1
관상동맥 스텐트 삽입술 후 Clopidogrel과 Cilostazol의 비교
송인숙a,b·최승기b,c·오정미d
a숙명여자대학교 임상약학대학원, b포천중문의과대학교 분당차병원 약제부,
c포천중문의과대학 약리학교실, d서울대학교 약학대학 임상약학실
Comparison of Clopidogrel versus Cilostazol in Coronary Artery Stenting
In Sook Song
a,b, Seung Ki Choi
b,cand Jung Mi Oh
da
Graduate School of Clinical Pharmacy, Sookmyung Women’s University, Seoul, 140-742, Korea
b
Dept of Pharmacy, Bundang CHA General Hospital
c
Department of Pharmacology, College of Medicine, Pochon CHA University, Sungnam, Kyonggi-do, 463-712, Korea
d
College of Pharmacy, Seoul national University, Seoul, 151-742, Korea
Following intracoronary stenting, antiplatelet therapy lead to greater protection from thrombotic complication. A few data are available about the effect of clopidogrel versus cilostazol, an antiplatelet commonly used after intracoronary stenting. To evaluate the efficacy and safety of clopidogrel plus aspirin compared with those of cilostazol plus aspirin in coronary stenting and to evaluate the efficacy of clopidogrel loading dose prior to coronary stenting in clopidogrel group. Data were retrospectively collected from medical charts of patients who had undergone coronary stenting and received either clopidogrel with or without loading 300 mg followed by 75 mg/d (n=58), or 200 mg/d cilostazol (n=72) for 1 year, between January 2000 and May 2002. All patients in both groups received aspirin 200 mg/d throughout the study. The primary endpoints at 7, 30, 180 and 365 days after stenting were the composite of death, Myocardial Infarc- tion, stroke, angina, and revascularization in the intent to treat population and restenosis at follow up angiography. The secondary endpoints were the incidence of bleeding complications at 7, 30, and 365 days, and durg adverse effects at 365 days after stenting. At 180 and 365 days after stenting, the combined primary endpoints were significantly reduced in clopidogrel plus aspirin group (relative risk 0.39; 95% CI 0.17 to 0.92; p=0.021, RR 0.43; 95% CI 0.22 to 0.84;
p=0.0085, respectively). However, the combined primary endpoints were not significantly different between the two groups at 7 and 30 days (p=1.00, p=0.79, respectively). Angiographic restenosis rate was 14.3% in clopidogrel plus aspirin group and 32.1% in cilostazol plus aspirin group (p=0.19). 300 mg of clopidogrel loading dose did not signifi- cantly reduce the combined primary endpoints at 30 days after stenting (RR 0.14; 95% CI 0.01 to 2.65; p=0.23). The rate of bleeding complications and drug adverse effects were not different between the two groups. In patients undergo- ing intracoronary stenting, clopidogrel plus aspirin therapy is more beneficial than cilostazol plus aspirin in reducing major adverse cardiac events with similar rate of bleeding complication. A loading dose of clopidogrel did not lead to a statistically significant reduction in major adverse cardiac events.
□ Key words
– clopidogrel, cilostazol, intracoronary stenting, major adverse cardiac events, bleeding complication
관상동맥질환이란 일반적으로 죽상동맥경화증으로 인해 관 상동맥의 협착이 일어나 심근의 혈류공급이 감소되어 협심증 이나 심근경색증, 심한 경우는 사망으로 이어지는 임상적인 증상을 말한다. 이 관상동맥질환은 서구에서는 이미 오래 전 부터 가장 흔한 사망원인으로 알려져 있고 최근 우리나라에
서도 동물성 지방섭취의 증가 등 식이습관의 변화와 함께 관상동맥질환이 급격히 증가하는 추세에 있다1). 이러한 관상 동맥 협착 병변의 치료로 관상동맥 풍선확장술에 비해 스텐 트 삽입술이 시술의 성공률을 높이고 재협착을 감소시키다는 보고 이후 스텐트라는 그물망을 삽입하여 혈관을 확장시키고 협착상태를 해소해주는 관상동맥 스텐트 삽입술이 급격히 증 가되고 있다2,3).하지만스텐트 자체가 이물질이므로 스텐트 삽입 후 한달 안에 발생하는 급성 및 아급성 스텐트 혈전증 이4) 중재술 이후 재협착이나 심근경색, 사망, 응급 관상동맥 우회술 등과 같은 허혈성 합병증으로 이어지고 있다5).
Correspondence to :
송인숙E-mail:
스텐트삽입술후혈전증
(
또는허혈성합병증)
을예방하기 위해 종래에는heparin,
경구용항응고제, aspirin
등을 병합 투여한 항응고 요법이 시행되어졌으나 출혈 등의 합병증이 높아6),
최근에는항혈소판제제의병합요법이도입되어출혈 과같은합병증을감소시키고입원기간도단축시켰다7).
스텐트삽입술후사용하는항혈소판제제의대표적인요법으로
aspirin
과thienopyridine
계열의 약물인ticlopidine
의 병합요법이있으며
ticlopidine
은작용발현시간이늦어최고의항혈소판 효과를 나타내려면
2-5
일이 소요되지만8),
이 요법은aspirin
과경구용항응고제의병합요법보다혈전증과출혈및혈관합병증을감소시킨다고보고하였다9)
.
그러나ticlopidine
은 발생빈도는낮지만 치명적으로 나타날 수 있는 중성구 감소증
,
혈소판감소증,
간기능 장애 등의 부작용이문제가되었고10)
,
이에좀더안전한약물이필요하게되었다. Cilostazol
은 혈소판의c-AMP phosphodiesterase type III
를 선택적으로억제하여혈소판응집억제및혈관확장등다양 한 작용기전을 가진 약물로 스텐트 삽입 후 기존의ticlopidine
에비교하여효과적인치료농도도달시간이빠르다고알려져있다11)
. Park
등12)이나Yoon
등13)에의하면cilostazol
은
ticlopidine
에 버금가는항혈소판작용을가지며, Kozuma
등14)이나
Kamishirado
등15)에 의하면ticlopidine
과 비교하여 재협착률을감소시키고,
심각한부작용을유발하지않는다고 보고하였다12-15).
