Risk Factors for Mortality in Patients with Carbapenem-Resistant Acinetobacter baumannii Bacteremia: Impact of Appropriate Antimicrobial Therapy
This study investigated predictors associated with 14-day mortality, and focused especially on the impact of appropriate antimicrobial treatment among patients with carbapenem- resistant Acinetobacter baumannii (CRAB) bacteremia. This retrospective study was performed at a tertiary care hospital in Korea from June 2007 to June 2010. Antibiotic therapy was considered appropriate if the antibiotics were administered via an appropriate route within 24 hr after the result of blood culture, had in vitro sensitivity to isolated strains, and of an adequate dosage according to the current guidelines. Ninety-five patients with A. baumannii bacteremia were included; of these, 53 (55.8%) were infected with CRAB.
The overall infection-related 14-day mortality was higher in patients receiving inappropriate antimicrobial therapy than in patients receiving appropriate therapy (59.5% [22/37] vs 13.8% [8/58], P < 0.05). Multivariate analysis showed that septic shock (OR 10.5, 95% CI, 1.93-57.4; P = 0.006), carbapenem-resistance (OR 7.29, 95% CI 1.57-33.8; P = 0.01), pneumonia as a source of bacteremia (OR 5.29, 95% CI 1.07-26.1; P = 0.04), and inappropriate antimicrobial therapy (OR 8.05, 95% CI 1.65-39.2; P = 0.009) were independent risk factors for 14-day mortality. Early definite antimicrobial therapy had an influence on favorable outcomes in patients with A. baumannii bacteremia.
Key Words: Acinetobacter baumannii; Risk Factors; Carbapenem-Resistance; Mortality Youn Jeong Kim1, Sang Il Kim1,
Kyung-Wook Hong1, Yang Ree Kim1, Yeon Joon Park2, and Moon-Won Kang1 Departments of 1Internal Medicine and 2Laboratory Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea
Received: 1 August 2011 Accepted: 27 January 2012 Address for Correspondence:
Yang Ree Kim, MD
Department of Internal Medicine, Uijeongbu St. Mary’s Hospital, The Catholic University of Korea College of Medicine, 271 Cheonbo-ro, Uijeongbu 480-717, Korea Tel: +82.31-820-3798, Fax: +82.31-847-2719 E-mail: [email protected]
http://dx.doi.org/10.3346/jkms.2012.27.5.471 • J Korean Med Sci 2012; 27: 471-475 Infectious Diseases, Microbiology & Parasitology
INTRODUCTION
Acinetobacter baumannii is an important nosocomial pathogen (1-6). Carbapenem is a preferred drug of choice for the treat- ment of multidrug-resistant A. baumannii. However, carbape- nem-resistant strains have now emerged around the world (2).
Prevalence of carbapenem-resistant A. baumannii varies in dif- ferent countries; in Korea, the resistance rate of A. baumannii against carbapenem was reported as 31.7% or 34.9% (7).
A. baumannii may cause various clinical manifestations rang- ing from colonization to septic shock, and A. baumannii bacte- remia-associated mortality rate is reported to be as high as 17%- 62% (8-10). Initiation of effective empirical antimicrobial treat- ment might be important for reducing A. baumannii bactere- mia-associated mortality. However, in Korea, initiation of broad spectrum antibiotic treatment with antibiotics such as carbap- enem or colistin is difficult because of insurance problems (11, 12). Because the severity of underlying disease could affect the outcomes in patients with A. baumannii bacteremia, it is not yet clear whether immediate and appropriate antimicrobial ther- apy as proper dose and administration route can affect these outcomes (12, 13). Because of the presence of limited therapeu-
tic options for carbapenem-resistant A. baumannii (CRAB), it is important to understand the factors responsible for the devel- opment of carbapenem-resistance and the risk factors associ- ated with mortality. In this study, we investigated the factors associated with acquisition of CRAB in patients with A. bau- mannii bacteremia; and the predictors associated with 14-day mortality. Our study especially focused on the impact of early and appropriate antimicrobial treatment after obtaining culture results.
MATERIALS AND METHODS Study design
A retrospective study was performed from June 2007 to June 2010 at a tertiary care hospital with 1,200 beds in Korea. All pa- tients over 16-yr old from whom A. baumannii was isolated from at least one set of blood cultures with definite clinical signs of infection were enrolled. Only the first bacteremic episode from each patient was included in this study. Antibiotic therapy was considered appropriate if the antibiotics administered via an appropriate route within 24 hr of blood culture results showed an in vitro effectiveness against isolated strains, and if the dos-
age was adequate according to the current guidelines. Infection was assessed according to “Centers for Disease Control and Pre- vention” criteria, and patients were considered infected when A. baumannii was isolated from a sterile site in patients with definite clinical signs of infection (14). Prior antibiotics treat- ment was defined as the use of systemic antibiotics for at least 7 days within the preceding 28 days. For better understanding of the patients’ baseline status, we assessed the APACHE II score before bacteremia on the date of admission. We used 14-day in- hospital mortality as the main outcome for assessment of mor- tality for patients with serious conditions due to bacteremia.
