https://doi.org/10.35827/cp.2019.18.2.76
접수일: 2019년 8월 7일, 게재승인일: 2019년 10월 16일 책임저자: 김대환, 수원시 영통구 월드컵로 164
16499, 아주대학교병원 재활의학과 Tel: 031-219-5507, Fax: 031-219-4360 E-mail: [email protected]
동결견 환자에서 관절강내 스테로이드 주사 후 관절가동범위의 변화
아주대학교병원 재활의학과
조형준ㆍ윤승현ㆍ김민철ㆍ김대환
Changes in Range of Motion after Intra-Articular Corticosteroid Injection in Frozen Shoulder:
A Retrospective 3-Month Follow-Up Study
Hyoung Jun Cho, M.D., Seung-Hyun Yoon, M.D., Ph.D., Minchul Kim, M.D. and Dae Hwan Kim, M.D.
Department of Physical Medicine and Rehabilitation, Ajou University Medical Center, Suwon, Korea
Objective: To examine (1) the degree of reduction of passive range of motion (PROM) on the affected side compared to that on the unaffected side and (2) the degree of increase in PROM following intra-articular corticosteroid injection (IACI) in patients with frozen shoulder. Method: The medical records of 120 patients with frozen shoulder were retrospectively reviewed.
PROM of the unaffected and affected shoulder (flexion, extension, abduction, internal rotation, external rotation) was compared, and changes in PROM of the affected shoulder after a single IACI (triamcinolone 20 mg) were evaluated after 12 weeks.
Results: At the time of diagnosis, PROM of the affected shoulder was most limited in external rotation, followed by internal rotation, abduction, extension, and flexion, compared to that of the unaffected shoulder. Compared to before IACI, PROM of external rotation demonstrated the greatest increase compared to all the other movements after IACI. Conclusion: Limitation in PROM of the frozen shoulder at the time of diagnosis was greatest for external rotation. Moreover, external rotation experi- enced the greatest improvement after IACI. Our findings should help to further clarify the clinical characteristics of frozen shoulder, aid in its diagnosis, and allow the prediction of the effects of IACI. (Clinical Pain 2019;18:76-81)
Key Words: Frozen shoulder, Intra-articular injection, Corticosteroids, Passive range of motion
INTRODUCTION
Frozen shoulder, also known as adhesive capsulitis, is a long-lasting, painful shoulder disorder. The disorder is caused by progressive fibrosis and eventual contracture of the capsule of the glenohumeral joint, which causes stiff- ness and pain.1,2 The treatment for frozen shoulder includes rehabilitation exercises and physical modalities, non- steroidal antiinflammatory drugs, intra-articular cortico- steroid injection (IACI), capsule distension, and arthro- scopic capsular release.1-5
IACI is one of the most common treatments for frozen shoulder. It targets the inflammatory process at the gleno- humeral joint. Reports reveal that IACI is effective for the rapid decrease of pain and improvement of passive range
of motion (PROM).6,7
Frozen shoulder is provoked by inflammation of the joint capsule and synovium, which eventually results in contracture of the capsule.8 This capsular contracture caus- es the global limitation of PROM of the glenohumeral joint. Limitation of PROM is an important clinical feature in frozen shoulder because it is an essential diagnostic cri- terion for this condition.9 Evaluating the changes in PROM after treatment is important for determining the effective- ness of treatment. Some authors have described that limi- tation of passive external rotation is common in frozen shoulder, but it is still controversial.1,10-12 There are few studies that quantified the degree of reduction of PROM in each plane in the affected side to support their arguments. Moreover, only a few studies have investigated the degree of improvement of PROM of the glenohumeral joint in all planes after IACI.
In the present study, we aimed to examine (1) the degree of reduction in PROM on the affected side compared to that on the unaffected side and (2) the degree of increase in PROM following IACI in patients with frozen shoulder.
MATERIALS AND METHODS 1. Subjects and study design
This study was a retrospective comparative study based on medical records from an outpatient rehabilitation clinic of a university hospital. Informed consent was waived for this retrospective study approved by the institutional review board at the university hospital. Between January 1, 2013 and December 31, 2018, 120 patients with frozen shoulder were reviewed retrospectively. All the patients underwent standardized history taking, physical examination, and shoulder ultrasonography. Evaluations for active range of motion, PROM, and muscle strength, and tests for rotator cuff tendinopathy and impingement were also conducted at the time of initial diagnosis.