Clopidogrel
은최근에개발된thienopyridine
계열의약물로선택적이고 비가역적인
platelet adenosine diphosphate(ADP) receptor inhibitor
로 혈소판에친화력이높은platelet fibrinogen receptor(GpIIb/IIIa)
의전환을억제하며aspirin
과병용투여했 을 때 항혈소판 작용의 상승효과가 있다고 알려져있다16).
또한
ticlopidine
보다강력한항혈소판효과를나타내고17),
작 용발현시간이좀더빠르며치명적인부작용을유발하지않는 것으로 알려져 있다18). CLASSICS
5) 연구에서는clopidogrel
은
ticlopidine
에 비해 안전하고순응도가 우수할뿐만 아니라항혈소판효과도유사하다고보고했다
. Clopidogrel 300 mg
부하량
(loading dose)
의투여는부하량을투여하지않고유지용량인
75 mg
을 투여할 때보다 작용발현시간이 더 빠르고5
µmol/L ADP-induced platelet aggregation
을 감소시켜혈전 을방지하는데초기효과가있다19).
PCI-CURE
20)연구, CREDO
21)연구등은스텐트시술전에clopidogrel 300 mg
을 부하량으로전처치한후 장기간 투여한 경우 주요심장사건
(major adverse cardiac events, MACE)
즉사망
,
심근경색,
뇌졸증,
혈관재관류등의총사건을유의 성 있게 감소시키고 출혈 등의 부작용에유의한 차이가없 다고 보고하였다.
상기연구들에의해clopidogrel
과cilostazol
은 스텐트 삽입 후 항혈소판 제제로서
ticlopidine
과 비교하여 동등이상의효과와안전성이보고되었고
, Lee
등32)에의 하면 스텐트삽입후30
일동안의 임상추적 결과cilostazol
이
clopidogrel
만큼안전하고효과적인항혈소판제제라고보고하였다
.
본연구에서는관상동맥스텐트삽입술을받은환 자 중에서스텐트 삽입술전에clopidogrel-aspirin
병합요법 이나cilostazol-aspirin
병합요법을장기간투여한환자를대 상으로항혈전효과로인한주요심장사건의감소와약물의 부작용을 비교하여 효과와 안전성을 평가하고 더불어clopidogrel-aspirin
군 내에서 스텐트 삽입술 전에 전처치로300 mg
부하량을투여할경우주요심장사건에미치는영향을평가하고자하였다
연구 방법
연구대상포천중문의과대학분당차병원에서
2000
년1
월부터2002
년5
월까지관상동맥스텐트삽입술을실시한환자들을대상으로 환자의입원
,
외래 기록을열람하여후향적방법으로자료를수집하여연구하였다
.
포함기준
스텐트를삽입한환자를 대상으로
clopidogrel-aspirin
를투 여 받은 환자이거나cilostazol-aspirin
을 투여 받은 환자로1
년동안추적관찰이가능한환자로하였다
.
제외기준
좌주관상동맥
(left main coronary artery)
에협착이있는환자, 3
주전에 관상동맥중재술에 실패한 환자, aspirin, clopidogrel,
cilostazol
외에 다른항혈소판제제를추가적으로복용한환자는 제외하였다
.
혈액검사에서 혈소판 감소증(<150,000/
mm
3)
환자나 심한 간 또는 신장질환자(serum creatinine>
2 mg/dl),
스텐트 삽입술전24
시간안에 혈전용해제를사용한 환자
,
스텐트 삽입술 전후로경구용 항응고제를 복용한환자
,
약물 용출성스텐트(drug-eluting stent)
삽입술을받은환자는대상에서제외하였다
.
자료수집방법
본 연구에서는 스텐트 삽입술을 받은 환자 중에서
clopidogrel-aspirin
을 복용한 환자나cilostazol-aspirin
을 복용한 환자들의기본특징을분석하기위해 입원
,
외래 의무기록지를조사하여 다음과같은 항목을수집하였다
.
첫째,
환 자의 기본 특징을 분석하기위해 환자의 성별,
연령,
신장,
체중을기록하고 출혈의부작용을평가하기 위해 임상병리 검사 결과 중 혈액학적자료인
hemoglobin(Hgb), hematocrit (Hct), platelet(PLT)
를 스텐트 삽입술을 시행하기 전과 시행 후24
시간, 48
시간,
퇴원전일의검사치를수집하였다.
둘째,
관상동맥질환의위험인자인고혈압
,
고지혈증,
당뇨,
뇌졸중,
흡연
,
가족력,
협심증이나심근경색증의과거력,
울혈성심부 전등기저질환의여부를조사하였다.
셋째, aspirin,
β-blocker,
지질강하 약물
(lipid lowering agents), ACE inhibitor, calcium
channel blocker, nitrates, heparin
등의 병용약물의현황을조 사하였다.
넷째,
관상동맥조영술기록지(coronary angiographic
report)
나 경피적 관상동맥성형술(Percutaneous Transluminal Coronary Angioplasty,
이하PTCA)
기록지를이용하여스텐 트시술전의참조혈관내경,
최소혈관내경,
혈관의협착정도,
병변 혈관의 수와 위치
[left anterior discending(LAD), left circumflex(LCx), right coronary artery(RCA)]
를 조사하고스텐트를삽입하게된시점을응급
(urgent)
과선택(elective)
으로구분하였고스텐트삽입혈관
(target vessel),
스텐트길이,
잔 여협착률(residual stenosis)
을수집하였다.
다섯째,
스텐트삽입술을 받게 된 임상적인 적응증을 심근경색
(Q-wave, Non
Q-wave),
불안정형협심증,
안정형협심증등으로구분하여조사하였다
.
여섯째,
스텐트삽입술후재협착률을평가하기위해
6
개월 이상 지난 후에 시행한추적 관상동맥조영술의결과를관상동맥조영술기록지를통하여수집하였다
.
일곱번째,
출혈 등의 부작용에미치는 영향을파악하고자
glycoprotein b/a receptor antagonist(
이하GpIIb/IIIa receptor antagonist)
의 사용여부를조사하였다.
항혈소판 제제 투여방법
Clopidogrel
은300 mg
을부하량으로투여하거나부하량으로 투여 없이 처음부터 유지용량인
75 mg
을1
일1
회 경구 투여하였고cilostazol
은100 mg
을1
일2
회로 경구투여했으 며 두 군 모두aspirin 200 mg
을1
일1
회 투여했다.
각각의 약물은스텐트삽입술전부터1
년간경구로투여되었다.
