Alcoholic liver disease
소화기내과학 교실 신 현필
Alcoholic liver disease in Korea
우리나라 간경변증 원인 :B 형 간염 이어 2 위
간세포암종 : B 형 (70% 이상 )>C 형 (12% 대 )> 알코올
우리나라 과다 음주자 : 남성 ( 일 40g), 여성 ( 일 20g) 비율 약 7%
B 형 간염 예방 , C 형 간염 완치율 증가
2000 년 이후 간암 : B 형 간염 관련 감소하고 Non-B, Non-C 증가세
Alcoholic liver disease ( 3 main lesion)
Normal liver
Fatty liver
Alcoholic hepatitis Cirrhosis 80-90%
10-30% 8-20%
? (40%)
Am J Gastroenterol 1998; 93:2023
Alcohol metabolism
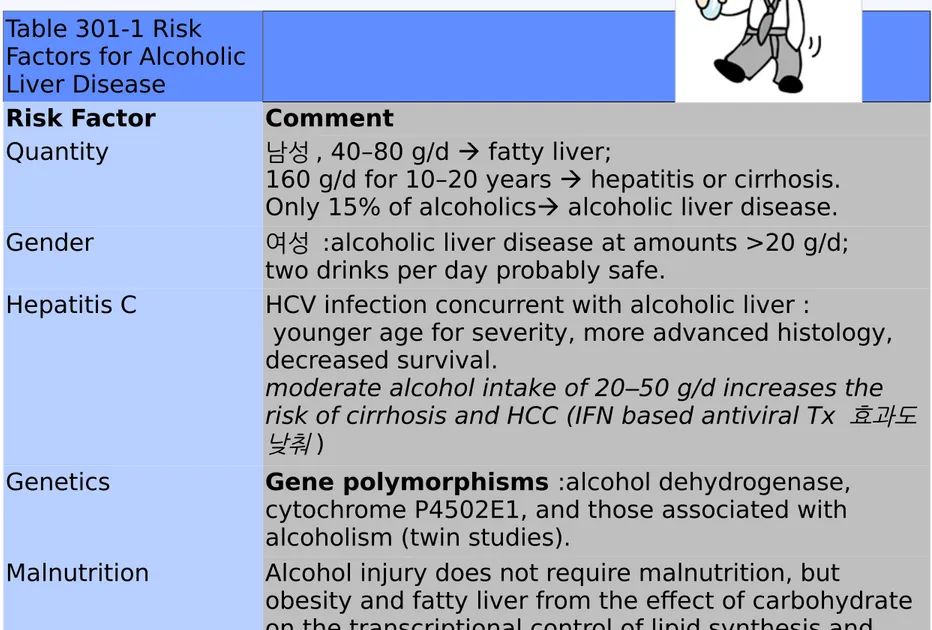
Table 301-1 Risk Factors for Alcoholic Liver Disease
Risk Factor Comment
Quantity 남성 , 40–80 g/d fatty liver;
160 g/d for 10–20 years hepatitis or cirrhosis.
Only 15% of alcoholics alcoholic liver disease.
Gender 여성 :alcoholic liver disease at amounts >20 g/d;
two drinks per day probably safe.
Hepatitis C HCV infection concurrent with alcoholic liver :
younger age for severity, more advanced histology, decreased survival.
moderate alcohol intake of 20–50 g/d increases the risk of cirrhosis and HCC (IFN based antiviral Tx 효과도 낮춰 )
Genetics Gene polymorphisms :alcohol dehydrogenase, cytochrome P4502E1, and those associated with alcoholism (twin studies).
Malnutrition Alcohol injury does not require malnutrition, but
obesity and fatty liver from the effect of carbohydrate on the transcriptional control of lipid synthesis and transport may be factors. Patients should receive vigorous attention to nutritional support.