The inclusion criteria for the study were as follows: (1) patients who had frozen shoulder with a normal radiog- raphy finding of the affected shoulder and restriction of PROM of > 30° in 2 or more planes of movement,9,13 (2) stage 2 frozen shoulder (frozen stage) according to Hannafin and Chiaia,1 and (3) at least 2 months of pain.
Patients were excluded if they had any of the following:
secondary frozen shoulder (secondary to other causes in- cluding inflammatory, metabolic, or infectious arthritis;
cerebrovascular accident; tumor; or fracture), rotator cuff lesion on both physical and ultrasonographic examinations, and full-thickness tear of the rotator cuff on ultrasono- graphic examination.
2. Intervention
IACI was performed with ultrasound guidance. A mix- ture of 2 mL of 10 mg/mL triamcinolone acetonide and 4 mL of 1% lidocaine was injected using a 23-gauge 6-cm-long needle behind the shoulder, with the needle positioned parallel to the transducer. After injection, pa- tients received leaflet and were educated by physical thera- pists to do a home exercise program for increasing the range of motion, including stretching forward and bending down to a desk, and the Codman exercise, wall-climbing exercise, external and internal rotation with bar, and poste- rior shoulder stretch.14 No nonsteroidal anti-inflammatory drugs, analgesics, or opioids were prescribed after injec- tion.
3. Outcome measurement
PROM in all planes of the shoulder except adduction was measured for both the affected and unaffected sides at the time of initial diagnosis and 12 weeks after injection.
To identify the limitation of motion of the affected side compared to the unaffected side at the time of diagnosis, the fraction of PROM of the affected side compared to that of the unaffected side (PROM of the affected side/PROM of the unaffected side) was calculated for each plane. In addition, to examine the changes in PROM of the affected side 12 weeks after injection, PROM change rate (amount of change in PROM after injection/PROM before injection) was calculated. The common follow up interval of the hos- pital was 4, 8 and 12 weeks. In this study, follow up inter- val was selected as 12 weeks to see the long-term effect rather than the short-term effect of IACI. PROM for for- ward flexion, abduction, and external rotation were meas- ured in the supine position using a goniometer. External ro- tation was measured in 0° abduction of the shoulder and 90° flexion of the elbow.
4. Statistical analysis
All data were analyzed using R 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria). Continuous data are presented as means and SDs, and categorical data are presented as frequencies and percentages. The joint move- ment with the most severe limitation in PROM was identi- fied using one-way analysis of variance (ANOVA), with the Bonferroni test as the post-hoc test. The degree of im- provement in PROM 12 weeks after corticosteroid injection was analyzed with the paired t-test after a test for normality was conducted. The changes in PROM after IACI were evaluated based on the PROM change rate after injection.
The plane of joint movement with the greatest improve- ment was determined by analyzing this change rate with one-way ANOVA and Bonferroni test. Statistical sig- nificance was set at p<0.05.
RESULTS 1. Characteristics of patients
A total of 120 patients were enrolled. The mean patient age was 54.1 ± 4.7 years. Thirty-four (28%) of the patients were men and 86 (72%) were women. The dominant
Table 3. Changes in Passive Range of Motion of the Affected Shoulder after Intra-articular Corticosteroid Injection
Flexion Extension Abduction Internal rotation External rotation
Pre-injection (°) 134 ± 16.4 33 ± 13.2 85 ± 18.4 34 ± 15.1 35 ± 16.2
Post-injection (°)* 158.1 ± 11.4 47.3 ± 11.6 125.2 ± 25.1 54.4 ± 16.0 57.1 ± 16.8
Ratio (%)† 17.7 41.6 46.6 56.4 62.5
Mean ratio (%)*,‡ 19.2 ± 15.4 56.6 ± 51.9 54.1 ± 50.5 80.1 ± 83.0 108 ± 172.9 Values are presented as mean ± standard deviation or as numbers.
†Ratio (%) = amount of change in PROM after injection/PROM before injection. ‡Mean ratio (%): mean value of the raw ratio, compared with one-way analysis of variance.
*p<0.001.