Endpoint 평가방법 및 정의
본 연구에서는 두 가지 유형의 사건빈도를 평가하였다
.
Primary endpoint
은 추적기간 동안 두 군에서 발생한 주요심장사건
(MACE)
및관상동맥조영술상의스텐트재협착을평가하였다
. Clopidogrel-aspirin
군에서는전처치로clopidogrel
을부하량으로투여한군과비부하량투여군과의주요심장 사건의 발생 빈도수로비교
,
평가하였다.
추적 관찰은 스텐트 삽입술후
7, 30
일, 6, 12
개월 동안으로구분하여분석하였다
.
주요 심장사건은 사망
,
협심증,
심근경색증(Q-wave
또는non Q-wave),
뇌졸중,
혈관재관류(revascularization)
로정의하 였다.
모든 사망은다른 분명한사망원인이 밝혀지지 않을 경우 심장 사망으로 간주하였다.
협심증은 의무기록지에chest pain(+), angina(+)
로기록되어있는 경우로하였고,
심근경색증은
creatine kinase(
이하CK)
농도가정상 상한치의2
배 이상 증가하며CKMB
농도가 증가한 경우로 하였고,
뇌졸중은뇌출혈이나뇌경색이발생했을경우로정의하였다
.
혈관재관류는스텐트삽입술후
30
일안에반복적인중재술 또는관상동맥우회술을시행한경우는응급표적혈관재관류(urgent target revascularization), 30
일 이후에 시행한 경우는표적혈관재관류
(any target revascularization),
표적혈관이 아닌다른 혈관에 시행한 경우에는 기타혈관재관류
(any reva- scularization)
라고정의하였다.
스텐트재협착은스텐트를삽입하고
6
개월이지난 후에 추적 관상동맥조영술을시행한 환자를대상으로스텐트를삽입한관상동맥내경이관상동맥 조영술에서50%
이상좁아진경우로정의하였다.
Secondary endpoint
로 출혈의 합병증과 약물의 부작용을평가하였다
.
출혈의합병증은스텐트삽입술후7, 30
일, 12
개월 동안으로 구분하여 발생한 사건을 분석하였고 그 외 약물의 부작용은 스텐트 삽입술 후
12
개월 동안에 발생한 빈도수를 분석하였다.
출혈은major bleeding
또는minor bleeding
으로 분류하여 분석하였다5). Major bleeding
은 뇌내 출혈(intracranial bleeding),
안구내 출혈,
소화관 출혈,
수혈 을 요하는 출혈,
혈소판감소증(<100,000/mm
3),
대퇴동맥접촉부위
(access site)
의 출혈, hemoglobin
의 수치가baseline
과비교하여
3 g/dl
이상의감소가있을경우로정의하였다. Minor bleeding
은major bleeding
외에 다른 출혈(
구강내출혈,
혈종,
혈뇨등
)
로정의하였다.
영향인자 분석
Endpoint
에 영향을미칠 수 있는상관 인자들을분석하기위하여위험인자중에당뇨
,
고혈압,
고지혈증,
흡연등과병용약물인지질강하제
,
β-blocker, ACE inhibitor, calcium channel blocker, heparin, GpII b/IIIa receptor antagonist
등을multivariate analysis
방법으로분석하였다.
분석 방법
통계적 분석은
intention-to-treat
원칙에 의해 실시 되었으며 연속변수의비교는 독립표본
t-test,
범주형변수는relative risk
와95% confidence intervals(CIs)
로 나타내었고Chi-square test
또는Fisher-exact test
로 분석하였다. Time-to-event curve
는
Kaplan-Meier estimator
를 이용하였으며 각 군의 결과의 비교는log-rank test
로 분석하였다. Endpoint
에 영향을미치 는 인자를 분석하기 위한multivariate analysis
는stepwise
를이용한
logistic regression
을 사용하였다.
모든 분석은SAS 8.2 version
을이용하여p<0.05
인경우를통계적으로유의하 다고간주하였다.
결 과
대상환자의 특징
대상환자는스텐트삽입술을받은환자로서분석이가능한 환자
130
명 중clopidogrel-aspirin
군은58
명, cilostazol-aspirin
군은
72
명이었다. Clopidogrel-aspirin
군과cilostazol-aspirin
군의 평균연령
(59±10.6
세, 60±9.5
세),
성별(
남성/
여성: 39
명/19
명
, 45
명/27
명),
체중(68.3±11.4 kg, 65.5±10.7 kg), Hgb(13.7±
1.5 g/dl, 13.5±1.5 g/dl), Hct(40.2±4.7%, 40.4±4.3%), PLT(249.4
±70.1×10
3mm, 265.8±69.2×10
3mm)
등 기본 특성은 두 군간 에 유사하였다.
스텐트를 삽입을 하게 된 임상 진단명은clopidogrel-aspirin
군에서는 심근경색증이19
명(32.7%),
불안정형 협심증이
35
명(60.3%),
안정형협심증이4
명(6.9%)
였고, cilostazol-aspirin
군에서는심근경색증이26
명(36.1%),
불안정 형 협심증이44
명(61.1%),
안정형 협심증이2
명(2.8%)
으로 두 군간에 차이가 없었다.
그 외 두 군간의 환자 특성은Table 1
과 같다.
관상동맥 위험인자인뇌졸중은clopidogrel- aspirin
군에서만8
명(13%)
으로clopidogrel-aspirin
군에서 유의하게 많았다
(p<0.0012).
그 외위험인자간에는차이가없 었다(Table 1).
병용약물
Clopidogrel-aspirin
군과cilostazol-aspirin
군에서의 스텐트 삽입술 후ACE inhibitor
의 사용은 각각38
명(65.5%), 59
명(83.1%) [p=0.02], calcium channel blocker
의 사용은 각각27
명(46.6%), 46
명(64.8%) [p=0.03]
으로cilostazol-aspirin
군에서유의하게더많이사용하였으며
,
스텐트삽입술후heparin
의 투여는유의한차이는 없지만
cilostazol-aspirin
군에서많 이사용한것으로나타났다(p=0.08)(Table 1).
관상동맥조영술의 특징
스텐트시술전의참조혈관내경
,
최소혈관내경,
협착률,
병변혈관의 분포
,
병변혈관의 수 등의 비교에서는 두 군간에 유의한차이는없었다(Table 1).
