Prediction of Subsequent Vertebral Collapse after Osteoporotic Thoracolumbar Vertebral Fractures
SeJun Park, SungSoo Chung
Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Objectives: To evaluate the clinical significance of vertebral bone bruise (VBB) in terms of subsequent collapse after osteoporotic thoracolumbar vertebral fractures.
Methods: We reviewed 41 consecutive patients with 46 osteoporotic thoracolumbar vertebral fractures treated nonoperatively from March 2007 to February 2010. Anterior wedge angle (AWA) was measured on plain radiographs and the change of AWA between the initial and last measurement was used to represent the subsequent vertebral collapse. The size of VBB was measured and VBB ratio was calculated on T1-weighted sagittal MR image.
Results: The average VBB ratio was 49.1% and the average change of AWA was 7.1o. Only VBB ratio significantly correlated with the change of AWA (P<0.001, cc=0.660). The other factors such as age, initial AWA, and endplate status showed no significant correlation with the change of AWA (P=0.629, P=0.724, P=0.690, respectively). In DEXA group, no correlation was found between T-score and the change of AWA as well as between T-score and VBB ratio (P=0.548, P=0.370, respectively). Five fractures were diagnosed as delayed post-traumatic vertebral collapse. Their average VBB ratio was 71.2% which was significantly higher than that of the other subjects (P=0.015). The fractures with VBB ratio more than 60% was likely to progress to delayed post-traumatic vertebral collapse.
Conclusions: VBB after osteoporotic thoracolumbar vertebral fracture was significantly correlated with subsequent vertebral collapse (cc=0.660). We recommend the patients with a large vertebral bone bruise, especially more than 60%, should be followed up meticulously for the early detection of delayed post-traumatic vertebral collapse.
Key Words: Delayed post-traumatic vertebral collapse, Osteoporotic thoracolumbar vertebral fracture, Predictor, Subsequent vertebral collapse, Vertebral bone bruise
Received: June 27, 2011 Revised: July 17, 2011 Accepted: July 26, 2011
Corresponding Author: SungSoo Chung, Samsung Medical Center, Sungkyunkwan University School of Medicine, 50 Ilwon- dong, Gangnam-gu, Seoul 135-710, Korea
Tel: +82-2-3410-0385, Fax: +82-2-3410-0061 E-mail: [email protected]
Bone bruise, known as the result of trabecular microfracture, is defined on magnetic resonance (MR) images as a region with an edema signal intensity in subchondral bone and marrow in post-traumatic
patients, that is, low-signal intensity on T1-weighted images and high-signal intensity on T2-weighted images.1 Several studies have been conducted to elucidate the histopathology, natural history, and clinical consequences of bone bruise after the acute knee injury.2-7 Histological evaluation of bone bruise in the knee revealed microfractures of cancellous bone, edema and bleeding in the fatty marrow.4 It is known that bone bruise disappears from MR images within 2~4 months of injury without any obvious osseous long-
term sequelae.3,7
It is not uncommon to encounter vertebral bone bruise (VBB) following acute osteoporotic thoraco- lumbar vertebral fractures. However, little information is available about the clinical significance post- traumatic VBB. Since MRI has played a role in vertebral fractures as a most sensitive initial imaging modality, it became possible to depict the injuries to vertebral body and endplates accurately.8-11 Teli et al.
examined 30 non-fractured levels which showed VBB in MRI after a thoracolumbar vertebral fracture. They found VBBs incidentally found at non-fractured levels did not cause significant progressive vertebral deformity or bone-implant interface failure.12 To the best of our knowledge, no reports have been previously issued about VBB at the fracture level and its subsequent effect in patients with osteoporotic thoracolumbar vertebral fractures.
Most vertebral fractures usually do not exhibit serious spinal canal compromise or segmental instability, but vertebral fractures, especially those resulting from osteoporosis, may lead to gradual collapse of vertebral body, ultimately resulting in progressive kyphosis and prolonged back pain and/or neurologic deficit. This is called delayed post-traumatic vertebral collapse and is also referred to as vertebral pseudoarthrosis or osteo- necrosis. However, its underlying mechanism and patho- genesis is still poorly understood.
