고령 고혈압 환자에서 천일염의 혈압 감소 효과: 예비 무작위 대조시험
백승하
1, 안주원
1, 이혜리
2, 조수현
1, 김정하
11중앙대학교 의과대학 중앙대학교병원 가정의학과, 2연세대학교 의과대학 강남세브란스병원 가정의학과
Anti-Hypertensive Effect of a Solar Salt Diet in Elderly Hypertensive Patients: A Preliminary Randomized, Double-Blind Clinical Trial
Seung Ha Baek
1, Ju Won Ahn
1, Hye-Ree Lee
2, Soo Hyun Cho
1, Jung-Ha Kim
11
Department of Family Medicine, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea
2
Department of Family Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
Background: High sodium and/or low mineral intake are known to be associated with elevated blood pressure.
It has been reported that substituting low-sodium, mineral-rich salt for refined salt lowers blood pressure (BP).
And solar salt is emerging as a low sodium high mineral salt for a healthy diet in Korea. Therefore, this dou- ble-blind, randomized, and placebo-controlled trial was conducted to explore changes in BP from substituting refined salt with solar salt among hypertensive elderly subjects.
Methods: Forty-three hypertensive and institutionalized elderly individuals aged 65 years or older were enrolled. Thirty-eight subjects (88.4%) completed the study. Subjects were provided with either a solar salt- or refined salt-based diet for eight weeks.
Results: Systolic BP decreased significantly in the solar salt-based diet group after 2, 4, and 8 weeks when compared to the refined salt-based diet group. And, diastolic BP was lowered significantly in the solar salt-based diet group compared to that in the refined salt-based diet group after 8 weeks. In addition, urinary sodium/po- tassium, and angiotension converting enzyme activity decreased significantly in the solar salt-based diet group compared to the refined salt-based group. Urinary potassium excretion was significantly increased in the solar salt-based diet group.
Conclusions: These results may provide clinical evidence that solar salt has beneficial effects on BP in elderly patients. And, people such as Koreans, who do not consume enough minerals, may experience a greater an- ti-hypotensive effect by using solar salt. However, further large-scale studies are necessary.
Korean J Health Promot 2015;15(3):98-107
Keywords: Hypertension, Blood pressure, Aged, Salt, Randomized controlled trial
■ Received:March 9, 2015 ■ Accepted:July 7, 2015
■ Corresponding author:Jung-Ha Kim, MD, PhD
Department of Family Medicine, Chung-Ang University Hospital, Chung-Ang University College of Medicine, 102 Heukseok-ro, Dongjak-gu, Seoul 06973, Korea
Tel: +82-2-1800-1114, Fax: +82-2-6264-8272 E-mail: [email protected]
■Financial support was provided by the Ministry of Knowledge and Economy through a regional technology innovation program.
INTRODUCTION
Hypertension is more prevalent, less controlled, and more severe in the elderly, affecting more than two out of every three individuals over the age of 75.
1)Although many eld- erly hypertensive patients use anti-hypertensive medications, it is necessary to consider all medical conditions and history before prescribing anti-hypertensive medications as adverse effects can occur frequently. In addition, there has been an increasing tendency not to treat high blood pressure with anti-hypertensive medications in the elderly.
2)Instead, mod- ifications in lifestyle, such as reduced sodium intake, are more importantly suggested as a first approach.
High sodium intake is associated with elevated blood pressure (BP) and increased risk of cardiovascular disease (CVD).
3)And, it has been shown that a high salt intake is an independent factor in predicting the risk of type 2 diabetes.
4)There have been many animal experiments, epi- demiological studies, and clinical trials concluding that hy- pertension and CVD can be prevented by decreasing dietary sodium.
5,6)It has also been reported that dietary minerals have a beneficial effect on blood pressure, especially in hy- pertensive patients.
7)However, the hypotensive effect of each mineral supplementation is not consistent.
7)Increasing the intake of a variety of minerals is more effective in low- ering BP than a single mineral.
7)Furthermore, the anti-hy- pertensive effect of the Dietary Approaches to Stop Hypertension diet, which includes numerous minerals such as potassium, calcium, and magnesium, was much greater than reduced sodium intake.
8)Therefore, the replacement of refined salt with low-sodium, mineral-rich salt has been suggested as an effective alternative to reducing salt and in- creasing minerals in the diet. Studies have shown that sub- stituting mineral-rich salt for refined salt lowered BP in subjects with hypertension.
9-12)Solar salt is produced from the evaporation and concen- tration of seawater. It contains a smaller percentage of NaCl (85.03%) than regular refined table salt (99.05%).
And, solar salt contains abundant minerals, including cal- cium (1,495 ppm), potassium (2,494 ppm), and magnesium (8,190 ppm).
13)Solar salt, as a low sodium-high mineral salt, in the diet may be useful in controlling high BP in elderly hypertensive patients. To date, no clinical study has been conducted comparing the effects of consuming solar salt and refined salt.
The purpose of this study was to explore the blood pressure lowering effect of a solar salt diet in hypertensive elderly subjects compared to those on a refined salt diet.
METHODS
1. Study subjects
Subjects were inpatients recruited from the department of family medicine and physical medicine & rehabilitation at a nursing hospital for the elderly from October 2009 to February 2010. Study procedures were explained to partic- ipants and their guardians. Eligible subjects were aged 65 years or older and had been diagnosed with hypertension.
Hypertension was defined as systolic BP ≥140 mmHg/dia- stolic BP ≥90 mmHg.
