□ 원 저 □
Vol. 11. No. 1, 2008
25
뇌실복막 우회술: 복강경하 원위부 우회관 삽입술의 유용성
건국대학교 의학전문대학원 외과학교실, 1신경외과학교실
심진석ㆍ유영범ㆍ이해원ㆍ장성환ㆍ조 준1ㆍ문창택1ㆍ고영초1ㆍ윤익진
Ventriculoperitoneal Shunts: the Usefulness of Laparoscopic-assisted Distal Shunt Placement
Jin Seok Sim, M.D., Young Bum Yoo, M.D., Hae Won Lee, M.D., Seong Hwan Chang, M.D., Joon Cho, M.D.1, Chang Taek Moon, M.D.1, Young Cho Kho, M.D.1, Ik Jin Yun, M.D.
Departments of Surgery and 1Neurosurgery, Konkuk University School of Medicine, Seoul, Korea Purpose: Distal ventriculoperitoneal shunt catheter placement
has traditionally been performed using a small abdominal incision. However, because this is done blindly, shunt failure frequently occurs secondary to inaccurate peritoneal catheter tip placement. Although laparoscopy has been used to facilitate peritoneal catheter placement, it is not usually the primary method. This study aimed to determine the usefulness and potential advantages of laparoscopic distal catheter placement as the primary approach through comparison with conventional minilaparotomy technique.
Methods: Between August 2005 and December 2007, 80 patients with hydrocephalus (no neonates) underwent ventriculoperitoneal shunt placement at Konkuk University Medical Center. Forty-nine patients underwent laparoscopic distal shunt placement during this period. The results were compared with those of another group of 31 patients who underwent surgery by conventional approach, using retro- spective analysis.
Results: No statistically significant difference in the rate of
shunt faillure was noted between the two groups. Age, sex, underlying disease, preoperative infectious disease, pre- operative leukocytosis, preoperative increased C-reactive protein (CRP), and operative time proved to be insignificant risk factors for inducing shunt failure. Shunt failure was increased principally due to shunt malfunction in patients in the mini-laparotomy group who had undergone previous abdominal surgery. However, shunt malfunction was sig- nificantly reduced by laparoscopic distal catheter placement.
Conclusion: The advantage of the laparoscopic approach was confirmed by noting precise catheter positioning and assessing cerebrospinal fluid (CSF) flow under direct visualization. We recommend laparoscopic-assisted distal ventriculoperitoneal shunt placement as a primary technique.
Key words: Laparoscopy, Peritoneal distal catheter, Ventri- culoperitoneal shunt
중심단어: 복강경, 복강내 원위부 단락관, 뇌실복막단락술
※ 통신저자:윤익진, 서울시 광진구 화양동 1번지 우편번호:143-701
건국대학교 의학전문대학원 외과학교실 Tel:02-2030-7583, Fax:02-2030-5822 E-mail:[email protected]
본 연구의 주요내용은 2008년 대한내시경복강경외과학회 춘계학 술대회에서 포스터 발표되었음.
서 론
뇌실복막 우회술은 수두증의 대표적인 수술적 치료방법 이다. 두정부 또는 전두부의 두개골에 구멍을 낸 다음 뇌실 관을 삽입하여 측뇌실을 천자하고 우회관을 피부 밑으로 통과하게 한 후 복강내로 삽입하여 뇌척수액을 복강내로 유도하는 수술이다. 그러나 전통적인 개복을 통한 윈위부 우회관 삽입술은 시술 과정에서 우회관의 위치가 정확하게 삽입 되었는지, 꺽이거나 막히지는 않았는지 등의 여부는 알 수가 없다. 최근 복강경하에 원위부 우회관 삽입술이 선
택적으로 시행되어지면서 수술자가 직접 눈으로 우회관의 위치 및 기능을 확인할 수 있어 개복을 통한 윈위부 우회관 삽입술에 비해 우월하다는 연구보고가 있다.1-10 저자들은 본 연구를 통해 뇌실복막 우회술 시행시 일차적 술식으로 써 복강경하 원위부 우회관 삽입술의 유용성을 알아보고자 한다.
