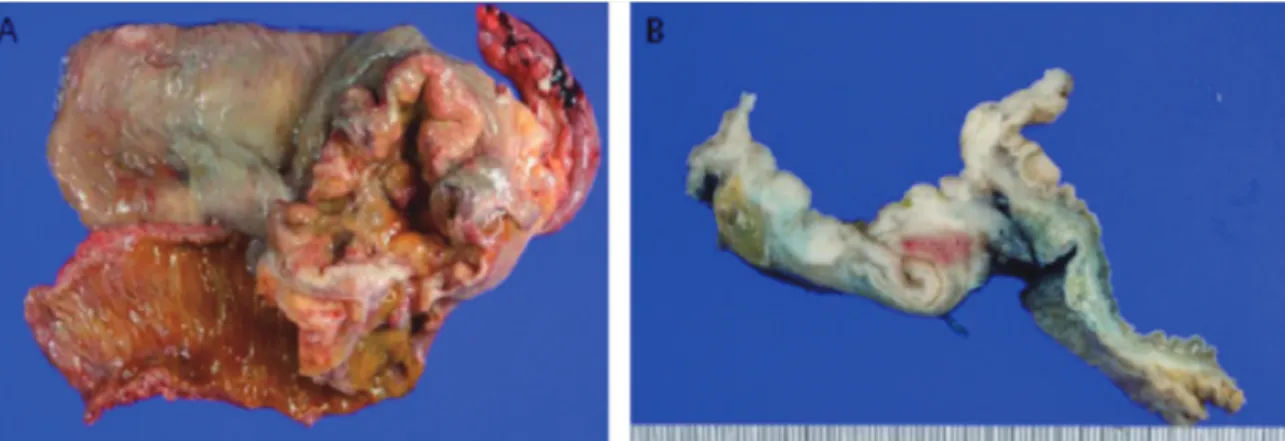
Primary Signet-ring Cell Carcinoma of the Cecum
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
• 이명의 치료에 대한 매커니즘과 디지털 음향 기술에 대한 상업적으로의 급속한 발전으로 인해 치료 옵션은 증가했 지만, 선택 가이드 라인은 거의 없음.. •
The proposal of the cell theory as the birth of contemporary cell biology Microscopic studies of plant tissues by Schleiden and of animal tissues by Microscopic studies of
diffuse large cell lymphoma with positive marrow biopsy Gallium scan (SPECT) or PET scan in large-cell lymphoma.. Stage
웹 표준을 지원하는 플랫폼에서 큰 수정없이 실행 가능함 패키징을 통해 다양한 기기를 위한 앱을 작성할 수 있음 네이티브 앱과
_____ culture appears to be attractive (도시의) to the
편평상피세포암(squamous cell carcinoma), 선암(adenocarcinoma) 그리고 대세 포암(large cell carcinoma)으로 나뉘고 그에 따라 치료제가 조금씩
After first field tests, we expect electric passenger drones or eVTOL aircraft (short for electric vertical take-off and landing) to start providing commercial mobility
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