14)or the use of anti-hypertensive medication. Subjects were excluded if they had one or more of the following: 1) malignant cancer; 2) life expectancy less than six months; 3) Global Deterioration Scale (GDS) stage 7/bed-ridden status; 4) acute exacerbation of chronic disorders; 5) renal dysfunction (high than normal range of serum creatinine); 6) unable to ingest solid food; or 7) change of anti-hypertensive medication within 4 weeks pri- or to screening. A total of 43 elderly patients with hyper- tension hospitalized with chronic diseases volunteered for the study. Among 140 hospitalized patients, 12 patients without hypertension patients, 8 cancer patients, 10 pa- tients with late dementia (GDS 7) or a bed-ridden status, 26 patients with unstable conditions due to acute ex- acerbation of chronic disease or an acute illness (such as urinary tract infection), 5 patients with abnormal renal function, 4 patients with change to their anti-hypertensive medications within 4 weeks prior to screening, and 32 pa- tients in for short-term admission, scheduled for discharge within 2 weeks, or not admitted at least 4 weeks prior to screening were excluded. This study was conducted ac- cording to the Declaration of Helsinki and the study pro- tocol was approved by the Institutional Review Board of the Chung-ang University Hospital. Written informed con- sent was obtained from every participant and guardian.
2. Study design
A randomized, double-blind clinical trial was carried out
for eight weeks to compare the effects of solar and refined
Figure 1. Flowchart of the study design and study subjects. BP, blood pressure.
Enrollment: 43 subjects
- Anthropometry - Biochemical assay - Nutritional analysis
- Cognitive and functional assessment 1 wk
Randomization
Common refined salt group
(n=22) 8 wk Solar salt group
(n=21) -BP measurement
- Nutritional analysis
Withdrawal : 2 subject - Unexpected discharge: 1 - Condition deterioration: 1
Withdrawal: 3 subjects - Unexpected discharge: 2 - Condition deterioration: 1
- Anthropometry -Biochemical assay -Nutritional analysis 20 completed
8-week diet 18 completed
8-week diet
salts on blood pressure in patients with hypertension (Fig.
1). Assuming a significant level (α)=0.05 and a one-sided test, the intended sample of 36 recruited subjects provided a power of 80%. In our study, the primary outcome meas- ure was systolic BP at week 8. In a previous study,
13)sys- tolic BPs at 8 weeks in the control group and mineral salt group were 161.0±2.1 and 151.8±2.1 mmHg, respectively.
We wanted the capability to show a difference of 2 mmHg in systolic BP between the groups. The drop-out rate was expected to be less than 15% and we asked 43 patients to participate in this study.
Among the subjects, two subjects in the solar salt group and one from the refined salt group were excluded from the study due to unexpected discharge from the hospital;
and two other subjects, one from each group, were excluded because of deteriorating conditions. Thirty-eight subjects completed the study, for a completion rate of 88.4%.
Study subjects were randomized in a double-blind fash- ion to receive either a solar salt- or a refined salt-based diet. Randomization was performed by creating a table of random numbers, which assigned each subject into either group. The investigator and subjects were unaware of the type of salt contained in the meals. Subjects were provided with a meal composed of 2,000 kcal/day for males and 1,600 kcal/day for females according to the Dietary Reference
Intakes for Koreans (KDRIs).
15)For both groups, 5,000 mg/day of sodium was provided based on the average Korean consumption,
16)as a sudden application of the KDRI (goal:
2,000 mg/day) resulted in a decrease in dietary intake due to significant changes in palatability to the subjects. Each meal was prepared by adding 2.4 g refined salt (sodium 1,000 mg) or 2.8 g solar salt (sodium 1,000 mg) to a low-salt diet (sodium 2,000 mg/day). Subjects and care workers were educated on the restrictions of extra snacks. The solar salt- based diet group was provided meals using seasoning, soy- bean paste, and kimchi (Korean-style fermented vegetables) made from solar salt (Shinan, Jeollanam-do, Korea). Subjects were evaluated after eight weeks, while continuing their anti-hypertensive therapy.
3. Measurements
Anthropometric evaluation, nutritional analysis, and bio-
chemical assays were performed for each patient. Medical
history, current medical conditions, and medication data
were collected from medical records. For cognitive and
functional assessment at baseline, valid and reliable instru-
ments including Korean Mini-Mental State Examination
(K-MMSE),
17)Korean Activities of Daily Living (K-ADL),
18)Seoul-Instrumental Activities of Daily Living (S-IADL),
19)and GDS
20)were performed. MMSE is a brief 30-point ques- tionnaire test that is used for screening cognitive impairment.
Scores of 24 and higher indicate normal cognition. Scores of less than 19 suggest dementia.
17)ADL and IADL are func- tional assessment tools, particularly in regards to people with disabilities and the elderly. ADL and IADL consist of 7 items (points range: 0-14) and 15 items (points range:
0-45), repectively.
18,19)Higher scores imply low functional status. GDS is a useful tool for staging dementia (1-7).
20)Stages 5, 6, and 7 suggest early dementia (moderately se- vere cognitive decline), middle phase of dementia (severe cognitive decline), and late dementia (very severe cognitive decline), respectively.
20)Body weight was measured to the nearest 0.1 kg using an electronic scale, and height was measured to the nearest 0.1 cm using a stadiometer. Body mass index (BMI) was calculated as weight/height
2(kg/m
2). Blood pressure was measured to the nearest 1 mmHg using a mercurial sphyg- momanometer via the auscultatory method twice a day (8 a.m. and 8 p.m.) and was calculated as an average value.