스텐트 시술의 특징
삽입한 스텐트의 수
,
스텐트의길이,
스텐트삽입의과정 등에는차이가없었고스텐트를삽입한표적혈관은LAD
나RCA
는 차이가 없었지만LCx
는cilostazol-aspirin
군에서 더유의하게많았다
(p=0.03)(Table 2).
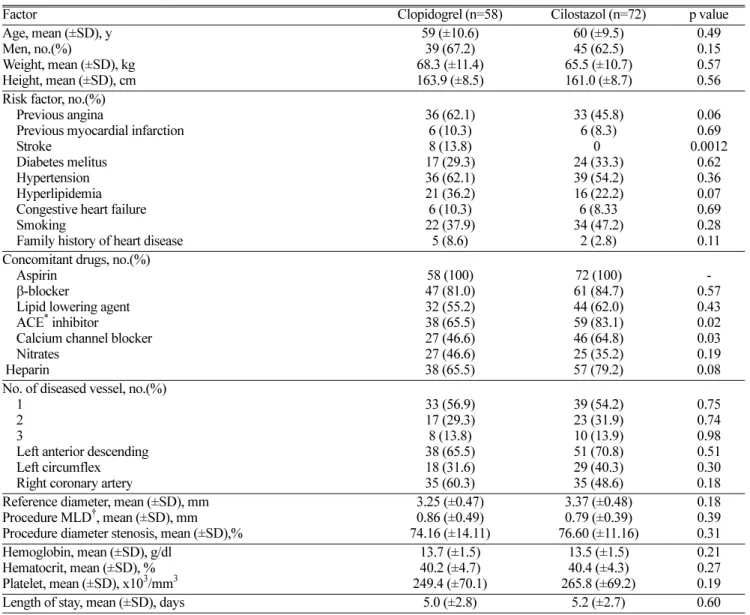
Table 1. Baseline demographics
Factor Clopidogrel (n=58) Cilostazol (n=72) p value
Age, mean (±SD), y Men, no.(%)
Weight, mean (±SD), kg Height, mean (±SD), cm
59 (±10.6) 39 (67.2) 68.3 (±11.4) 163.9 (±8.5)
60 (±9.5) 45 (62.5) 65.5 (±10.7) 161.0 (±8.7)
0.49 0.15 0.57 0.56 Risk factor, no.(%)
Previous angina
Previous myocardial infarction Stroke
Diabetes melitus Hypertension Hyperlipidemia Congestive heart failure Smoking
Family history of heart disease
36 (62.1) 6 (10.3) 8 (13.8) 17 (29.3) 36 (62.1) 21 (36.2) 6 (10.3) 22 (37.9)
5 (8.6)
33 (45.8) 6 (8.3) 24 (33.3) 0 39 (54.2) 16 (22.2) 6 (8.33 34 (47.2)
2 (2.8)
0.06 0.69 0.0012
0.62 0.36 0.07 0.69 0.28 0.11 Concomitant drugs, no.(%)
Aspirin
β
-blocker
Lipid lowering agent ACE
*inhibitor
Calcium channel blocker Nitrates
Heparin
58 (100) 47 (81.0) 32 (55.2) 38 (65.5) 27 (46.6) 27 (46.6) 38 (65.5)
72 (100) 61 (84.7) 44 (62.0) 59 (83.1) 46 (64.8) 25 (35.2) 57 (79.2)
0.57 - 0.43 0.02 0.03 0.19 No. of diseased vessel, no.(%) 0.08
1 2
3 Left anterior descending Left circumflex Right coronary artery
33 (56.9) 17 (29.3) 8 (13.8) 38 (65.5) 18 (31.6) 35 (60.3)
39 (54.2) 23 (31.9) 10 (13.9) 51 (70.8) 29 (40.3) 35 (48.6)
0.75 0.74 0.98 0.51 0.30 0.18 Reference diameter, mean (±SD), mm
Procedure MLD
†, mean (±SD), mm Procedure diameter stenosis, mean (±SD),%
3.25 (±0.47) 0.86 (±0.49) 74.16 (±14.11)
3.37 (±0.48) 0.79 (±0.39) 76.60 (±11.16)
0.18 0.39 Hemoglobin, mean (±SD), g/dl 0.31
Hematocrit, mean (±SD), % Platelet, mean (±SD), x10
3/mm
313.7 (±1.5) 40.2 (±4.7) 249.4 (±70.1)
13.5 (±1.5) 40.4 (±4.3) 265.8 (±69.2)
0.21 0.27
Length of stay, mean (±SD), days 5.0 (±2.8) 5.2 (±2.7) 0.19 0.60
*
ACE=angiotensin convert enzyme ,
†MLD=minimal luminal diameter
Primary endpoint
스텐트삽입술 후 임상추적의 분석 결과는
Table 3
과 같 다.
스텐트 삽입술후7
일동안 주요 심장사건의총발생은clopidogrel-aspirin
군에서1
명(1.7%), cilostazol-aspirin
군에서1
명(1.4%)
으로유의한차이가없었다(p=1.0).
두군모두관 상동맥 중재술이 필요하였던 경우는 없었으나cilostazol- aspirin
군에서스텐트삽입술후1
명(1.4%)
이4
일째심장쇽으 로 사망했다.
스텐트삽입술후30
일 동안주요 심장사건의 총 발생은clopidogrel-aspirin
군에서3
명(5.2%), cilostazol- aspirin
군에서3
명(4.2%)
으로 유의한차이가 없었고(p=0.79),
협심증을 제외한 주요 심장사건의 총 발생은
clopidogrel- aspirin
군에1
명(1.7%), cilostazol-aspirin
군에서2
명(2.8%)
으로 차이가 없었다(p=0.69).
협심증의 발생률은clopidogrel- aspirin
군에서2
명(3.5%), cilostazol-aspirin
군에서1
명(1.4%)
으로 유의한 차이가 없었고
(p=0.44),
두 군 모두 관상동맥중재술이 필요하였던 경우는없었으나
cilostazol-aspirin
군에서1
명이15
일째뇌경색이발생하였다.
스텐트삽입술후
6
개월동안주요심장사건의총발생은clopidogrel-aspirin
군에서6
명(10.3%), cilostazol-aspirin
군에서19
명(26.4%)
으로cilostazol-aspirin
군에서 유의하게 높았지만(p=0.021),
협심증을제외한주요심장사건의총발생은유의한 차이가 없었다
(p=0.29).