The purpose of this study was to evaluate the effect of VBB in terms of subsequent vertebral collapse by comparing the anterior wedge angle (AWA) at initial and last measurement. In addition, the other factors such as sex, age, bone quality, the status of endplate, and initial AWA that might affect subsequent collapse after injury were investigated. The hypothesis is that the fractured vertebrae with larger VBB are more susceptible to subsequent collapse.
MATERIALS AND METHODS
1. Subjects
This study was conducted after obtaining approval from IRB. In the present study, we reviewed the 52 patients with acute osteoporotic thoracolumbar compression or burst fractures necessitating active treatment (operative or conservative) from March 2007 to February 2010. Osteoporosis was defined as T-score below -2.5 in DEXA study. Patients with pathologic fractures including malignancy and infection were excluded. Eleven patients who had operations, including vertebroplsty or kyphoplasty, within 6 weeks were excluded in order to ensure uninhibited evaluation of the effect on VBB over time. Thus, 41 patients who were treated conservatively for more than 6 weeks after trauma were included for current study.
2. Treatment
Decisions regarding treatment options were taken by one of two senior orthopedic spine surgeons using the AO classification.13 Patients with type A1, A2, or A3 fractures without neurologic involvement were consi- dered to be treated conservatively. All patients followed the same treatment protocol. Conservative treatment consisted of immediate ambulation with a removable brace (a TLSO or a corset depending on the fractured level) for 3 months. Patients were allowed to ambulate as soon as possible to avoid long-standing bed rest.
During follow-up, if the fractures became unstable and caused disabling back pain or a neurologic deficit, surgery was perfomed.
3. Radiographic evaluation
At the first visit to our clinic, both standing plain radiographs and MRI were taken. The mean time from trauma to imaging study was 8.4 days. The same plain radiographs were obtained at 3 weeks, 6 weeks, 3 months, 6 months, 1 year and annually thereafter.
AWA, which is defined as the angle between superior
Fig. 1. Measurement of anterior wedge angle (AWA).
ΔAWA was calculated in the following way : ΔAWA (o)=AWA in Fig. B - AWA in Fig. A.
Left panel: the initial measurement. Right panel: the last measurement
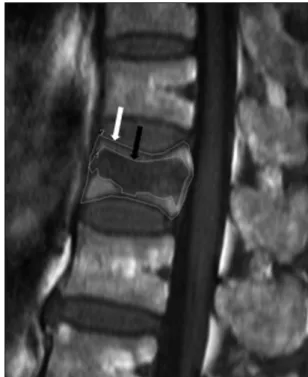
Fig. 2. Measurement of VBB ratio. Using area calcu- lation tool in PACS, both VBB (black arrow) and corresponding vertebral body (white arrow) were outlined. In this picture the size of VBB was 268.8 mm2, the size of corresponding ver- tebral body was 487.2 mm2, so VBB ratio was calculated to 55.2%.
end plate and inferior end plate of fractured vertebral body on standing lateral radiographs, was measured using PACS (CentricityⓇ, GE healthcare IT, Barrington, IL, USA). Radiographic measurement was supposed to complete when an operation was performed for any reason or when AWA did not increase on the two consecutive measurements. The extent of subsequent vertebral collapse was evaluated using the difference of AWA (ΔAWA) between the initial and last measure- ments (Fig. 1). The development of delayed post- traumatic vertebral collapse was observed during follow-up.
A 1.5 T-MRI (SignaⓇ, GE Medical Systems, Milwaukee, WI, USA) was performed for all patients.
Spin echo T1-weighted (350~700/10~40 [TR/TE]) and fast spin echo T2-weighted (2400~5000/70~120 [TR/TE]) images were obtained in the sagittal and axial planes. The size of VBB was measured quantitatively on the sagittal T1-weighted image, in which VBB was found most prominent, using the area calculation tool in PACS. To compensate for individual variations in size of vertebral body, VBB ratio was calculated in the following way : VBB ratio (%) = (size of VBB / size of corresponding vertebral body) × 100 (Fig. 2).