Dietary intake of subjects was evaluated twice a week (Tuesdays and Saturdays) by directly weighing the foods consumed by individuals by a trained dietitian. Dietary da- ta were collected from a week before randomization to the end of the trial. With this information, energy and nutrient intake were analyzed using the CAN-Pro 3.0 program (The Korean Nutrition Society, Seoul, Korea) developed by the Korean Nutrition Society.
Biochemical tests were performed on blood samples col- lected after overnight fasting (>8 hours). Serum levels of fasting glucose, total cholesterol, high density lipoprotein (HDL)-cholesterol, and triglyceride were measured using an ADVIA 1650 Chemistry system (Siemens, Tarrytown, NY, USA). Blood urea nitrogen, creatinine, and serum and urine electrolytes including sodium, potassium and chlor- ide, were measured by an ADVIA 1650 Chemistry system (Siemens). Fasting insulin levels were measured via an elec- trochemiluminescence immunoassay (Roche, Indianapolis, IN, USA), and insulin resistance was estimated according to the homeostasis model assessment of insulin resistance (HOMA-IR) index [(insulin (μlU/mL) ×fasting blood glu- cose (mg/dL)/18)/22.5]. Angiotensin converting enzyme (ACE) levels were measured using an enzyme- linked immunosorbent assay (R&D Systems, Minneapolis, MN, USA), and the in- ter- and intra-assay variabilities were 5.9±1.6 and 3.7±0.3%,
respectively.
4. Statistical analyses
Data are presented as median (25-75%). Baseline charac- teristics in subjects were compared using Wilcoxon rank sum test for continuous variables and the Chi-square test or Fisher’s exact test for categorical variables in cells with an expected count less than 5. Changes in systolic and dia- stolic BPs, and other clinical parameters were calculated using the Wilcoxon rank sum test or the Wilcoxon signed rank test between groups or within each group according to the randomization. And, the Kolmogorov-Smirnov nor- mality test on the ACE values was performed. To examine the change of ACE levels between groups, ANCOVA (Analysis of Covariance) was used. Significance was defined at the 0.05 level of confidence. All calculations were per- formed using the SAS 9.1 statistics package (SAS Institute Inc., Cary, NC, USA).
RESULTS
1. Clinical characteristics of the subjects at baseline
The clinical characteristics of subjects according to solar or refined salt-based diets are shown in Table 1. No stat- istical differences were seen in age, BMI, gender, BP and pulse rate, cognitive and functional assessment, or medical history between the groups. Twenty-seven patients (71.05%) were currently using one or more anti-hypertensive medi- cations. Four patients in each group have taken an anti-hy- pertensive medication (solar-salt group: 1 diuretic, 2 calcium channel blocker (CCB), and 1 ACE inhibitor or angio- tensin receptor blocker (ARB); refined salt group:1 diu- retic, 3 CCB). Users (P=0.980) and types (P=0.450) in blood pressure-lowering agents were not different between the groups. There were no significant differences in the levels of fasting glucose (P=0.130) and insulin (P=0.600); HOMA-IR (P=0.860); total cholesterol (P=0.750); triglyceride (P=0.480);
HDL-cholesterol (P=0.360); low density lioprotein-choles- terol (P=0.540); blood urea nitrogen (P=0.970) and creatinine (P=0.120); serum sodium (P=0.200), potassium (P=0.160), and chloride (P=0.450); or urinary sodium (P=0.770), potassium (P=0.970), and chloride (P=0.690) between the two groups.
Also, angiotensin converting enzyme activity (solar salt group:
Table 1. Clinical characteristics of the subjects at baseline
Solar salt (n=18) Refined salt (n=20) Pa
Age, y 79.5 (75-88)b 80.0 (77-84)b 0.520
Body mass index, kg/m2 24.4 (19.9-25.8)b 23.8 (19.2-25.3)b 0.270
Sex 0.170
Male 9 (64.29)c 5 (25.00)c
Female 9 (36.00)c 15 (75.00)c
Blood pressure, mmHg
Systolic 127.5 (121-140)b 129.0 (122-136)b 0.300
Diastolic 74.0 (70-94)b 76.0 (70-88)b 0.610
Pulse rate, beat/min 75 (70-82)b 72 (69-78)b 0.250
Geriatric functional assessment, score
MMSE-K 21 (13-23)b 20 (12-23)b 0.380
K-ADL 4.0 (2-7)b 4.0 (1-8)b 0.610
S-IADL 29.5 (20.0-38)b 32 (30-38)b 0.470
GDS 4.0 (3-5)b 5.0 (4-5)b 0.440
Antihypertensive medication 13 (72.2)c 14 (66.6)c 0.980
Diuretics 2 (15.38)c 1 (7.14)c
Calcium channel blockers 12 (92.31)c 13 (92.86)c
ACE inhibitors or ARBs 8 (61.54)c 6 (42.86)c
Beta-blockers 2 (15.38)c 3 (21.43)c
Medical history
Cardiovascular diseased 8 (44.44)c 9 (42.86)c 0.990
Diabetes mellitus 8 (44.44)c 6 (28.57)c 0.760
Dyslipidemia 2 (11.11)c 1 (4.76)c 0.590
Dementia 6 (33.33)c 7 (33.33)c 1.000
Osteoporosis 3 (16.67)c 7 (33.33)c 0.290
Abbreviations: MMSE-K, mini-mental state examination-Korean version; K-ADL, Korean activities of daily living; S-IADL, Seoul- in- strumental activities of daily living; GDS, global deterioration scale; ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker.
aCalculated using a Wilcoxon rank sum test, Fisher’s exact test or χ2 -test.
bMedian (25-75%).
cNumber (%).
dCerebral infarction, cerebral hemorrhage, myocardial infarction, angina or atherosclerosis.