협심증의 발생률은clopidogrel- aspirin
군에서4
명(6.9%), cilostazol-aspirin
군에서16
명(22.2%)
으로
cilostazol-aspirin
군에서 유의하게 높았으며(p=0.016), cilostazol-aspirin
군에서5
개월째뇌경색이1
명더발생했으나유의한 차이는 없었다
.
관상동맥중재술은 총9
명으로clopidogrel-aspirin
군에서3
명(5.2%), cilostazol-aspirin
군에서6
명(8.3%)
으로유의한차이는나타내지않았으며(p=0.73),
두 군모두응급표적혈관재관류는시행되지않았고표적혈관재 관류는clopidogrel-aspirin
군과cilostazol-aspirin
군에서 각각2
명(3.5%), 3
명(4.2%),
기타혈관재관류는 각각1
명(1.7%), 3
명
(4.2%)
으로각각의항목에서도유의한차이를나타내지않았다
.
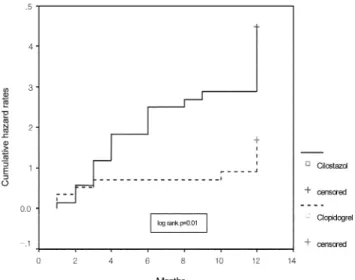
스텐트 삽입 후
12
개월 동안의 주요 심장사건의총 발생 은clopidogrel-aspirin
군에서9
명(15.5%), cilostazol-aspirin
군에서
26
명(36.2%)
으로cilostazol-aspirin
군에서유의하게높았으며
(p=0.0085),
협심증을제외한 주요 심장사건의 총 발생과 협심증발생 빈도는
cilostazol-aspirin
군에서유의하게높 았다(p=0.036, p=0.021)(Table 3, Figures 1, 2).
그러나 심근 경색증,
뇌졸중,
혈관재관류의 발생율은 두 군간에 유의한 차이가없었다.
스텐트 재협착
연구기간동안에 추적 관상동맥조영술은 스텐트삽입술 후 평균
7
개월째에clopidogrel-aspirin
군에서는21
명(36.2%), cilostazol-aspirin
군 에서는28(38.8%)
명이실시하였다.
스텐 트를 삽입한 관상동맥의 내경이 관상동맥 조영술에서50%
이상 좁아진 경우는
clopidogrel-aspirin
군에서3
명(14.3%), cilostazol-aspirin
군에서9
명(32.1%)
으로 나타났으나 두 군간 에유의한차이는없었다(p=0.19)(Table 6).
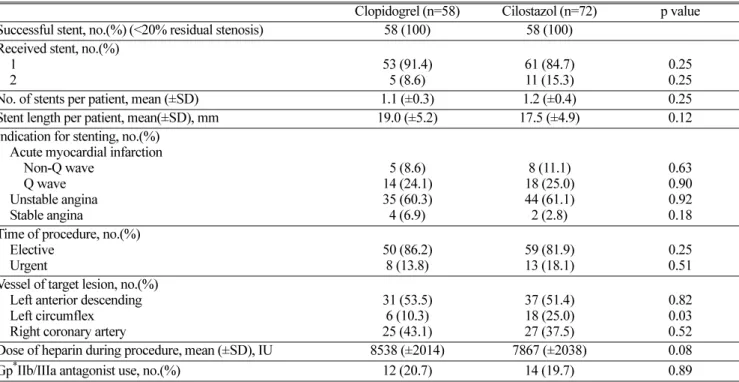
Table 2. Procedural characteristics
Clopidogrel (n=58) Cilostazol (n=72) p value Successful stent, no.(%) (<20% residual stenosis) 58 (100) 58 (100)
Received stent, no.(%)
1 2 53 (91.4)
5 (8.6) 61 (84.7)
11 (15.3) 0.25
No. of stents per patient, mean (±SD) 1.1 (±0.3) 1.2 (±0.4) 0.25 0.25
Stent length per patient, mean(±SD), mm 19.0 (±5.2) 17.5 (±4.9) 0.12
Indication for stenting, no.(%) Acute myocardial infarction
Non-Q wave Q wave Unstable angina Stable angina
5 (8.6) 14 (24.1) 35 (60.3) 4 (6.9)
8 (11.1) 18 (25.0) 44 (61.1) 2 (2.8)
0.63 0.90 0.18 0.92 Time of procedure, no.(%)
Elective
Urgent 50 (86.2)
8 (13.8) 59 (81.9)
13 (18.1) 0.25
Vessel of target lesion, no.(%) 0.51 Left anterior descending Left circumflex Right coronary artery
31 (53.5) 6 (10.3) 25 (43.1)
37 (51.4) 18 (25.0) 27 (37.5)
0.82 0.03 Dose of heparin during procedure, mean (±SD), IU 8538 (±2014) 7867 (±2038) 0.52 0.08
Gp
*IIb/IIIa antagonist use, no.(%) 12 (20.7) 14 (19.7) 0.89
*Gp=glycoprotein
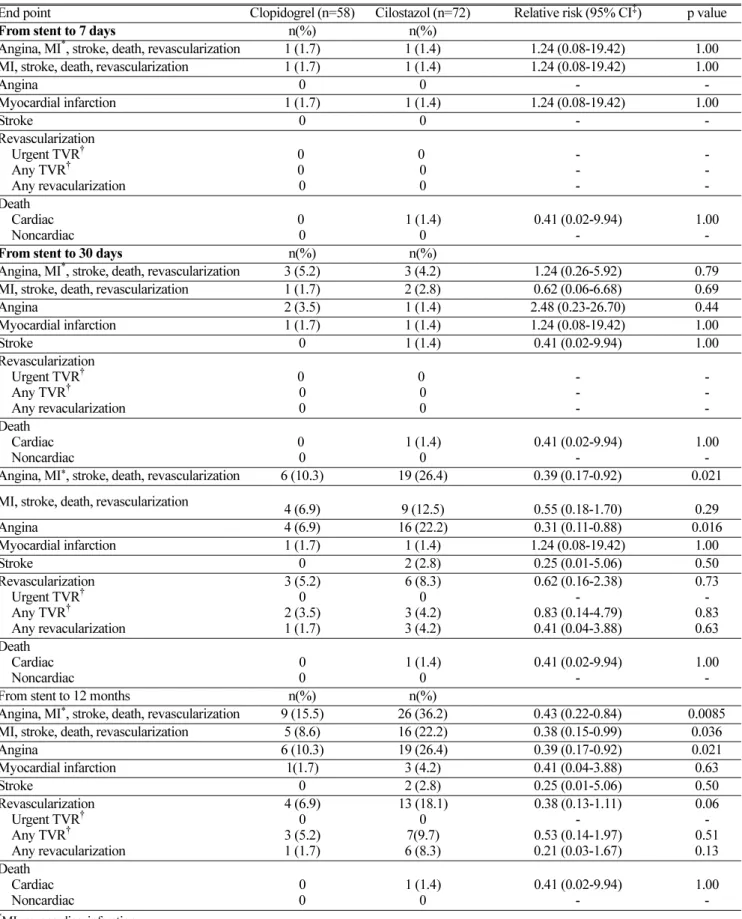
Table 3. Primary endpoint
End point Clopidogrel (n=58) Cilostazol (n=72) Relative risk (95% CI
‡) p value
From stent to 7 days n(%) n(%)
Angina, MI