We evaluated the effect of the status of endplates on
subsequent collapse. Endplates were categorized to 4 grades on T2-weighted image as described by Oner et al9 where grade 1 represented only plastic deformity of the endplate, grade 2 and 3 disruptions of the anterior and posterior halves of the endplate, respectively, and grade 4 disruption of the whole endplate. To analyze the effect of endplate, we used endplate (EP) scores by endowing each endplate with the same value as endplate grade, then summarizing them.
Bone mineral density (BMD) was determined by Dual-Energy X-ray Absorptiometry (DEXA) system (Hologic scannerⓇ, Hologic inc., Bedford, MA, USA).
DEXA was performed for all patients in the current study.
4. Analysis
Comprehensive patient demographic data such as
A B
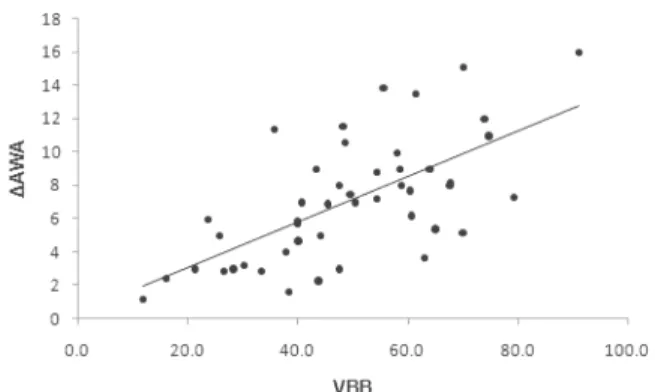
Fig. 3. Graphs showing significant correlation between VBB ratio and ΔAWA.
Table 1. Patient demographics No. of patients (M:F) 41 (6:35) No. of fractured level 46
Average T-score -3.4±0.7 (range, -2.5~5.0) Average age (years old) 67.2±7.4 (range, 56~88) Average VBB ratio (%) 49.1±17.5 (range, 11.7~91.0) Average ΔAWA (o) 7.1±3.7 (range, 1.2~16.0)
age, sex, fractured level, and fracture type were obtained. All radiographic measurements were repeated 2 weeks apart in order to assess the intraobserver agreement. Intraclass correlation for VBB ratio, initial AWA and ΔAWA and Kappa statistics for EP score were used to describe the intraobsever reliability. All intraclass correlation coefficients were greater than 0.87 and Kappa value was 0.91. The relationship between VBB ratio and ΔAWA was evaluated and the effect of other factors such as sex, age, endplate status and initial AWA on subsequent collapse were also investi- gated. The relationship between T-score and ΔAWA, between T-score and VBB was also evaluated. Spearman’s correlation test was used throughout the analysis and correlation coefficient was calculated. Fisher’s exact test with minimum p-value approach was used to compare the occurrence rate of delayed post-traumatic vertebral collapse according to VBB ratio. A statistical software package (SAS ver. 9.1.3, SAS Institute Inc., Cary, NC, USA and R. ver. 2.11.1, the R foundation for statistical computing) was used to analyze the data.
The statistically significant level for all was set to 0.05.
RESULTS
Table 1 shows patient demographics. Forty one patients had 46 fractures ; 36 patients had a single-level fracture, 5 two-level fractures. Thoracolumbar junctions (T10, T11, T12, L1, L2) were involved in 36 fractures, lower thoracic vertebrae (T7, T8, T9) were involved in 3 fractures and lower lumbar vertebrae (L3, L4, L5) were involved in 7 fractures. Subjects, 6 men and 35
women, were of average age 67.2 years (range, 56~
88) and average period until the last radiographic measurement was 8.3 months (range, 3~24). During follow-up, 3 patients underwent surgery ; two patients with delayed post-traumatic vertebral collapse at 6 months later and one patients with infective spondylitis at the fracture level at 3 months later.