Table 2. Changes in nutrient intake by the weighing method after 8 weeks
Solar salt (n=18) Pa Refined salt (n=20) Pa
Pre (baseline) Post (8 wk) Pre (baseline) Post (8 wk)
Calorie intake, kcal 1,299.06
(1,142.71-1,729.12)b 1,324.52
(1,011.63-1,732.43)b 0.770 1,271.91
(1,044.55-1,503.03)b 1,355.25
(1,178.77-1,475.32)b 0.120 Protein, % energy 16.61 (15.27-18.87)b 16.48 (14.53-17.78)b 0.770 17.94 (16.24-19.70)b 17.01 (16.15-17.62)b 0.160 Fat, % energy 19.92 (15.20-22.37)b 20.87 (14.97-23.08)b 0.090 20.60 (19.41-23.85)b 22.00 (18.87-23.03)b 0.930 Carbohydrate, % energy 63.14 (58.72-69.44)b 62.65 (58.81-70.36)b 0.640 62.30 (55.77-63.82)b 60.97 (58.90-64.98)b 0.650
aCalculated using a Wilcoxon signed rank test.
bMedian (25-75%).
107.3±33.98 ng/mL, refined salt group: 100.19±45.44 ng/mL;
P=0.300) was not different (Table 1).
2. Nutrient status before and after trial
Total calorie and nutrient intake before and after the tri- al are described in Table 2. There were no significant dif- ferences in baseline nutrient intake between the groups.
Intake of total calorie, protein, fat, and carbohydrate did not differ with change to the type of salt (Table 2).
3. Clinical outcomes of solar- or refined salt-based diet before and after 8 weeks
Pre- and post-study data are presented in Table 3. There
were significant decreases in systolic BP (P=0.007) and uri-
nary sodium/potassium (P=0.040) within the solar salt group
after trial. And, serum (P=0.030) and urinary (P=0.008) po-
tassium levels were increased within the solar salt group af-
ter the trial. In the refined salt group, no significant differ-
ences were found after the trial.
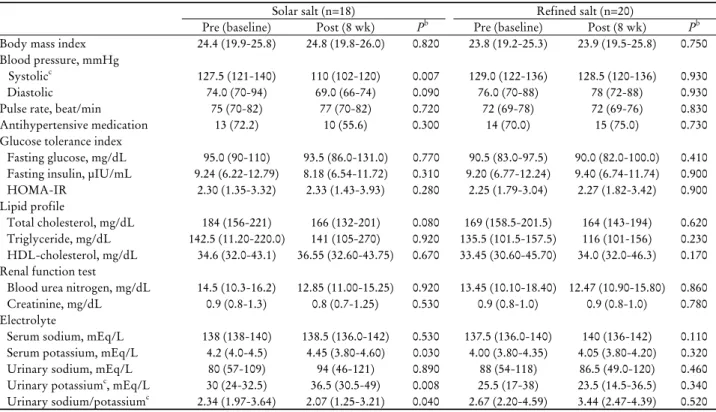
Table 3. Changes in study outcomes of solar- or refined salt-based diet after 8 weeks
aSolar salt (n=18) Refined salt (n=20)
Pre (baseline) Post (8 wk) Pb Pre (baseline) Post (8 wk) Pb
Body mass index 24.4 (19.9-25.8) 24.8 (19.8-26.0) 0.820 23.8 (19.2-25.3) 23.9 (19.5-25.8) 0.750 Blood pressure, mmHg
Systolicc 127.5 (121-140) 110 (102-120) 0.007 129.0 (122-136) 128.5 (120-136) 0.930
Diastolic 74.0 (70-94) 69.0 (66-74) 0.090 76.0 (70-88) 78 (72-88) 0.930
Pulse rate, beat/min 75 (70-82) 77 (70-82) 0.720 72 (69-78) 72 (69-76) 0.830
Antihypertensive medication 13 (72.2) 10 (55.6) 0.300 14 (70.0) 15 (75.0) 0.730
Glucose tolerance index
Fasting glucose, mg/dL 95.0 (90-110) 93.5 (86.0-131.0) 0.770 90.5 (83.0-97.5) 90.0 (82.0-100.0) 0.410 Fasting insulin, μIU/mL 9.24 (6.22-12.79) 8.18 (6.54-11.72) 0.310 9.20 (6.77-12.24) 9.40 (6.74-11.74) 0.900
HOMA-IR 2.30 (1.35-3.32) 2.33 (1.43-3.93) 0.280 2.25 (1.79-3.04) 2.27 (1.82-3.42) 0.900
Lipid profile
Total cholesterol, mg/dL 184 (156-221) 166 (132-201) 0.080 169 (158.5-201.5) 164 (143-194) 0.620 Triglyceride, mg/dL 142.5 (11.20-220.0) 141 (105-270) 0.920 135.5 (101.5-157.5) 116 (101-156) 0.230 HDL-cholesterol, mg/dL 34.6 (32.0-43.1) 36.55 (32.60-43.75) 0.670 33.45 (30.60-45.70) 34.0 (32.0-46.3) 0.170 Renal function test
Blood urea nitrogen, mg/dL 14.5 (10.3-16.2) 12.85 (11.00-15.25) 0.920 13.45 (10.10-18.40) 12.47 (10.90-15.80) 0.860
Creatinine, mg/dL 0.9 (0.8-1.3) 0.8 (0.7-1.25) 0.530 0.9 (0.8-1.0) 0.9 (0.8-1.0) 0.780
Electrolyte
Serum sodium, mEq/L 138 (138-140) 138.5 (136.0-142) 0.530 137.5 (136.0-140) 140 (136-142) 0.110 Serum potassium, mEq/L 4.2 (4.0-4.5) 4.45 (3.80-4.60) 0.030 4.00 (3.80-4.35) 4.05 (3.80-4.20) 0.320
Urinary sodium, mEq/L 80 (57-109) 94 (46-121) 0.890 88 (54-118) 86.5 (49.0-120) 0.460
Urinary potassiumc, mEq/L 30 (24-32.5) 36.5 (30.5-49) 0.008 25.5 (17-38) 23.5 (14.5-36.5) 0.340 Urinary sodium/potassiumc 2.34 (1.97-3.64) 2.07 (1.25-3.21) 0.040 2.67 (2.20-4.59) 3.44 (2.47-4.39) 0.520 Abbreviations: HOMA-IR, homeostasis model assessment of insulin resistance; HDL, high density lipoprotein.