대상 및 방법
2005년 8월 1일부터 2007년 12월 31일 까지 건국대학교 병원 신경외과에서 뇌실복막 우회술을 시행 받은 신생아를 제외한 80명의 환자를 대상으로 하였다. 신경외과의 뇌실 천자 및 원위부 우회관의 피하 통과가 끝난 후 외과에서 복강내 원위부 우회관 삽입술을 시행 하였다. 개복을 통한 원위부 우회관 삽입술은 전통적 방법으로써 주로 우상복부 에서 2.5∼3 cm정도의 절개창으로 복강내로 원위부 우회관 을 삽입시켰다. 복강경하에 우회관 삽입술을 시행할 경우
Table 1. Characteristics and clinical data of patients
Open peritoneal Laparoscopic peritoneal Total
catheter placement catheter placement (n=80)
(n=31) (n=49)
Sex (M/F) 42/38 16/15 25/24
Age (yr) 53.70±17.01 (9∼85) 46.03±19.38 (9∼77) 57.77±14.05 (17∼85)
<60 48 23 25
≥60 32 8 24
Underlying disease 46 16 30
HTN 34 12 22
DM 13 6 7
CRF 1 1 0
Malignancy 4 0 4
Others 10 3 7
History of abdominal surgery 19 7 12
Preoperative infectious disease 26 6 20
Preoperative leukocytosis (WBC>10,000μl) 9 4 5
Preoperative increased CRP (>0.3 mg/dl) 32 11 21
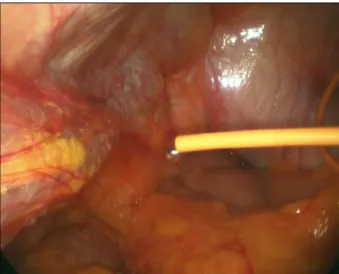
Operative time (min) 148±49.80 (60∼298) 163.16±47.69 (107∼298) 138.95±49.28 (60∼286) Fig. 1. Laparoscopic direct visualization of peritoneal CSF drainage.
에는 배꼽아래에서 0.7 cm 크기로 피부절개 후 5 mm 투관 침을 삽입하고 기복강을 만든 후 복강경 카메라를 적용하 였으며 우회관은 우상복부에서 복강경의 직접적 시야 하에 복막을 뚫고 뇌척수액의 배액을 확인 후 우측 골반강내로 위치 시켰다(Fig. 1). 이 과정에서 대부분 1개의 5 mm 투관 침이 추가적으로 필요하였다. 후향적 조사를 통하여 두 군 간의 성별, 나이, 기저질환, 수술전 감염성 질환의 유무, 수 술전 백혈구증, 수술전 C-reactive protein (CRP) 상승, 수술 시간 등에 따른 우회술 실패율 및 우회술 실패의 원인에 대해 비교분석 하였으며 Chi-square 검정을 통하여 p value 가 0.05 미만인 경우를 유의성이 있다고 판단하였다. 우회
술 실패는 우회관 감염 또는 우회관의 기능적 이상에 의하 여 뇌실복막 우회관을 유지 할 수 없는 경우로 정하였다.
결 과
전체 80명의 환자 중 31명은 개복을 통한 원위부 우회관 삽입술을 받았고 나머지 49명의 환자는 복강경하 원위부 우회관 삽입술을 시행 받았다(Table 1). 대부분의 개복술은 2005년 8월에서 2006년 2월까지 시행 되어졌고, 그 이후에 는 복강경 술식이 시행 되었으며 평균 추적 관찰 기간은 18개월(6∼34개월)이었다.
1) 성별, 나이
전체 환자의 남녀 비는 1.10:1, 평균 나이는 53.70 (9∼
85) 이었으며, 우회술 실패에 관하여 두 군간에 유의한 차이 는 없었다.