For all 46 fractures average VBB ratio was 49.1%
(range, 11.7~91.0) and average ΔAWA was 7.1o (range, 1.2~16.0). VBB ratio showed a significant correlation with ΔAWA (P<0.001, cc=0.660) (Fig. 3).
No difference of ΔAWAs was found between men and women (P=0.317). Age, initial AWA, and EP score showed no significant correlation with ΔAWA (P=
0.629, P=0.724, P=0.690, respectively, not shown in the figure). There was also no correlation between T-score and ΔAWA, between T-score and VBB ratio (P= 0.548, P=0.370, respectively) (Fig. 4).
During follow-up, 5 patients with 5 fractures were diagnosed as delayed post-traumatic vertebral collapse.
These patients were all old women. Details were shown in Table 2. The average T-score was -3.4 which was not significantly different from that of whom didn’t have delayed post-traumatic vertebral collapse (P=
0.873). The average VBB ratio and ΔAWA was 71.2%
and 13.5o which was significantly greater than that of whom didn’t have delayed post-traumatic vertebral collapse (P=0.015, P<0.001, respectively). Further
Fig. 4. Graphs showing (a) no correlation between T-score and ΔAWAand (b) no correlation between T-score and VBB ratio.
Table 2. Data of the patients diagnosed as delayed post-traumatic vertebral collapse No. Sex Age Level (Type) Time to develop
(months) T-score VBB ratio (%) ΔAWA (o) Opeartion
1 F 61 L1 (A3.1) 6 -5.0 70.0 15.1 Yes
2 F 72 T12 (A3.3) 6 -2.5 94.5 14.0 Yes
3 F 72 L1 (A3.1) 3 -4.3 61.3 13.5 No
4 F 74 L1 (A1.2) 8 -2.8 55.4 13.9 No
5 F 88 L1 (A1.1) 3 -2.6 74.6 11.0 No
Average - 73.4 - 5.2 -3.4 71.2 13.5 -
Table 3. Comparison of the occurrence rate of delayed post-traumatic vertebral collapse according to VBB ratio*
2 groups according to VBB ratio P
<20% vs >20% 1.000
<40% vs >40% 0.632
<60% vs >60% 0.037
<80% vs >80% 0.274
* Analyzed using Fisher’s exact test with minimum P- value approach
Analysis was done by dividing VBB ratio into several sections. In the fractures with VBB ratio more than 60%, delayed post-traumatic vertebral collapse developed significantly more than in those with less than 60%
(P=0.037) (Table 3). In other words, of 32 levels with VBB ratio less than 60%, one delayed post-traumatic vertebral collapse developed (3.1%). On the other hand, of 14 levels with VBB ratio more than 60%, 4 delayed post-traumatic vertebral collapses developed (28.6%).
Of these 5 patients with delayed post-traumatic verte- bral collapse, two were treated operatively. One had two level fracture of T12 and L1 followed by delayed post-traumatic vertebral collapse of L1. She had suffered from persistent pain without neurologic deficit.
Because she had taken medication including warfarin, surgery could not be performed, and thus, verte- broplasty at T12, L1 was performed at 6 months after injury. The other patient with a T12 single level fracture who had progressvie kyphosis and neurologic deficit underwent anterior reconstruction and posterior instrumentation at 6 months after injury. The other three patients with delayed post-traumatic vertebral collapse were asymptomatic without neurologic deficit and had a severe medical comorbidity, and thus, were not considered to be treated operatively.
DISCUSSION
Bone bruise has been well investigated in MRI A
B
studies of the knee and ankle.7,14 Its outcomes are generally good both radiologically and clinically if no other articular structures have been injured.6 In case of acute thoracolumbar vertebral fractures, VBB is also observed in the majority at the injured vertebrae.
Contrary to the knee and ankle, gradual subsequent collapse usually occurs after the vertebral fracture, although it is sometimes minimal. It has been reported that kyphosis had increased by a mean of 3o to 8o after nonoperative treatment in patients with a burst fracture.15-17 Willen et al. reported that kyphosis increased by a mean of 8˚ during the first 6 months after fracture, and that no further progression occurred.15 Our results were comparable to these findings in that average ΔAWA was 7.1o and average period until the last radiographic measurement was 8.3 months.