aValues are presented as median (25-75%) or N (%).
bCalculated using a Wilcoxon signed rank test or χ2-test within each group.
cStatistical significance at P<0.05 according to a Wilcoxon rank sum test for comparing % change between two groups.
There were significant differences in the to systolic BP (solar salt: -15.38% [-16.67~-8.33], refined salt: 0%
[-7.69~15.38], P=0.040), urinary potassium excretion (solar salt: 5.27% [2.74-16.63], refined salt: -1.15% [-11.25~2.56], P=0.010), and urinary sodium/potassium (solar salt: -18.03%
[-31.38~-2.00], refined salt: 2.92% [-1.23~5.23], P=0.003).
The systolic BP decreased significantly after 2, 4, and 8 weeks within the solar salt-based diet group (all P<0.050), and was also significantly different after 2, 4, and 8 weeks between the two groups (all P<0.050, Fig. 2A). Changes in the diastolic BP were not observed after 2, 4, and 8 weeks within either group, but significant differences were ob- served between the two groups after 8 weeks (P=0.045, Fig. 2A). ACE activity decreased significantly in the solar salt-based diet (P=0.030, Fig. 2B) compared to the refined salt-based diet group after adjusting for age and sex.
After adjusting for total calories and urinary sodium us- ing ANCOVA for differences by calorie intake, we as- sessed the changes to the BP in the two groups. There were significant differences in systolic BP (P=0.020) and the rate of change of the systolic BP (P=0.040) in the solar salt group
compared to the refined salt group. Systolic BP (least square mean [standard error]) decreased by 14.12 (4.92) mmHg in the solar salt group and 1.48 (5.34) mmHg in the refined salt group, and the rate of change to systolic BP was -10.85 (3.77)% in the solar salt group and 0.14 (4.10)% in the re- fined salt group (data is not shown).
Also, in the case of including drop-out patients for the analysis of intention to treat, systolic BP for the solar salt group (n=21) was 130 (121-140) mmHg in the pre-study and 114 (110-132) mmHg in the post-study (P=0.010), and that of the refined salt group (n=22) was 129 (122-138) mmHg in pre- study and 129 (120-138) mmHg in post-study (P=0.910). Also, the rate of change of the systolic BP was significantly different between the two groups (P=0.009) (data is not shown) (Table 3).
DISCUSSION
The results of this study indicate that a solar salt-based
diet had beneficial effects on blood pressure in institutionali-
zed, elderly patients with hypertension. In addition, urinary
Figure 2. (A) Changes in systolic and diastolic blood pressures with intake of solar or refined salt over eight weeks. P-values were calculated using Wilcoxon rank sum test and Wilcoxon signed rank test. (B) The rate of change in ACE activity with intake of solar (least square mean [SE]: -15.45 [16.13]) or refined salt (least square mean [SE]: 34.09 [14.82]) before and after the study. P-values were calculated using ANCOVA. ACE, angiotensin converting enzyme; SE, standard error.
A B
sodium/potassium and ACE activity decreased significantly in the solar salt-based diet group compared to the refined salt-based group; and the urinary potassium excretion in- creased significantly in the solar salt-based diet.
In some previous studies,
9-12)a fall in systolic BP of 5-10 mmHg was reported by replacing refined salt with low so- dium, high potassium, high magnesium mineral salt in sub- jects with treated or untreated mild to moderate hyper- tension (above the mean systolic BP of 150 mmHg at base- line). Our solar salt study result is consistent with these previous studies, although each study had different mineral content of salt substitutes, characteristics of subjects, and intervention period. And, the hypotensive effect of solar salt in this trial was not inferior to the previous studies.
Subjects in this study were hospitalized patients. Therefore, their BP was relatively well-controlled with medication (baseline systolic blood pressure/diastolic blood pressure 128.5/76 mmHg). Nevertheless, we could still identify the hypotensive effect of mineral salt. In addition, our results suggest the possibility of a preventive effect by replacing
refined salt with solar salt for pre-hypertension individuals (systolic BP at 120-139 mmHg or a diastolic BP at 80-89 mmHg).