Table 1. Passive Range of Motion of the Affected and Unaffected Shoulder
Flexion Extension Abduction Internal rotation External rotation
Unaffected side (°) 158 ± 14.6 54 ± 10.7 161 ± 17.5 79 ± 17.6 99 ± 16.7
Affected side (°) 134 ± 16.4 33 ± 13.2 85 ± 18.4 34 ± 15.1 35 ± 16.2
Ratio (%)† 84.9 61.5 52.9 44.0 35.2
Mean ratio (%) *,‡ 85.8 ± 14.1 62.4 ± 24.0 53.8 ± 14.4 45.4 ± 21.3 36.3 ± 18.3 Values are presented as mean ± standard deviation or as numbers.
†Ratio (%) = PROM of the affected side/PROM of the unaffected side. ‡Mean ratio (%) = mean value of the raw ratio, compared with one-way analysis of variance.
*p<0.001.
Table 2. Post-hoc Test for Limitation in Passive Range of Motion in the Affected Shoulder prior to Intra-articular Corticos- teroid Injection
External rotation
Internal
rotation Abduction Extension
Internal rotation <0.001 - - -
Abduction <0.001 <0.001 - -
Extension <0.001 <0.001 <0.001 - Flexion <0.001 <0.001 <0.001 <0.001 shoulder was affected in 54 patients (45%) and the
non-dominant shoulder was affected in 66 patients (55%).
The mean duration of pain was 7.01 ± 2.32 months.
2. Limitation in PROM due to frozen shoulder prior to injection
The mean PROM of the unaffected shoulder was 158 ± 14.6º flexion, 54 ± 10.7º extension, 161 ± 17.5º abduction, 79 ± 17.6º internal rotation, and 99 ± 16.7º external rotation. For the affected shoulder, flexion was limited to 84.9% (134 ± 16.4º), extension 61.5% (33 ± 13.2º), abduc- tion 52.9% (85 ± 18.4º), internal rotation 44.0% (34 ± 15.1º), and external rotation to 35.2% (35 ± 16.2º) of the PROM of the unaffected shoulder, showing the significant difference in mean ratio between each planes (p<0.001, all; Table 1). When comparing the degree of limitation of PROM between each plane, it showed the greatest limi- tation for external rotation, followed by internal rotation, abduction, extension, and flexion (Table 2).
3. Changes in PROM after IACI
PROM of the affected shoulder was measured 12 weeks after IACI. Compared to that prior to IACI, flexion was improved by 17.7%, extension by 41.6%, abduction by 46.6%, internal rotation by 56.4%, and external rotation by 62.5%. Improvement in PROM was significant in all planes and there was also significant difference in mean ra- tio between each plane (p<0.001, all; Table 3). When comparing the superiority of change rate of PROM be-
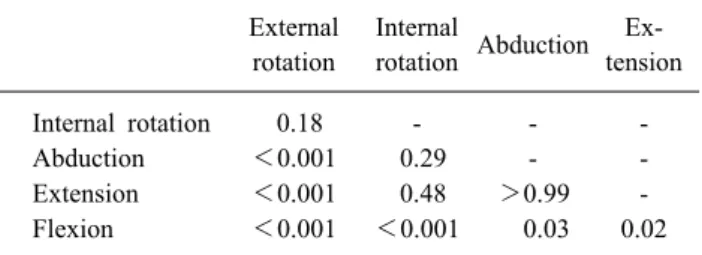
Table 4. Post-hoc Test for Change Rate in Passive Range of Motion in the Affected Shoulder after Intra-articular Corticoster- oid Injection
External rotation
Internal
rotation Abduction Ex- tension
Internal rotation 0.18 - - -
Abduction <0.001 0.29 - -
Extension <0.001 0.48 >0.99 -
Flexion <0.001 <0.001 0.03 0.02
tween each plane, external rotation was more significantly improved than extension, flexion, and abduction. However, the degree of improvement was not significantly different from that for internal rotation. There was significantly less improvement in flexion compared to all other planes (Table 4).
DISCUSSION
To our knowledge, our study is the first to quantify and compare the degree of improvement in PROM in each plane following IACI among patients with frozen shoulder.
This study showed that (1) limitation in PROM of the af- fected shoulder at the time of diagnosis was greatest for external rotation, followed by internal rotation, abduction, extension, and flexion and that (2) PROM of external rota- tion was improved the most after IACI.