The vertebral bodies have the peculiar anatomic and biomechanical features that are different from the bony structures around the knee. First, because vertebral bodies are composed of more cancellous bone and have thinner cortices than bones around the knee, they are vulnerable to deform after trauma.18 Second, thoraco- lumbar vertebral fractures usually occur in elderly people than knee injuries. As age increases, the bone quality of vertebral body tends to worsen, whereas the bony structures around knee become much harder due to degenerative changes and subsequent subchondral sclerosis.19 Third, VBB in vertebral fracture is located within the vertebral body that is under weight-bearing.
In injured knees, for example, in cases of ACL (anterior cruciate ligament) injury, bone bruise usually develops in the posterior aspect of the lateral tibial plateau and the anterior aspect of the lateral femoral condyle, which are not directly under weight-bearing.3 These differences probably explain why vertebral fractures gradually collapse over time whereas injuries of the knee do not.
Our hypothesis was proven through the current results that showed only VBB ratio was significantly correlated with ΔAWA (P=0.001, cc=0.660). There was
no difference of ΔAWA according to gender. Other parameters such as age, initial AWA, EP score showed no significant correlation with ΔAWA. Before starting the study we expected the BMD would affect the subsequent vertebral collapse. In present study, how- ever, the T-score had no correlation with ΔAWA.
Standard spine BMD, measured in the anteroposterior direction, includes mineral in the posterior elements and facet joint as well as the abdominal aorta, which may not contribute to the strength of the vertebral body.20 Moreover, spine BMD tends to increase after 65 years old by degenerative change of facet joint.21 Considering these facts, the BMD, especially in old age, might not fully reflect the trabecular microstructures of vertebral body itself.
The architecture of the vertebral body consists of highly porous trabecular bone and a fairly dense, solid shell. However, this shell is very thin throughout, on average only 0.4 mm,18 and is indistinguishable from the trabecular core but rather is a denser arrangement of treabecular elements. Finite element analysis esti- mated the contribution made by the shell to the overall load carrying capacity was less than 15%.22,23 In other words, vertebral bodies mainly depends on the well- organized trabecular structure to resist the vertical compressive load. VBB is an emanation of the micro- fracture at medullar trabeculae24,25, which disorganizes the trabecular architecture and reduces load sharing capacity. Accordingly, it can be assumed that VBB might indicate a loss of supporting structures and facilitate subsequent vertebral collapse.
In contrast to our results, Teli et al.12 suggested that VBB within a thoracolumbar vertebral body in an adult patient did not cause significant vertebral wedging, and thus, concluded that VBB was not a risk factor for post-traumatic deformity. Their study was performed on accompanying occult vertebral injuries that showed just bone bruise without cortical disruption, whereas we placed a focus on fractured vertebrae. We are of the opinion that incidentally found VBB after occult verte-
bral injury replicates bone bruise after knee injury because both injuries usually occur with preservation of cortical continuity. We postulate that once cortical continuity is disrupted, VBB begins to play a role in subsequent vertebral collapse via destruction of suppor- ting trabecular structures.
Delayed post-traumatic vertebral collapse develops especially after osteoporotic vertebral fractures. Clini- cally, it is known to occur in approximately 10% of osteoporotic vertebral fractures mainly in the thoraco- lumbar zone. In the present study, 5 patients were diagnosed as having delayed post-traumatic vertebral collapse. Their average T-score was -3.4 which was not significantly different from that of the other DEXA group. Therefore, BMD per se does not seem to predispose delayed post-traumatic vertebral collapse.