In particular, the elevation of the systolic BP is a result of the loss of arterial elasticity, or compliance, and is a characteristic of the elderly.
21,22)Systolic BP is a better in- dicator of increased cardiovascular risk in the elderly and is more reliable than diastolic BP alone.
23)Thus, the re- markable decrease in the systolic BP in the solar salt-based diet group is strong evidence for switching to a solar salt-based diet to prevent or manage cardiovascular diseases in the elderly.
Although there was no statistical significance, three sub- jects (1 diuretic user [hydrochlorothiazide 12.5 mg] and 2 CCB users [amlodipine maleate 5 mg]) did not need an- ti-hypertensive medication while on the solar salt-based diet.
Anti-hypertensive medications were also reduced from the
combination therapy of CCB (amlodipine maleate 5 mg)
and ARB (losartan 50 mg) to CCB mono-therapy in one
patient on the solar salt diet. These effects of consuming
solar salt may be more important in elderly hypertensive patients.
Urinary potassium excretion and sodium/potassium changed in the solar salt group. Minerals such as potassium, calcium, magnesium, and sodium in the body have a reciprocal rela- tion. Possible explanations for the association of these min- erals, contrary to sodium, with hypotensive effects have been suggested by experimental studies. First, potassium supple- ment increased sodium excretion in high sodium intake Dahl salt-sensitive rats.
24)Second, these minerals can directly in- fluence vascular relaxation and dilatation by changing the cell membrane potential in the vascular smooth muscle and endothelial cells
25-27)and by increasing nitric oxide pro- duction in the endothelium.
24)Third, modulation of the re- nin-angiotensin-aldosterone system (RAAS), a hormone sys- tem regulating blood pressure and fluid balance, can be in- volved in the hypotensive effect via these minerals directly or indirectly. Changes in calcium and magnesium fluxes across cell membranes are reflected in plasma rennin activ- ity in hypertension.
28,29)Extracellular ionized calcium inhibits rennin secretion through the calcium- sensing receptors lo- calized in the juxtaglomerular apparatus.
30)Blood pressure in the solar salt-based diet group did not increase as much as that in the refined salt-based diet group of Dahl salt-sen- sitive rats.
31)Plasma ACE activity in the solar salt-based diet group was also lower than that in the refined salt-based diet group.
32)Finally, possible mechanism offered by some previous researches is the anti-oxidative effect of the min- eral abundant solar salt. It is also known that sodium en- hances oxidative stress.
32)However, production of peroxides was lower with solar salt than with regular refined salt.
33)The antioxidative effects of Cheonggukjang, soybeans nat- urally fermented by Bacillus subtilis, made using solar salt were higher than that made using regular refined salt.
34)Furthermore, solar salt fed mice showed higher suppression of tumor growth, increases in natural killer cell activity, and inhibition of lipid peroxidation than regular refined salt fed mice in the Sarcoma-180 cell transplanted mice.
35)Although the mechanism by which solar salt-based diet modulates vascular tone is not fully understood, decrease in sodium retention, vasodilation and improvement of endothelial func- tion, modulation of RAAS, and the anti-oxidative effect may be important factors.
According to the Korea National Health and Nutrition Examination Survey, there is an inadequate intake of cal-
cium and potassium. Calcium intake was 66% of the Rec- ommended Nutrient Intake (RNI) and potassium was 78%
of the RNI in females older than 1 year old.
36)Therefore, substituting low-sodium and abundant mineral solar salt for refined salt may have a greater anti-hypotensive effect in Koreans.
ACE activity was reduced in the solar salt group. How- ever, unexpectedly, increased ACE activity in the refined salt group was much greater than the decreased ACE activ- ity in the solar salt group. Increased ACE expression is well-known to be related to a higher risk of cardiovascular disease development and progression.
37)ACE inhibitors are widely used to reduce blood pressure and prevent renal complication.
38)But the mechanisms that regulate ACE ex- pression are still unclear.
39)The reason for the increased ACE activity in the refined salt group is difficult to ex- plain properly. We cannot exclude the possibility of the in- fluence of other factors than salt.
This study has some limitations including its small sam-
ple size. The design was non-community-based and, along
with this, there is a potential for selection bias. Due to the
small number of subjects, it was difficult to assess other ben-
eficial effects or mechanisms besides the anti-hypertensive
effects of solar salt intake. However, because salt-based
foods, including such dishes as Kimchi and other salt-fer-
mented fish products, are very diverse among the foods
consumed regularly by Koreans, we had to conduct a trial
with a small number of subjects for dietary control. In or-
der to not alter individual salt taste preferences, we had to
provide equivalent sodium content to both groups. This
study supports the beneficial effects of solar salt intake, in-
cluding sodium reduction. And, in a nutrient database used
for this study, solar salt is not included. We could not
evaluate properly the mineral intake of the solar salt-based
diet group. Thus, measuring urinary sodium and potassium
excretion was the only option. Also, we cannot clarify the
effect of refined salt in type and dose of antihypertensive
medication. In conclusion, our results may provide clinical
evidence that solar salt is beneficial for lowering or main-
taining a healthy blood pressure. However, further large-scale
studies and trials considering variable antihypertensive medi-
cation are necessary to investigate the other potential bene-
fits of solar salt intake in elderly patients with hypertension.