The marked limitation in PROM noted for external rota- tion at the time of diagnosis seems related to the con- tracture of the anterior capsule. Although fibroplasia of the entire capsule causes global limitation,15 the limitation in external rotation is known to be particularly severe because the contracture of the anterior capsule is more severe com- pared to that of other capsule regions.11,16,17 Contracture particularly occurs in the coracohumeral ligament at the ro- tator interval, and some studies showed that anterior capsu- lar release improves PROM of external rotation in patients with refractory frozen shoulder.18
Currently, there are several clinical diagnostic criteria for frozen shoulder due to the lack of a clear consensus on the degree of limitation of PROM for the diagnosis of frozen shoulder. Regarding diagnostic criteria, some authors used a limitation of external rotation,19,20 while many others did not.21-24 Frozen shoulder is characterized by global limi-
tation, but in the present study, we showed that the limi- tation in external rotation caused by anterior capsule con- tracture was the most characteristic feature with specific supporting data. Although the limitation of external rota- tion was the most important characteristic, it is currently not included in most diagnostic criteria. We strongly sug- gest that the limitation in external rotation should be in- cluded in the diagnostic criteria for frozen shoulder.
Despite our findings, few studies show the specific data that a limited external rotation is the most common limi- tation in PROM of the shoulder. Neviaser et al.10 described that early loss of external rotation is a hallmark of frozen shoulder. Likewise, Hannafin et al.1 reported that external rotation is the most limited plane in frozen shoulder. But there is no specific supporting data in both of them. In one study that quantified the degree of PROM in 30 patients with frozen shoulder, the authors showed that external rota- tion of the affected shoulder was significantly limited com- pared to internal rotation and abduction,25 and this is con- sistent with our findings. However, their study had a small sample and only examined 3 planes of shoulder joint movement (external rotation, internal rotation, and abduc- tion).
Passive external rotation was more significantly im- proved after IACI compared to the other planes, with the exception of internal rotation. This is because the limitation in external rotation is more related to localized inflam- mation and consequently to the contracture of the anterior capsule, as opposed to the contracture of the global cap- sule. For this reason, the anti-inflammatory effect of IACI would have been effective for improving PROM of ex- ternal rotation. In one meta-analysis study about the effects of IACI in patients with frozen shoulder showed that PROM in all planes was significant improved after IACI.26 However, when reviewing the individual studies, none of them calculated the rate of improvement of the degree and compared the superiority between each planes. Not only did our study quantify the degree of improvement after IACI, but it also compared the superiority between each plane.
Our study analyzed the degree of improvement of PROM after IACI using the change rate of PROM. When analyzing with the amount of change of PROM, abduction was the most improved plane. Differences in the results of the two methods might be the limitation for this study.
However, since the normal values of PROM of each plane are all different, using the amount of change of PROM may produce the unstandardized results. Our study was intended to obtain standardized results using the change rate of PROM.
The fact that we examined changes in PROM after in- jection in the present study has the following clinical implications. First, because external rotation is most notice- ably limited in frozen shoulder, IACI can be selected from various treatment methods as the most effective therapy for improving PROM of external rotation. Second, the degree of improvement in PROM after IACI can be predicted.
One strength of this study is that it presented evidence supporting previous arguments that external rotation is the most limited movement in frozen shoulder and that PROM of external rotation is the most improved after IACI.
However, our study has some limitations. First, it is limited by its retrospective design. Second, after IACI, patients were educated by physical therapists to do a home exercise program including stretching exercise and could not verify that all patients had carried out what they had been educated. This might have affected the measured PROM.
Further study that considers such limitation will be needed in the future.
CONCLUSION
Limitation in PROM of frozen shoulder at the time of diagnosis was greatest for external rotation, followed by in- ternal rotation, abduction, extension, and flexion. More- over, external rotation demonstrated the greatest improve- ment after IACI. The findings of this study should help clarify the clinical characteristics of frozen shoulder, aid in its diagnosis, and allow the prediction of the effects of IACI.
REFERENCES
1. Hannafin JA, Chiaia TA. Adhesive capsulitis. A treatment approach. Clin Orthop Relat Res 2000; 372: 95-109 2. Neviaser AS, Neviaser RJ. Adhesive capsulitis of the
shoulder. J Am Acad Orthop Surg 2011; 19: 536-542 3. Blockey NJ, Wright JK, Kellgren JH. Oral cortisone ther-
apy in periarthritis of the shoulder; a controlled trial. Br Med J 1954; 1: 1455-1457
4. Chambler AF, Carr AJ. The role of surgery in frozen
shoulder. J Bone Joint Surg Br 2003; 85: 789-795 5. Tveita EK, Tariq R, Sesseng S, Juel NG, Bautz-Holter E.