2) 기저질환
고혈압, 당뇨, 만성신부전, 악성 신생물 과 기타 고지혈 증, 갑상선기능이상, 결핵 등이 이었으며, 수술전 기저질환 에 따라 우회술 실패 미치는 영향은 통계학적으로 유의 하 지 않았다.
3) 수술전 감염성 질환의 유무
수술전 감염성 질환이 있었던 환자는 전체환자 중 26명 이었는데, 주로 폐렴(19명), 뇌수막염(4명), 기타(1명)으로 조사 되었으나, 두 군간에 유의한 차이는 없었다.
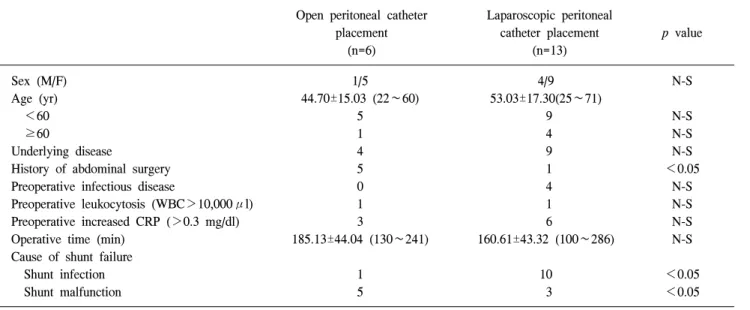
Table 2. Shunt failure
Open peritoneal catheter Laparoscopic peritoneal
placement catheter placement p value
(n=6) (n=13)
Sex (M/F) 1/5 4/9 N-S
Age (yr) 44.70±15.03 (22∼60) 53.03±17.30(25∼71)
<60 5 9 N-S
≥60 1 4 N-S
Underlying disease 4 9 N-S
History of abdominal surgery 5 1 <0.05
Preoperative infectious disease 0 4 N-S
Preoperative leukocytosis (WBC>10,000μl) 1 1 N-S
Preoperative increased CRP (>0.3 mg/dl) 3 6 N-S
Operative time (min) 185.13±44.04 (130∼241) 160.61±43.32 (100∼286) N-S
Cause of shunt failure
Shunt infection 1 10 <0.05
Shunt malfunction 5 3 <0.05
N-S = not significant.
4) 수술전 백혈구증 및 수술전 CRP상승
수술전 백혈구증이 있었던 환자는 전체 환자 중 9명, CRP 상승이 있었던 환자는 32명이었으나, 두 군간에 우회 술 실패 발생에 관하여는 통계학적 차이를 보이지 않았다.
5) 수술 시간
신경외과의 수술을 포함한 전체 수술 시간으로 평균 148 분(60∼298분)이 소요 되었다. 개복술을 시행했을 경우 평 균 163분(107∼298분)으로써 복강경을 이용한 원위부 우회 관 삽입 시 평균 138분(60∼286분) 보다 수술 시간이 긴 것 으로 조사되었으나 통계학적 차이는 없었으며, 우회관 감 염에 미치는 영향 또한 두 군간에 유의한 차이는 없었다.
6) 복부 수술 과거력
뇌실복막 우회술 시행 전 이미 복부 수술의 과거력이 있 었던 환자는 전체 환자 중 19명 이었으며, 복부 수술의 종류 로써 충수돌기절제술이 9명, 담낭절제술이 6명, 자궁절제술 2명, 기타 수술이 2명으로 조사되었다. 이중 6명(31%)에서 우회술 실패가 발생하였는데, 개복술 시 5명이 발생함으로 써 통계학적 유의성을 보였다(p=0.001).
7) 우회술 실패율
전체 환자 80명중 19명(23%)에서 우회술 실패가 발생하 였으며, 개복을 시행한 31명의 환자에서 6명(19.4%), 복강 경을 시행한 49명의 환자 중 13명(26.5%)에서 우회술 실패 가 발생하였다(Table 2).