*, stroke, death, revascularization 1 (1.7) 1 (1.4) 1.24 (0.08-19.42) 1.00
MI, stroke, death, revascularization 1 (1.7) 1 (1.4) 1.24 (0.08-19.42) 1.00
Angina 0 0 - -
Myocardial infarction 1 (1.7) 1 (1.4) 1.24 (0.08-19.42) 1.00
Stroke 0 0 - -
Revascularization Urgent TVR
†Any TVR
†Any revacularization
0 0 0
0 0 0
- - -
- - Death -
Cardiac
Noncardiac 0
0 1 (1.4)
0 0.41 (0.02-9.94)
- 1.00
From stent to 30 days n(%) n(%) -
Angina, MI
*, stroke, death, revascularization 3 (5.2) 3 (4.2) 1.24 (0.26-5.92) 0.79
MI, stroke, death, revascularization 1 (1.7) 2 (2.8) 0.62 (0.06-6.68) 0.69
Angina 2 (3.5) 1 (1.4) 2.48 (0.23-26.70) 0.44
Myocardial infarction 1 (1.7) 1 (1.4) 1.24 (0.08-19.42) 1.00
Stroke 0 1 (1.4) 0.41 (0.02-9.94) 1.00
Revascularization Urgent TVR
†Any TVR
†Any revacularization
0 0 0
0 0 0
- - -
- - Death -
Cardiac
Noncardiac 0
0 1 (1.4)
0 0.41 (0.02-9.94)
- 1.00
Angina, MI
*, stroke, death, revascularization 6 (10.3) 19 (26.4) 0.39 (0.17-0.92) 0.021 -
MI, stroke, death, revascularization 4 (6.9) 9 (12.5) 0.55 (0.18-1.70) 0.29
Angina 4 (6.9) 16 (22.2) 0.31 (0.11-0.88) 0.016
Myocardial infarction 1 (1.7) 1 (1.4) 1.24 (0.08-19.42) 1.00
Stroke 0 2 (2.8) 0.25 (0.01-5.06) 0.50
Revascularization Urgent TVR
†Any TVR
†Any revacularization
3 (5.2) 2 (3.5) 0 1 (1.7)
6 (8.3) 3 (4.2) 0 3 (4.2)
0.62 (0.16-2.38) 0.83 (0.14-4.79) - 0.41 (0.04-3.88)
0.73 - 0.83 0.63 Death
Cardiac
Noncardiac 0
0 1 (1.4)
0 0.41 (0.02-9.94)
- 1.00
From stent to 12 months n(%) n(%) -
Angina, MI
*, stroke, death, revascularization 9 (15.5) 26 (36.2) 0.43 (0.22-0.84) 0.0085
MI, stroke, death, revascularization 5 (8.6) 16 (22.2) 0.38 (0.15-0.99) 0.036
Angina 6 (10.3) 19 (26.4) 0.39 (0.17-0.92) 0.021
Myocardial infarction 1(1.7) 3 (4.2) 0.41 (0.04-3.88) 0.63
Stroke 0 2 (2.8) 0.25 (0.01-5.06) 0.50
Revascularization Urgent TVR
†Any TVR
†Any revacularization
4 (6.9) 3 (5.2) 0 1 (1.7)
13 (18.1) 7(9.7) 0 6 (8.3)
0.38 (0.13-1.11) 0.53 (0.14-1.97) - 0.21 (0.03-1.67)
0.06 - 0.51 0.13 Death
Cardiac
Noncardiac 0
0 1 (1.4)
0 0.41 (0.02-9.94)
- 1.00
-
*
MI=myocardiac infarction
†
TVR=target vessel revascularization
‡
CI=confidence interval
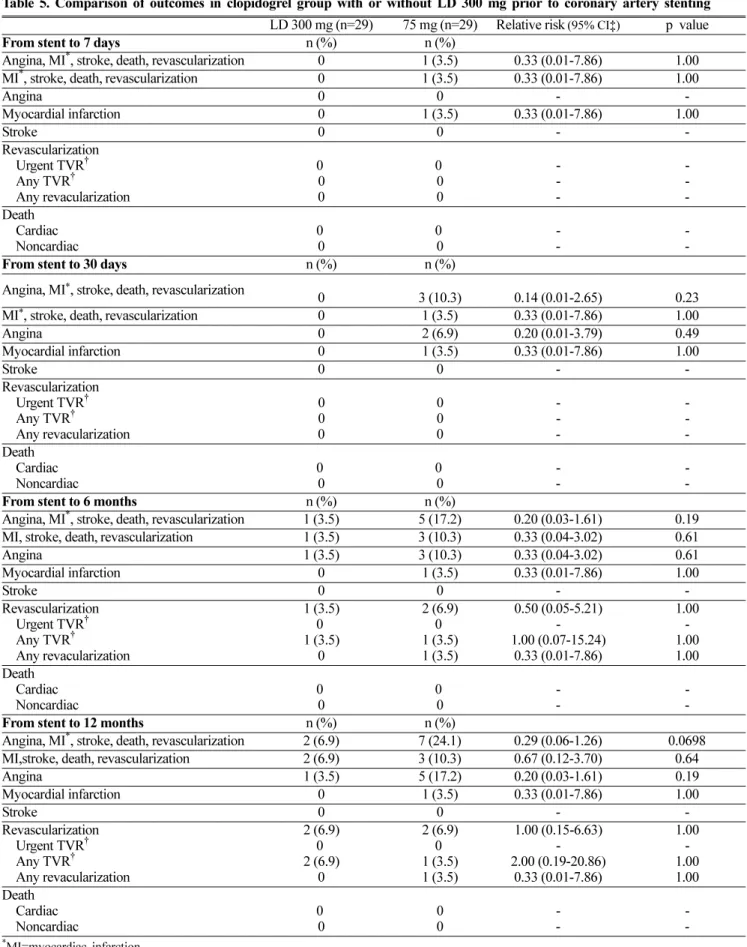
Clopidogrel 부하량으로 전처치 시의 endpoint
Clopidogrel-aspirin
군에서300 mg
의부하량을투여한환자 수는29
명(50%)
이었고부하량없이75 mg
을투여한환자는9
명(50%)
이었다.