알코올을 하루 80g
소주 300-370cc = 양주 150cc = 맥주 1500-2000cc = 포도주 750cc
Pathogenesis
P450 약물대사 억제하고 간독성
Collagen 합 성 늘리고 fibrosis 새로운 항원으로 작용하여
cytotoxic T lymphocyte 반응 등 유
발
Hepatocyte apoptosis and
necrosis 유발 Complex interaction- alcohol mediated liver
injury :key
Complex interaction- alcohol mediated liver injury :key
Alcoholic fatty liver
처음에 보이는 가장 흔한 조직학적 반응
과음자의 80-90%
알코올 산화
니코틴아마이드아데닌 다이뉴클레오티드 (NADH) 생성증가
중성지방 , 지방산 생성증가
지방조직에서 간으로 유리지방산 유입증가 , 내장점막에서 유미지립
증가 (Chylomicron) 유입증가
AMPK 활성 저하 지방질 생합성 증가
PPAR-a 억제 지방산 분해 감소
Acetaldehyde – mitochondria 와 microtubule 손상 VLDL 축적
Alcoholic fatty liver
Extensive fatty change and distortion of the hepatocytes with macrovesicular fat
( 간세포가 fat droplet 에 의해 팽창되고 핵을 세포막쪽으로 미는 )
Hepatomegaly – 간혹 , 유일한 소견
DDx : alcoholic and non alcoholic ??
음주력이 가장 중요
금주시 정상화 .
지속 음주시는 30% 이상에서 간경화로 진행가능
Progressive liver injury 관련 steatohepatitis +
giant mitochondria, perivenular fibrosis, and macrovesicular fat
Cause of fatty liver
Alcoholic hepatitis
Hallmark 1. Spotty necrosis
2. PMN (polymorphonuclear) infiltration
3. Perivenular & perisinusoidal space of Disse fibrosis
음주 지속시 간섬유화 진행이 가속알코올성 간염 50% 에서 조직검사상 간경병 동반 4. Mallory body (70-75%) : not specific & not diagnostic
진단에 생검이 이용되지만 항상 필요한 것은 아니다 !
.
Alcoholic hepatitis
Clinical features
Alcoholic hepatitis : 광범위한 clinical features.
Cytokine production
systemic manifestations of alcoholic hepatitis 관련 .
Fever (modest), spider nevi, jaundice, abdominal pain - extreme << asymptomatic
Portal hypertension, ascites, or variceal bleeding : without cirrhosis.
Laboratory Features (I)
Alcoholic Fatty Liver and Alcoholic Hepatitis
AST Increased two- to sevenfold, <400 U/L, greater than ALT
ALT Increased two- to sevenfold, <400 U/L AST/ALT Usually >1
GGTP Not specific to alcohol, easily inducible,
모든 fatty liver, DM, smoking 등에서 영향 음주자의 금주 여부 판단
Bilirubin May be markedly increased in alcoholic hepatitis despite modest elevation in alkaline phosphatase
PMN If >5500/ ㎕ predicts severe alcoholic hepatitis when discriminant function > 32
Laboratory Features (II)
Hypertriglyceridemia, hypercholesterolemia 도 가능
Hepatocyte synthetic function 악화 :
more serious
Hypoalbuminemia and coagulopathy Anemia 유발기전
: acute & chronic GI blood loss : nutritional deficiency
: hypersplenism : hemolytic anemia
: direct toxic effect on BM
LFT
Prognosis
ALD mortality 예측인자 : PT, bilirubin
Severe alcoholic hepatitis :
bil>8mg/dL, PT 5 초 이상 연장 , Alb<2.5mg/dL, anemia, ascites, renal failure
Discriminate function :
4.6 x [prothrombin time control (seconds)]
+ serum bilirubin (mg/dL)
Dismal prognosis (discriminant function > 32).
ascites, variceal hemorrhage,
deep encephalopathy, or hepatorenal syndrome
Other prognosis scoring system
9 점 이상- 스테로이드 효과
Treatment (I)
① 금주
Conunselors – 환자 별 접근
Daily drinking( 중단해 본적 없어 ) and binge drinking ( 몇 달 중단 가능 ) Naltrexone(opioid antagonist), acamprostate(taurina analogue)
-- 음주시 high 및 priming 줄여줘
-- 과거 disufiram 과 달리 음주 가능 : 속이지는 않아 ② Multi vitamin
Thiamine (Wernicke-Korsakoff disease) ③ Nutritional support
④ Severe alcoholic hepatitis
Treatment (II)
Glucocorticoids.