8) 우회관 감염
복강경 술식은 2006년 3월 이후부터 활발히 시행 되어졌 는데, 두 군간에 유의한 차이는 없으나(p=0.462) 복강경 시 행 시 우회술 실패율이 높은 이유는 2007년 8월에서 11월 사이에 우회관 감염 8건이 집중적으로 발생하였기 때문이 다. 원내 감염관리팀의 조사 결과 대부분 피부상재균인 Coagulase negative Staphylococci (CNS)이 원인으로 밝혀져 의료진의 손 소독 및 환자의 피부소독 시 주의를 강조한 후 더 이상의 감염이 발생하지 않았다.
9) 우회술 실패의 원인
우회술 실패가 발생한 19명의 환자 중 우회관 감염에 의 한 우회술 실패 11명(57%), 우회관 기능이상에 의한 우회술 실패는 8명(43%)으로 조사되었으며, 복강경 술식 시 개복 술에 비해 원위부 우회관의 기능적 이상에 의한 우회술 실 패가 유의하게 감소하는 것으로 조사되었다(p=0.013).
고 찰
뇌실복막 우회술을 시행 시 우회관에 관련하여 발생할 수 있는 합병증은 성인에서 1년 안에 약 29% 정도로 보고 하고 있으며, 소아영역에서는 발생률이 더 높아 1개월이 내 에 14%, 1년 이내에 40∼50% 까지 생기는 것으로 알려져 있다.11 최근 조사된 California그룹에서는 우회관 합병증의 발생률을 5년 내 평균 32% (성인 27%, 소아 48%)인 것으로 발표하였다.12 합병증의 종류로는 우회관의 폐쇄, 꺽임 등으 로 인한 우회관 기능이상과 우회관 감염으로 인한 우회술
실패 등이 있다. 이러한 합병증 발생률을 줄이기 위해 염증 반응을 최소화한 새로운 소재의 우회관의 개발과 복 강경을 이용한 시야 확보를 통해 복강내 유착을 해결하거 나 피하는 등의 노력이 있어 왔다. 특히 모든 우회술 실패의 25∼30%가 윈위부 우회관의 기능적 이상에 의한 것으로 밝 혀지면서 복강내 우회관의 올바른 삽입 및 기능 유지의 중 요성이 대두 되었다.5,12-14 Rodgers 등15은 1978년에 소아 환 자에서 뇌실복막 우회관의 기능이상의 진단 및 교정을 위 해 처음으로 복강경을 적용하였으며, Guzinski 등16은 1982 년에 연결이 차단된 뇌실복막 우회관을 복강경으로 통하여 교정하여 보고하였다. 1990년대에 들어 복강내 원위부 우 회관 삽입에 복강경을 이용하려는 여러 시도 들이 있었는 데, 주로 합병증이 발생한 우회관의 제거 또는 교정에 적용 하고자 하는 경우 들이었다.17-20 1993년에 Armburster 등1 및 Basauri 등2을 비롯하여 1995년에 Cautico 등3, 1996년에 Box 등4이 복강경을 이용한 원위부 우회관 삽입술을 시행한 환 자들을 분석하여 좋은 결과를 발표하여 복강경 술식을 권 장 하였다. 1998년에는 Khosrovi 등5이 13명의 복강내 유착 이 있거나 또는 비만인 환자를 대상으로 이전에 전통적 술 식을 시행 받은 군과 일차적 복강경 적용 군에 대하여 복강 경을 통한 우회관 교정 및 일차적 우회관 삽입술을 시행하 여 비교 분석 하였는데, 두 군에서 모두 복강경의 적용이 성공적이었으며, 복강내 유착이 의심되거나 비만인 환자에 서는 일차적 복강경 술식을 추천하였다. 2005년 Schubert 등10 은 전향적 통제 연구(prospective controlled study)를 시행하 였는데 50명의 환자에게는 복강경을 통한 우회관 삽입을 시행하고 다른 50명의 대조군 에게는 전통적 우회관 삽입 술을 시행하여 비교 분석하였다. 두 군간에는 성별, 나이, ASA (American Society of Anesthesiologists) 점수, 수술 적응 증 및 과거 복부 수술의 빈도에 따라 유의한 차이를 보이지 않았으며, 평균 추적관찰 기간 18개월 동안 복강경군에서 는 우회술 실패가 3명(우회관 감염 1명, 우회관 기능이상 2명), 대조군 에서는 우회술 실패가 12명(우회관 감염 6명, 우회관 기능이상 6명)이 발생하였다. 통계학적 유의성 판단 (p<0.05)에 따라 복강경 술식에 의해 원위부 우회관 기능 이상에 의한 우회술 실패를 줄일 수 있다고 주장하였다.