모든평가항목에서유의한차이는없었으나스텐트삽입 술 후
7
일과30
일 동안의 주요 심장사건의 발생은75 mg
비부하량투여군에서만
1
명 발생하였고6
개월 동안의주요 심장사건의 총 발생은300 mg
부하량투여군이75 mg
비 부하량 투여군보다적게 나타났다[1(3.5%) vs 5(17.2%), RR 0.20(0.03-1.61)].
협심증을제외한 주요 심장사건의총 발생 에서도 부하량을 투여 받은 환자군에서 적게 나타났다[1(3.5%) vs 3(10.3%), RR 0.33(0.04- 3.02)].
또한 스텐트삽입술 후
12
개월 동안의주요 심장사건의총 발생은300 mg
부하량 투여군이
75 mg
비부하량투여군보다 적게 나타났다
[2(6.9%) vs 7(24.1%), RR 0.29(0.06-1.26)](Table 5).
Secondary endpoint
Major bleeding
의발생률은두군간에유의한차이가없었고
[9
명(15.5%) vs 10
명(13.9%), p=0.79]
두 군 모두 뇌내 출혈이나안구 출혈,
혈소판감소증은 없었다.
대부분의출 혈성합병증은스텐트삽입후7
일안에 발생했으며소화관 출혈은clopidogrel-aspirin
군에서만18
일째1
명에서발생했다.
Minor bleeding
의발생률도두군간에유의한차이가없었으며
(p=0.75),
두 군 모두 혈종이2
명씩 나타났고 구강출혈은clopidogrel-aspirin
군에서만2
명,
혈뇨는cilostazol-aspirin
군에서만
2
명으로나타났다.
두군모두그외다른출혈은관찰 할수 없었다. Gpb/a receptor antagonist
를투여한환자나투 여하지않은 환자들간의출혈의합병증은유사하였다(Table 7).
약물의 부작용으로 투약을 조기 중단해야 하는 경우는 없었고clopidogrel-aspirin
군에서는두통이1
명,
현훈이1
명에서 나타났고
cilostazol-aspirin
군에서는 소화기 장애가3
명,
두통이
3
명,
빈맥이3
명,
현훈이3
명에서나타났다(Table 4).
영향인자 분석
Multivariate analysis
분석에서endpoint
에 유의성있게 영 향을미칠수있는인자는없었다.
고 찰
관상동맥질환의치료로관상동맥스텐트삽입술은최근널 리 시술되고있으나 스텐트 삽입 후 발생하는스텐트혈전 증이나재협착을예방하기위하여항혈소판제제를투여하는 것은 중요하다
. 2001 American College of Chest Physicians
VI
지침서23)에 의하면 스텐트 삽입후에 항혈전증 제제인aspirin 80-325 mg/day
와ticlopidine
부하량500 mg
을 투여 후 유지량으로250 mg
을1
일2
회10-14
일 투여하거나clopidogrel
부하량300 mg
을 투여 후 유지량으로75 mg
을투여하도록 추천하고 있다
.
스텐트 시술 중에는heparin
을 투여하고고위험군에서는GpIIb/IIIa receptor antagonist
를투 여하고ticlopidine
을 사용할 경우ticlopidine
으로 인해 나타 날 수있는 혈액학적부작용인중성구감소증,
혈소판감소 증,
간독성을모니터링하도록권고하고있다.
따라서이러한ticlopidine
의안전성의문제점을해결할수있는 대체약물이요구되어져 왔고 최근
clopidogrel
과cilostazol
이 대두되고 있다5,12-15).
Clopidogrel
과cilostazol
은작용기전상서로 다른항혈소판 제제로그동안표준요법으로사용된ticlopidine
을대조군으로 하여 비교한 여러 연구가 발표되어 있다
. Ticlopidine
과cilostazol
을비교한연구로서는Park
등12), Yoon
등13), Kozuma Fig. 1. Kaplan-Meier cumulative hazard rates for angina,
myocardial infarction, stroke, death, or revascularization.
Fig. 2. Kaplan-Meier cumulative hazard rates for myocardial
infarction, stroke, death, or revascularization.
등14)
, Kamishirado
등15)이 있고ticlopidine
과clopidogrel
을 비 교한 연구는CLASSICS
5), Pache
22)등의연구가 있다.