Several studies had been conducted to determine the pathophysiology of delayed post-traumatic vertebral collapse. It has been known that delayed post-traumatic vertebral collapse results from a combination of ische- mia and pseudoarthrosis. Maldague et al. stated that vertebral collapse was associated with bone necrosis,26 and Lee et al. classified the MR appearance and correlated it with histologic findings.27 In the present study, average VBB ratio in those that experienced delayed post-traumatic vertebral collapse was 71.2%, which was significantly higher than the average (46.5%) for the other subjects (P=0.015). We found that the fractures with VBB over 60% were more likely to develop delayed post-traumatic vertebral collapse than those with under 60% (Table 3). We believe that the VBB ratio can be a radiographic risk factor of delayed post-traumatic vertebral collapse in osteoporotic thoracolumbar vertebral fractures, because we thought VBB could represent compromised intravertebral vascu- lature which is vulnerable to ischemia and resultant necrosis and nonunion. Yasuo et al.28 emphasized the importances of achieving an initial correct diagnosis and of immobilization after osteoporotic vertebral fractures for preventing the delayed collapse and
subsequent neurological deficits. We suggest that patients with a large-sized VBB should be followed up meticulously to early detect intravertebral vacuum or delayed post-traumatic vertebral collapse and should be treated strictly not to progress delayed collapse.
We acknowledge several limitation of the current study. Because MRI was taken mean 8.4 days after the initial trauma, the amount of bone bruise might change.
However, we took the plain radiographs and MRI at the same time, so we thought it was reasonable to compare the change in plain radiographs as to the MRI findings. The ways to measure VBB and its application to the change of AWA is a potential source of bias.
However, in this study we assumed that subsequent vertebral collapse would mainly occur in the similar plane where bone bruise was largest. We used the parameter of ΔAWA to represent the degree of subsequent vertebral collapse. ΔAWA is probably an imperfect surrogate to represent the degree of the vertebral collapse because there might be the somewhat different fracture pattern, although rare, that shows just cupping of the superior endplate or simultaneous collapse of the anterior and posterior cortex, and under these conditions anterior wedging can be minimal or absent. Nevertheless, this study does demonstrate a tendency toward subsequent vertebral collapse of fractured vertebrae with larger VBB. To overcome these limitations, CT study needs to be included.
Although we found no correlation between ΔAWA and age, T-score and EP score, we believe that other factors such as BMI and daily activity status might affect subsequent collapse.
Despite several limitations, this is the first study to measure VBB quantitatively and to determine its impact on subsequent vertebral collapse in osteoporotic verte- bral fractures. The study showed that VBB and sub- sequent vertebral collapse are significantly related.
Vertebral bone bruise after osteoporotic thoracolumbar vertebral fracture was significantly correlated with subsequent vertebral collapse (cc=0.660). We recom-
mended that patients with a large VBB, especially in case of >60%, should be followed up meticulously for the early detection of delayed post-traumatic vertebral collapse.
REFERENCES
1. Eustace S, Keogh C, Blake M, Ward RJ, Oder PD, Dimasi M. MR imaging of bone oedema: mecha- nisms and interpretation. Clin Radiol 2001;56:4-12.
2. Boks SS, Vroegindeweij D, Koes BW, Bernsen RM, Hunink MG, Bierma-Zeinstra SM. Clinical consequences of posttraumatic bone bruise in the knee. Am J Sports Med 2007;35:990-5.
3. Roemer FW, Bohndorf K. Long-term osseous sequelae after acute trauma of the knee joint evaluated by MRI. Skeletal Radiol 2002;31:615-23.
4. Rangger C, Kathrein A, Freund MC, Klestil T, Kreczy A. Bone bruise of the knee: histology and cryosections in 5 cases. Acta Orthop Scand 1998;
69:291-4.
5. Boks SS, Vroegindeweij D, Koes BW, Bernsen RM, Hunink MG, Bierma-Zeinstra SM. MRI follow-up of posttraumatic bone bruises of the knee in general practice. AJR Am J Roentgenol 2007;
189:556-62.
6. Wright RW, Phaneuf MA, Limbird TJ, Spindler KP. Clinical outcome of isolated subcortical trabecular fractures (bone bruise) detected on mag- netic resonance imaging in knees. Am J Sports Med 2000;28:663-7.
7. Miller MD, Osborne JR, Gordon WT, Hinkin DT, Brinker MR. The natural history of bone bruises. A prospective study of magnetic resonance imaging- detected trabecular microfractures in patients with isolated medial collateral ligament injuries. Am J Sports Med 1998;26:15-9.