2007년 Roth 등14이 발표한 후향적 연구에 따르면, 연구에 포함된 211명의 환자 중 복강경 술식이 시행되어진 59명의 환자에서 복부 수술의 과거력이 있는 경우 우회관 기능이 상에 의한 실패율이 유의 있게 감소하였다. 최근 들어 1개 의 투관침 만을 사용하거나 또는 카메라를 위한 투관침 만 을 가지고 우회관을 삽입하는 등 더욱 간편화되고 최소침 습적인 복강경 술기들을 보고하고 있다.21-24 본 연구에서는 복강경을 통한 우회관 삽입 시 카메라를 위한 port외에 1개 의 트로카 만을 이용하는 동일한 방법으로 시행하였으며, 복강내 유착이 심한 환자에서는 유착을 일부 제거한 후 우 회관을 삽입하였지만 모든 유착을 제거하지는 않았다. 신
경외과의 수술이 모두 끝난 후 참여 하였으며, 외과에서 진 행한 시간은 대부분 20분 미만이었다. 최근 보편화된 복강 경 충수돌기절제술을 능히 할 수 있는 수술자이면 특별한 기술적 어려움 없이 시행할 수 있었다. 초기에 급격히 발생 한 우회관 감염의 문제로 인해 본 연구의 가설에 입각한 결과의 도출이 어려워 보였지만 짧은 시간 내에 기본적 주 의 및 조정으로 해결되었으며 통계학적 유의성을 판단하는 데 무리가 없을 것으로 여겨진다.
결 론
뇌실복막 우회술 시행 시 복강경하 원위부 우회관 삽입 술을 통하여 수술자의 직접적 시야 하에 원위부 우회관을 정확한 위치에 삽입 할 수 있었으며, 우회관을 통한 뇌척수 액의 배액을 확인함으로써 개복을 통한 원위부 우회관 삽 입술 후 경험하는 비정상적 위치, 꺽임 및 대망과의 유착으 로 인한 막힘 등으로 발생하는 우회관 실패를 줄일 수 있었 다. 뇌실복막 우회술 시행 시 복강경하 원위부 우회관 삽입 술은 복강내 우회관의 기능적 측면에서 볼 때 매우 유용한 술식이며 또한 기술적으로 고도의 숙련도를 요하지 않기 때문에 습득 기간이 짧아 뇌실복막 우회술시 일차적 술식 으로써 유용할 것이다.
참고문헌
1) Armburster C, Blauensteiner J, Ammerer H, Kriwanek S.
Laparoscopically assisted implantation of ventriculoperitoneal shunts. J Laparoendosc Surg 1993;3:191-192.
2) Basauri L, Selman JM, Lizana C. Peritoneal catheter insertion using laparoscopic guidance. Pediatr Neurosurg 1993;19:
109-110.
3) Cautico W, Vannix D. Laparoscopically guided peritoneal insertion in ventriculoperitoneal shunts. J Laparoendosc Surg 1995;5:309-311.
4) Box JC, Young D, Mason E, et al. A retrospective analysis of laparoscopically assisted ventriculoperitoneal shunts. Surg Endosc 1996;10:311-313.
5) Khosrovi H, Kaufman HH, Hrabovsky E, Bloomfield SM, Prabhu V, El-Kadi HA. Laparoscopic-assisted distal ventri- culoperitoneal shunt placement. Surg Neurol 1998;49:127-135.