ACKNOWLEDGEMENTS
The authors would like to thank In-Cheol Kim, Ph.D.
and Hag-Lyeol Kim, Ph.D. for providing solar salt and products such as soybean paste and kimchi made from so- lar salt. The authors are grateful to Jee-Aee Im, Ph.D. at INTOTO Inc. for performing laboratory analyses and to Sung-Jun Park, M.D. at Lohas-clover Hospital for clinical trial.
요 약
연구배경: 나트륨 과다 섭취와 적은 미네랄 섭취는 혈압
상승과 연관된 것으로 알려져 있으며 , 정제 소금을 저염도,
고미네랄 천일염으로 대체하는 것은 혈압을 낮춘다고 보 고되고 있다. 천일염은 한국에서 건강한 식습관을 위한 저 염도, 고미네랄 소금으로 부상되고 있다. 따라서 정제 소금 을 천일염으로 대체한 고령 고혈압 환자의 혈압 변화에 대 하여 연구하기 위하여 무작위 이중 맹검 위약 대조시험을 시행하였다.
방법: 43명의 65세 이상 노령 고혈압 환자가 이 실험에 최초 등록되었고 , 이 중 38명(88.4%)이 시험을 완료했다. 연 구 대상은 실험군으로 천일염 그리고 대조군으로 정제염을 섭취하는 식생활을 8주 동안 진행하였다.
결과: 천일염을 섭취하는 집단은 정제염을 섭취하는 대조 집단과 비교하였을 때 수축기 혈압이 2, 4, 8주 후에 크게 감소하였고, 확장기 혈압 또한 8주 후에 크게 떨어졌다. 또 한 천일염을 섭취하는 집단에서는 소변 중 나트륨/칼륨과 ACE 활동이 정제염을 섭취하는 집단보다 크게 감소하였 다. 소변 중 칼륨 배설 또한 크게 증가하였다.
결론: 이러한 결과는 고령 환자에서 천일염이 혈압에 유 익한 효과가 있다는 임상 증거를 제공하고 있으며, 한국인 과 같이 충분한 미네랄 섭취가 부족한 경우에 천일염을 사 용하여 더 큰 항고혈압 효과를 가질 수도 있을 것으로 보 인다. 따라서 추가적인 대규모 연구가 요구된다.
중심 단어: 고혈압, 혈압, 고령, 천일염, 무작위 대조 시험
REFERENCES
1. Fields LE, Burt VL, Cutler JA, Hughes J, Roccella EJ, Sorlie P.
The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension 2004;44(4):398-404.
2. McCarty CA, Berg RL, Rottscheit CM, Dart RA. The use of di- etary supplements and their association with blood pressure in a large Midwestern cohort. BMC Complement Altern Med 2013;
13:339.
3. Safar ME, Temmar M, Kakou A, Lacolley P, Thornton SN. Sodium intake and vascular stiffness in hypertension. Hypertension 2009;54(2):203-9.
4. Hu G, Jousilahti P, Peltonen M, Lindström J, Tuomilehto J.
Urinary sodium and potassium excretion and the risk of type 2 diabetes: a prospective study in Finland. Diabetologia 2005;48 (8):1477-83.
5. He FJ, MacGregor GA. A comprehensive review on salt and health and current experience of worldwide salt reduction pro- grammes. J Hum Hypertens 2009;23(6):363-84.
6. Meneton P, Jeunemaitre X, de Wardener HE, MacGregor GA.
Links between dietary salt intake, renal salt handling, blood pressure, and cardiovascular diseases. Physiol Rev 2005;85(2):
679-715.
7. Houston M. The role of magnesium in hypertension and car- diovascular disease. J Clin Hypertens (Greenwich) 2011;13(11):
843-7.
8. Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med 2001;344(1):3-10.
9. Gilleran G, O'Leary M, Bartlett WA, Vinall H, Jones AF, Dodson PM. Effects of dietary sodium substitution with potassium and magnesium in hypertensive type II diabetics: a randomised blind controlled parallel study. J Hum Hypertens 1996;10(8):
517-21.
10. Geleijnse JM, Witteman JC, Bak AA, den Breeijen JH, Grobbee DE. Reduction in blood pressure with a low sodium, high po- tassium, high magnesium salt in older subjects with mild to moderate hypertension. BMJ 1994;309(6952):436-40.
11. China Salt Substitute Study Collaborative Group. Salt sub- stitution: a low-cost strategy for blood pressure control among rural Chinese. A randomized, controlled trial. J Hypertens 2007;25(10):2011-8.
12. Sarkkinen ES, Kastarinen MJ, Niskanen TH, Karjalainen PH, Venäläinen TM, Udani JK, et al. Feasibility and antihypertensive effect of replacing regular salt with mineral salt -rich in magne- sium and potassium- in subjects with mildly elevated blood pressure. Nutr J 2011;10:88.
13. Lee KD, Park JW, Choi CR, Song HW, Yun SK, Yang HC, et al.
Salinity and heavy metal contents of solar salts produced in Jeollanamdo province of Korea. J Korean Soc Food Sci Nutr 2007;36:753-8.
14. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al.; Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.
National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42(6):1206-52.
15. Paik HY. Dietary Reference Intakes for Koreans (KDRIs). Asia Pac J Clin Nutr 2008;17 Suppl 2:416-9.
16. Korean Ministry of Health, Welfare, and Family Affairs &
Korea Centers for Disease Control and Prevention. The Korean National Health and Nutrition Examination Survey - KNHANES IV (2007). Seoul; 2008. [Accessed December 12, 2014]. http://knhanes.cdc.go.kr.
