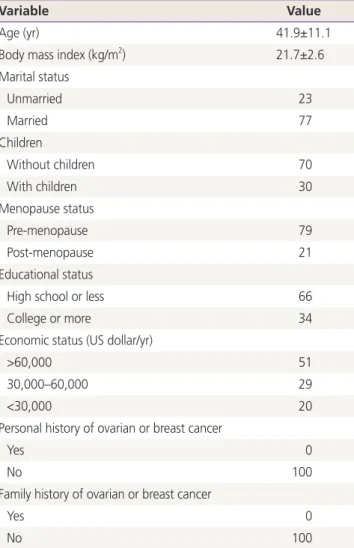
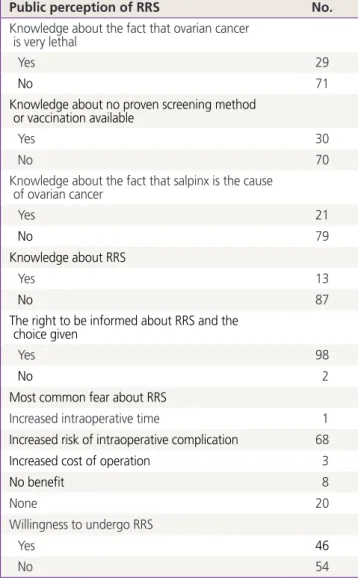
This paper aimed to investigate the level of knowledge of hereditary ovarian cancer and anxiety in women diagnosed with serous ovarian cancer in Korea and determine differences
In the Gynecologic Oncology Group (GOG) 172 trial [5], a milestone study investigating the survival between the two groups, patients with stage III ovarian or primary
This paper aimed to investigate the level of knowledge of hereditary ovarian cancer and anxiety in women diagnosed with serous ovarian cancer in Korea and determine differences in