이연 구들의 결과에의하면cilostazol
과clopidogrel
의 두 약물모두가
ticlopidine
에 비해 동등이상의 효과와 안전성이 있는약물인것으로보고되고있다
. Lee
등32)에의하면스텐트삽입술 후
cilostazol
과clopidogrel
을 각각30
일 동안 투여한 환자를 대상으로30
일 동안의 추적 관찰한 결과를 보면cilostazol
은clopidogrel
만큼 안전하고 효과적인 약물이라고 Table 4. Secondary endpointClopidogrel (n=58) Cilostazol (n=72) Relative risk (95% CI
†) p value
From stent to 7 days n(%) n(%)
Bleeding complication Major bleeding
Intracranial Intraocular GI
*bleeding Access site
Decreased hemoglobin Thrombocytopenia Blood transfusion Minor bleeding
Hematoma Hematuria Oral
8 (13.8) 0 0 3 (5.2) 0 5 (8.6) 3 (5.2) 0 4 (6.9) 2 (3.5) 2 (3.5) 0
10 (13.9) 0 0 1 (1.4) 0 7 (9.7) 3 (4.2) 0 3 (4.2) 2 (2.8) 1 (1.4) 0
0.99 (0.42-2.35) - - 3.72 (0.40-34.9) - 0.89 (0.30-2.65) 1.21 (0.26-5.92) - 1.66 (0.39-7.10) 1.24 (0.18-8.55) 0.41 (0.02-9.94) 6.19(0.30-126.38)
0.99 - - - 0.32 0.83 0.78 - 0.70 0.83 1.00 0.20 From stent to 30 days
Bleeding complication Major bleeding
Intracranial Intraocular GI
*bleeding Access site
Decreased hemoglobin Thrombocytopenia Blood transfusion Minor bleeding
Hematoma Hematuria Oral
9 (15.5) 0 0 1 (1.7) 3 (5.2) 6 (10.3)
4 (6.9) 0 4 (6.9) 2 (3.5) 2 (3.5) 0
10 (13.9) 0 0 1 (1.4) 0 7 (9.7) 3 (4.2) 0 4 (5.6) 2 (2.8) 2 (2.8) 0
1.11 (0.49-2.57) - - 3.72 (0.15-89.45) 3.72 (0.40-34.86) 1.06 (0.38-2.92) 1.66 (0.39-7.10) - 1.24 (0.32-4.75) 1.24 (0.18-8.55) 0.25 (0.01-5.06) 6.19(0.30-126.38)
0.79 - 0.45 - 0.32 0.91 0.70 - 0.75 0.83 0.50 0.20 From stent to 12 months
Bleeding complication Major bleeding
Intracranial Intraocular GI
*bleeding Access site
Decreased hemoglobin Thrombocytopenia Blood transfusion Minor bleeding
Hematoma Hematuria Oral Other side effects Skin disorder GI
*disturbance Headache Palpitation Dizziness
9 (15.5) 0 0 1 (1.7) 3 (5.2) 6 (10.3)
4 (6.9) 0 4 (6.9) 2 (3.5) 2 (3.5) 0
0 0 1 (1.7) 1 (1.7) 0
10 (13.9) 0 0 1 (1.4) 0 7 (9.7) 3 (4.2) 0 4 (5.6) 2 (2.8) 2 (2.8)
0 3 (4.2) 0 3 (4.2) 3 (4.2) 3 (4.2)
1.11 (0.49-2.57) - - 3.72 (0.15-89.45) 3.72 (0.40-34.86) 1.06 (0.38-2.92) 1.66 (0.39-7.10) - 1.24 (0.32-4.75) 1.24 (0.18-8.55) 0.25 (0.01-5.06) 6.19(0.30-126.38)
0.18 (0.01-3.35) - 0.41 (0.04-3.87) 0.18 (0.01-3.35) 0.41 (0.04-3.87)
0.79 - 0.45 - 0.32 0.91 0.70 - 0.75 0.83 0.50 0.20 0.25 - 0.63 0.25 0.63
*GI=gastrointestinal
†CI=confidence interval
Table 5. Comparison of outcomes in clopidogrel group with or without LD 300 mg prior to coronary artery stenting LD 300 mg (n=29) 75 mg (n=29) Relative risk (95% CI‡) p value
From stent to 7 days n (%) n (%)
Angina, MI
*, stroke, death, revascularization 0 1 (3.5) 0.33 (0.01-7.86) 1.00
MI
*, stroke, death, revascularization 0 1 (3.5) 0.33 (0.01-7.86) 1.00
Angina 0 0 - -
Myocardial infarction 0 1 (3.5) 0.33 (0.01-7.86) 1.00
Stroke 0 0 - -
Revascularization Urgent TVR
†Any TVR
†Any revacularization
0 0 0
0 0 0
- - -
- - Death -
Cardiac
Noncardiac 0
0 0
0 -
- -
From stent to 30 days n (%) n (%) -
Angina, MI
*, stroke, death, revascularization 0 3 (10.3) 0.14 (0.01-2.65) 0.23
MI
*, stroke, death, revascularization 0 1 (3.5) 0.33 (0.01-7.86) 1.00
Angina 0 2 (6.9) 0.20 (0.01-3.79) 0.49
Myocardial infarction 0 1 (3.5) 0.33 (0.01-7.86) 1.00
Stroke 0 0 - -
Revascularization Urgent TVR
†Any TVR
†Any revacularization
0 0 0
0 0 0
- - -
- - Death -
Cardiac
Noncardiac 0
0 0
0 -
- -
From stent to 6 months n (%) n (%) -
Angina, MI
*, stroke, death, revascularization 1 (3.5) 5 (17.2) 0.20 (0.03-1.61) 0.19
MI, stroke, death, revascularization 1 (3.5) 3 (10.3) 0.33 (0.04-3.02) 0.61
Angina 1 (3.5) 3 (10.3) 0.33 (0.04-3.02) 0.61
Myocardial infarction 0 1 (3.5) 0.33 (0.01-7.86) 1.00
Stroke 0 0 - -
Revascularization Urgent TVR
†Any TVR
†Any revacularization
1 (3.5) 1 (3.5) 0 0
2 (6.9) 1 (3.5) 0 1 (3.5)
0.50 (0.05-5.21) 1.00 (0.07-15.24) -
0.33 (0.01-7.86)
1.00 - 1.00 1.00 Death
Cardiac
Noncardiac 0
0 0
0 -
- -
From stent to 12 months n (%) n (%) -
Angina, MI
*, stroke, death, revascularization 2 (6.9) 7 (24.1) 0.29 (0.06-1.26) 0.0698
MI,stroke, death, revascularization 2 (6.9) 3 (10.3) 0.67 (0.12-3.70) 0.64
Angina 1 (3.5) 5 (17.2) 0.20 (0.03-1.61) 0.19
Myocardial infarction 0 1 (3.5) 0.33 (0.01-7.86) 1.00
Stroke 0 0 - -
Revascularization Urgent TVR
†Any TVR
†Any revacularization
2 (6.9) 2 (6.9) 0 0
2 (6.9) 1 (3.5) 0 1 (3.5)
1.00 (0.15-6.63) 2.00 (0.19-20.86) -
0.33 (0.01-7.86)
1.00 - 1.00 1.00 Death
Cardiac
Noncardiac 0
0 0
0 -
- -
*
MI=myocardiac infarction -
†
TVR=target vessel revascularization
‡