Discriminant function > 32 ( 참고 MELD>18, GHAS 9 이상 )
Prednisone, 40 mg/d, or prednisolone, 32 mg/d, for 4 weeks followed by a steroid taper
Exclusion criteria:
active gastrointestinal bleeding, sepsis, renal failure, or pancreatitis.
Women with encephalopathy from severe alcoholic hepatitis
particularly good candidates
Effect of glucocorticoid therapy of severe alcoholic hepatitis on short-term survival
Treatment (III)
Pentoxyfylline 400mg tid x 4 weeks
Glucocorticoid alternative, 원래 말초혈관 혈액순환 개선제
경구 phophodiesterase 억제제 : Non specific TNF inhibitor( 다른 cytokines 과 함께 TNFa 도 억제 )
Steroid 사용에 따른 부작용 없다 – GI bleeding, renal failure 시 장점 A/N, Stress 가 문제
Neutralizing monoclonal Ab specific for TNF (infliximab) -> secondary infection, TFN 는 간세포 Necrosis 외에 재생 역할도 한다는 점
Transplantation – Not candidate
-surgical mortality, recidivism
Wernicke-Korsakoff syndrome
Neurologic complication of thiamine (Vit. B1) deficiency
Two different syndromes
Wernicke's encephalopathy (WE)
acute syn. death and neurologic morbidity.
Korsakoff's amnestic syndrome (KS) :
chronic neurologic condition, : consequence of WE.
WK syndrome- pathology
Thiamine deficiency in alcohol abusers : dietary intake ↓ + GI absorption ↓
+ hepatic storage ↓+ impaired utilization
Thiamine (vitamin B1) : Major role as cofactor or coenzymes in energy(glucose) metabolism
Thiamine 가장 필요 :
높은 metabolic demand 와 높은 glucose intake.
Thiamine 투여 전에 admin. of iv glucose thiamine 에 대한 요구 급격히 증가
Atrophy of the mamillary bodies
: highly specific finding (up to 80 %)WK syndrome- Diganosis
Classic triad of Wernicke‘s encephalopathy
1. Encephalopathy
2. Oculomotor dysfunction
3. Gait ataxia
All classic triad in 17 % none in 19 %.
No laboratory studies : diagnostic of WE.
Not necessary in all patients, not delay treatment.
hyperintensity
in the periaqueductal region of the
midbrain
mammillary bodies
thalamus
bilateral symmetrical hyperintensity in the frontal-parietal
cortices
WK syndrome- Treatment and prognosis
The diagnosis : difficult to confirm
IV administration of thiamine :
safe, simple, inexpensive, and effective
Adverse reactions: anaphylaxis and bronchospasm
100 mg of thiamine iv or for five consecutive days.
Prompt thiamine improvement in ocular signs within hours to days fail other diagnosis ?
Recovery of vestibular function : 2nd week after Therapy improvement in gait ataxia
Confusion subsides : days ~ weeks
WK syndrome- Prognosis
Signal abnormality on MRI resolves with clinical improvement
In the largest cohort : residual deficits
Gaze palsies recovered completely in most cases
Only about 40 % recovered from ataxia
Prevention
Wernicke's encephalopathy (WE) may be iatrogenically precipitated by glucose loading
To avoid this complication in ED
thiamine prior to or along with glucose infusion.
The prevention of WE and Korsakoff's amnestic syndrome : oral thiamine to outpatients at risk.
The low cost and safety of oral thiamine : alcohol abusers
others at risk for developing thiamine deficiency.