17. Kang Y, Na DL, Hahn S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients.
J Korean Neurol Assoc 1997;15(2):300-8.
18. Won CW, Rho YG, Kim SY, Cho BR, Lee YS. The validity and reliability of Korean Activities of Daily Living (K-ADL) scale. J Korean Geriatr Soc 2002;6(2):98-106.
19. Ku HM, Kim JH, Kwon EJ, Kim SH, Lee HS, Ko HJ, et al. A study on the reliability and validity of Seoul-Instrumental Activities of Daily Living (S-IADL). J Korean Neuropsychiatr Assoc 2004;43(2):189-99.
20. Choi SH, Na DL, Lee BH, Hahm DS, Jeong JH, Jeong Y, et al.
The validity of the Korean version of Global Deterioration Scale. J Korean Neurol Assoc 2002;20(6):612-7.
21. Franklin SS, Gustin W 4th, Wong ND, Larson MG, Weber MA, Kannel WB, et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 1997;96(1):308-15.
22. Susic D, Varagic J, Frohlich ED. Isolated systolic hypertension in elderly WKY is reversed with L-arginine and ACE inhibition.
Hypertension 2001;38(6):1422-6.
23. Haider AW, Larson MG, Franklin SS, Levy D; Framingham Heart Study. Systolic blood pressure, diastolic blood pressure, and pulse pressure as predictors of risk for congestive heart fail- ure in the Framingham Heart Study. Ann Intern Med 2003;
138(1):10-6.
24. Zhou MS, Nishida Y, Yoneyama H, Chen QH, Kosaka H.
Potassium supplementation increases sodium excretion and nitric oxide production in hypertensive Dahl rats. Clin Exp Hypertens 1999;21(8):1397-411.
25. Stolarz-Skrzypek K, Bednarski A, Czarnecka D, Kawecka- Jaszcz K, Staessen JA. Sodium and potassium and the patho- genesis of hypertension. Curr Hypertens Rep 2013;15(2):122- 30.
26. Wu G, Tian H, Han K, Xi Y, Yao Y, Ma A. Potassium magne- sium supplementation for four weeks improves small distal ar- tery compliance and reduces blood pressure in patients with es- sential hypertension. Clin Exp Hypertens 2006;28(5):489-97.
27. Kim MH, Bu SY, Choi MK. Daily calcium intake and its rela- tion to blood pressure, blood lipids, and oxidative stress bio- markers in hypertensive and normotensive subjects. Nutr Res Pract 2012;6(5):421-8.
28. Resnick LM, Laragh JH, Sealey JE, Alderman MH. Divalent cations in essential hypertension. Relations between serum ion- ized calcium, magnesium, and plasma renin activity. N Engl J
Med 1983;309(15):888-91.
29. Jin K, Kim TH, Kim YH, Kim YW. Additional antihypertensive effect of magnesium supplementation with an angiotensin II re- ceptor blocker in hypomagnesemic rats. Korean J Intern Med 2013;28(2):197-205.
30. Maillard MP, Tedjani A, Perregaux C, Burnier M. Calcium-sens- ing receptors modulate renin release in vivo and in vitro in the rat. J Hypertens 2009;27(10):1980-7.
31. Lee KD, Gao TC, Bang MA, Cho JY, Ham KS. Effects of a min- eral-rich solar salt on blood pressure in dahl salt-sensitive rats.
In: 2008 Proceedings of the Korean Society of Post harvest Science and Technology of Agricultural Products Conference.
Gwangju: The Korean society of food preservation; 2008.
p.325-6.
32. Swei A, Lacy F, DeLano FA, Schmid-Schönbein GW. Oxidative stress in the Dahl hypertensive rat. Hypertension 1997;30(6):
1628-33.
33. Ha JO, Park KY. Comparison of autooxidation rate and comu- tagenic effect of different kinds of salt. J Korean Assoc Cancer Prevention 1999;4:44-51.
34. Lee JJ, Kim AR, Chang HC, Lee MY. Antioxidative effects of chungkukjang preparation by adding solar salt. Korean J Food Preserv 2009;16(2):238-45.
35. Jung KO, Lee KY, Rhee SK, Park KY. (2002). Effects of various kinds of salt on the tumor formation, NK cell activity and lipid peroxidation in Sarcoma-180 cell transplanted mice. J Korean Assoc Cancer Prevention 2002;7(2):134-42.
36. Oh KW. Korea National Health and Nutrition Examination Survey (KNHANE) Ⅵ-Ⅰ(2013). Cheongju: Korean Ministry of Health, Welfare, and Family Affairs & Korea Centers for Disease Control and Prevention; 2013. [Accessed December 12, 2014]. http://knhanes.cdc.go.kr/knhanes/index.do.
37. Diet F, Pratt RE, Berry GJ, Momose N, Gibbons GH, Dzau VJ.
Increased accumulation of tissue ACE in human atherosclerotic coronary artery disease. Circulation 1996;94(11):2756-67.
38. Sheppard RJ, Schiffrin EL. Inhibition of the renin-angiotensin system for lowering coronary artery disease risk. Curr Opin Pharmacol 2013;13(2):274-9.
39. Kohlstedt K, Trouvain C, Boettger T, Shi L, Fisslthaler B, Fleming I. AMP-activated protein kinase regulates endothelial cell angiotensin-converting enzyme expression via p53 and the post-transcriptional regulation of microRNA-143/145. Circ Res 2013;112(8):1150-8.