8. Saifuddin A. MRI of acute spinal trauma. Skeletal Radiol 2001;30:237-46.
9. Oner FC, van Gils AP, Dhert WJ, Verbout AJ.
MRI findings of thoracolumbar spine fractures: a categorisation based on MRI examinations of 100 fractures. Skeletal Radiol 1999;28:433-43.
10. Saifuddin A, Noordeen H, Taylor BA, Bayley I.
The role of imaging in the diagnosis and manage- ment of thoracolumbar burst fractures: current concepts and a review of the literature. Skeletal Radiol 1996;25:603-13.
11. Oner FC, vd Rijt RH, Ramos LM, Groen GJ, Dhert WJ, Verbout AJ. Correlation of MR images of disc injuries with anatomic sections in experi- mental thoracolumbar spine fractures. Eur Spine J 1999;8:194-8.
12. Teli M, de Roeck N, Horwitz MD, Saifuddin A, Green R, Noordeen H. Radiographic outcome of vertebral bone bruise associated with fracture of the thoracic and lumbar spine in adults. Eur Spine J 2005;14:541-5.
13. Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S. A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 1994;3:
184-201.
14. Labovitz JM, Schweitzer ME. Occult osseous injuries after ankle sprains: incidence, location, pattern, and age. Foot Ankle Int 1998;19:661-7.
15. Willen J, Anderson J, Toomoka K, Singer K. The natural history of burst fractures at the thoraco- lumbar junction. J Spinal Disord 1990;3:39-46.
16. Reinhold M, Knop C, Lange U, Bastian L, Blauth M. [Non-operative treatment of thoracolumbar spinal fractures. Long-term clinical results over 16 years]. Unfallchirurg 2003;106:566-76.
17. Moller A, Hasserius R, Redlund-Johnell I, Ohlin A, Karlsson MK. Nonoperatively treated burst frac- tures of the thoracic and lumbar spine in adults: a 23- to 41-year follow-up. Spine J 2007;7:701-7.
18. Silva MJ, Wang C, Keaveny TM, Hayes WC.
Direct and computed tomography thickness measure- ments of the human, lumbar vertebral shell and endplate. Bone 1994;15:409-14.
19. Ferguson SJ, Steffen T. Biomechanics of the aging spine. Eur Spine J 2003;12 Suppl 2:S97-S103.
20. Cummings SR, Bates D, Black DM. Clinical use of bone densitometry: scientific review. JAMA 2002;
288:1889-97.
21. Steiger P, Cummings SR, Black DM, Spencer NE, Genant HK. Age-related decrements in bone mine- ral density in women over 65. J Bone Miner Res 1992;7:625-32.
22. McBroom RJ, Hayes WC, Edwards WT, Goldberg RP, White AA, 3rd. Prediction of vertebral body compressive fracture using quantitative computed tomography. J Bone Joint Surg Am 1985;67:1206- 14.
23. Silva MJ, Keaveny TM, Hayes WC. Load sharing between the shell and centrum in the lumbar vertebral body. Spine (Phila Pa 1976) 1997;22:
140-50.
24. Mink JH, Deutsch AL. Occult cartilage and bone injuries of the knee: detection, classification, and assessment with MR imaging. Radiology 1989;
170:823-9.
25. Yao L, Lee JK. Occult intraosseous fracture: detec- tion with MR imaging. Radiology 1988;167:749-51.
26. Maldague BE, Noel HM, Malghem JJ. The intra- vertebral vacuum cleft: a sign of ischemic vertebral collapse. Radiology 1978;129:23-9.
27. Lee CS, Yu JW, Chung SS, Suh YL, Ahn G, Ahn JM. Delayed Post-traumatic Vertebral Collapse:
MR Categorization and MR-Pathology Correlation.
Asian Spine J 2007;1:32-7.
28. Ito Y, Hasegawa Y, Toda K, Nakahara S. Patho- genesis and diagnosis of delayed vertebral collapse resulting from osteoporotic spinal fracture. Spine J 2002;2:101-6.