Hydrodilatation, corticosteroids and adhesive capsulitis: a randomized controlled trial. BMC Musculoskelet Disord 2008; 9: 53
6. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev 2003; 1:
CD004016
7. Marx RG, Malizia RW, Kenter K, Wickiewicz TL, Hannafin JA. Intra-articular corticosteroid injection for the treatment of idiopathic adhesive capsulitis of the shoulder.
HSS J 2007; 3: 202-207
8. Johnson AJ, Godges JJ, Zimmerman GJ, Ounanian LL.
The effect of anterior versus posterior glide joint mobi- lization on external rotation range of motion in patients with shoulder adhesive capsulitis. J Orthop Sports Phys Ther 2007; 37: 88-99
9. Warner JJ. Frozen shoulder: diagnosis and management. J Am Acad Orthop Surg 1997; 5: 130-140
10. Neviaser AS, Hannafin JA. Adhesive capsulitis: a review of current treatment. Am J Sports Med 2010; 38: 2346- 2356
11. Robinson CM, Seah KT, Chee YH, Hindle P, Murray IR.
Frozen shoulder. J Bone Joint Surg Br 2012; 94: 1-9 12. Uppal HS, Evans JP, Smith C. Frozen shoulder: A system-
atic review of therapeutic options. World J Orthop 2015;
6: 263-268
13. Buchbinder R, Green S, Forbes A, Hall S, Lawler G.
Arthrographic joint distension with saline and steroid im- proves function and reduces pain in patients with painful stiff shoulder: results of a randomised, double blind, place- bo controlled trial. Ann Rheum Dis 2004; 63: 302-309 14. Matsen FA LS, Sidles J, Harryman DT. Practical evaluation
and management of the shoulder, Philadelphia: Saunders, 1994, 45-49
15. Tamai K, Akutsu M, Yano Y. Primary frozen shoulder:
brief review of pathology and imaging abnormalities. J Orthop Sci 2014; 19: 1-5
16. Uhthoff HK, Boileau P. Primary frozen shoulder: global capsular stiffness versus localized contracture. Clin Orthop Relat Res 2007; 456: 79-84
17. Lee SY, Lee KJ, Kim W, Chung SG. Relationships between capsular stiffness and clinical features in adhesive capsu- litis of the shoulder. PM R 2015; 7: 1226-1234
18. Hsu JE, Anakwenze OA, Warrender WJ, Abboud JA.
Current review of adhesive capsulitis. J Shoulder Elbow Surg 2011; 20: 502-514
19. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clinical study with an eval- uation of three treatment regimens. Ann Rheum Dis 1984;
43: 353-360
20. Watson L, Dalziel R, Story I. Frozen shoulder: a 12-month clinical outcome trial. J Shoulder Elbow Surg 2000; 9:
16-22
21. Lundberg BJ. The frozen shoulder. Clinical and radio- graphical observations. The effect of manipulation under general anesthesia. Structure and glycosaminoglycan con- tent of the joint capsule. Local bone metabolism. Acta Orthop Scand Suppl 1969; 119: 1-59
22. Kay NR. The clinical diagnosis and management of frozen shoulders. Practitioner 1981; 225: 164-167
23. Rizk TE, Pinals RS. Frozen shoulder. Semin Arthritis
Rheum 1982; 11: 440-452
24. Neviaser RJ. Painful conditions affecting the shoulder. Clin Orthop Relat Res 1983; 173: 63-69
25. Mitsch J, Casey J, McKinnis R, Kegerreis S, Stikeleather J. Investigation of a consistent pattern of motion restriction in patients with adhesive capsulitis. J Man Manip Ther 2004; 12: 153-159
26. Sun Y, Zhang P, Liu S, Li H, Jiang J, Chen S, et al.
Intra-articular steroid injection for frozen shoulder: a sys- tematic review and meta-analysis of randomized controlled trials with trial sequential analysis. Am J Sports Med 2017;
45: 2171-2179