6) Reimer R, Wharen RE Jr, Pettit PDM. Ventriculoperitoneal shunt placement with video-laparoscopic guidance. J Am Coll Surg 1998;187:637-639.
7) Khaitan L, Brennan EJ Jr. A laparoscopic approach to ventriculoperitoneal shunt placement in adults. Surg Endosc 1999;13:1007-1009.
8) Kubo S, Nakata H, Yoshimine T. Peritoneal shunt tube placement performed using an endoscopic threaded imaging port. J Neurosurg 2001;94:677-679.
9) Kirshtein B, Benifla M, Roy-Shapira A, et al. Laparoscopically guided distal ventriculoperitoneal shunt placement. Surg Laparosc Endosc Percutan Tech 2004;14:276-278.
10) Schubert F, Fijen BP, Krauss JK. Laparoscopically assisted peritoneal shunt insertion in hydrocephalus. Surg Endosc 2005;19:1588-1591.
11) Bryant MS, Bremer AM, Tepas JJ, Mollitt DL, Nquyen TZ, Talber JL. Abdominal complications of ventriculoperitoneal shunts. Am Surg 1988;54:50-55.
12) Wu Y, Green NL, Wrensch MR, Zhao S, Gupta N.
Ventriculoperitoneal shunt complications in california: 1999 to 2000. Neurosurg 2007;61:557-563.
13) Kestle J, Drake J, Milner R, et al. Long-term follow-up data from the shunt design trial. Pediatr Neurosurg 2000;33:
230-236.
14) Roth J, Sagie B, Szold A, Elran H. Laparoscopic versus non-laparoscopic-assisted ventriculoperitoneal shunt placement in adults. Surg Neurol 2007;68:177-184.
15) Rodgers BM, Vries JK, Talbert JL. Laparoscopy in the diagnosis and treatment of malfunctioning ventriculoperitoneal shunts in children. J Pediatr Surg 1978;13:247-253.
16) Guzinski GM, Meyer WJ, Loser JD. Laparoscopic retrieval of disconnected ventriculoperitoneal shunt catheters. J Neurosurg 1982;56:587-589.
17) Schrenk P, Woisetschlager R, Wayand WU, Polanski P.
Laparoscopic removal of dislocated ventriculoperitoneal shunts.
Report of two cases. Surg Endosc 1994;8:1113-1114.
18) Tanaka J, Kikuchi K, Sasajima H, Koyama K. Laparoscopic retrieval of disconnected ventriculoperitoneal shunt catheters:
report of two cases. Surg Laparosc Endosc 1995;5:263-266.
19) Esposito C, Porreca A, Gangemi M, Garipoli V, De Pasquale M. The use of laparoscopy in the diagnosis and treatment of abdominal complications of ventriculoperitoneal shunts in children. Pediatr Surg Int 1998;13:352-354.
20) Kusano T, Miyazato H, Shimoji H, et al. Revision of ventriculoperitoneal shunt under laparoscopic guidance in patients with hydrocephalus. Surg Laparosc Endosc 1998;
8:474-476.
21) Fanelli RD, Mellinger DN, Crowell RM, Gersin KS. Laparoscopic ventriculoperitoneal shunt placement: a single-trocar technique.
Surg Endosc 2000;14:641-643.
22) Reardon PR, Scarborough TK, Matthews BD, Marti JL, Preciado A. Laparoscopically assisted ventriculoperitoneal shunt placement using 2-mm instrumentation. Surg Endosc 2000;14:585-586.
23) Turner RD, Rosenblatt SM, Chand B, Luciano MG.
Laparoscopic peritoneal catheter placement: result of a new method in 111 patients. Neurosurg 2007;61:167-174.
24) Konstantinidis H, Balogiannis I, Foroglu N, et al. Laparoscopic placement of ventriculoperitoneal shunts: An innovative simplification of the existing techniques. Minim Invas Neurosurg 2007;50:62-64.