Microbiological examination
Identification of A. baumannii in blood samples was performed using a VITEKR2 automated system (bioMérieux, Marcy l’Etoile, France). Susceptibility results were interpreted according to guidelines established by the Clinical and Laboratory Standards Institute (15). CRAB was defined as non-susceptible to merope- nem and/or imipenem in vitro, and isolates with intermediate resistance were regarded as resistance.
Statistically analysis
Student’s t-test was used for analysis of continuous variables, and the chi-squared test or Fisher’s exact test was used for cate- gorical variables and Student’s t test or the Mann-Whitney U test for continuous variables. We analyzed the risk factors asso- ciated with mortality using univariate and multivariate logistic regression analyses. Survival curves were prepared using the Kaplan-Meier method with log-rank test. Statistical analysis was performed using SPSS 13.0 and a P value < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the institutional review board of Seoul St. Mary’s Hospital (Protocol No; KC10OISI0070). Informed consent was waived by the board. All the data collected during this study were kept confidential.
RESULTS
A total of 95 patients with A. baumannii bacteremia were in- cluded in this study. Demographic characteristics of these pa-
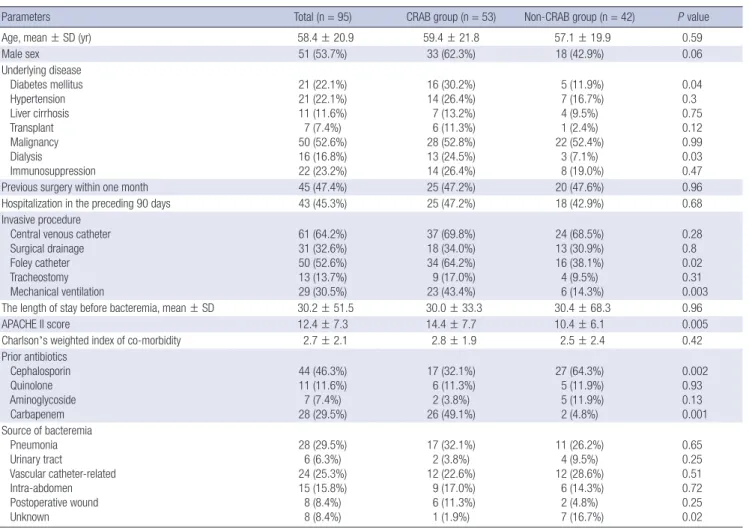
Table 1. Clinical characteristics of patients with Acinetobacter baumannii bacteremia
Parameters Total (n = 95) CRAB group (n = 53) Non-CRAB group (n = 42) P value
Age, mean ± SD (yr) 58.4 ± 20.9 59.4 ± 21.8 57.1 ± 19.9 0.59
Male sex 51 (53.7%) 33 (62.3%) 18 (42.9%) 0.06
Underlying disease Diabetes mellitus Hypertension Liver cirrhosis Transplant Malignancy Dialysis
Immunosuppression
21 (22.1%) 21 (22.1%) 11 (11.6%) 7 (7.4%) 50 (52.6%) 16 (16.8%) 22 (23.2%)
16 (30.2%) 14 (26.4%) 7 (13.2%) 6 (11.3%) 28 (52.8%) 13 (24.5%) 14 (26.4%)
5 (11.9%) 7 (16.7%) 4 (9.5%) 1 (2.4%) 22 (52.4%)
3 (7.1%) 8 (19.0%)
0.04 0.3 0.75 0.12 0.99 0.03 0.47
Previous surgery within one month 45 (47.4%) 25 (47.2%) 20 (47.6%) 0.96
Hospitalization in the preceding 90 days 43 (45.3%) 25 (47.2%) 18 (42.9%) 0.68
Invasive procedure Central venous catheter Surgical drainage Foley catheter Tracheostomy Mechanical ventilation
61 (64.2%) 31 (32.6%) 50 (52.6%) 13 (13.7%) 29 (30.5%)
37 (69.8%) 18 (34.0%) 34 (64.2%) 9 (17.0%) 23 (43.4%)
24 (68.5%) 13 (30.9%) 16 (38.1%) 4 (9.5%) 6 (14.3%)
0.28 0.8 0.02 0.31 0.003
The length of stay before bacteremia, mean ± SD 30.2 ± 51.5 30.0 ± 33.3 30.4 ± 68.3 0.96
APACHE II score 12.4 ± 7.3 14.4 ± 7.7 10.4 ± 6.1 0.005
Charlson’s weighted index of co-morbidity 2.7 ± 2.1 2.8 ± 1.9 2.5 ± 2.4 0.42
Prior antibiotics Cephalosporin Quinolone Aminoglycoside Carbapenem
44 (46.3%) 11 (11.6%) 7 (7.4%) 28 (29.5%)
17 (32.1%) 6 (11.3%) 2 (3.8%) 26 (49.1%)
27 (64.3%) 5 (11.9%) 5 (11.9%) 2 (4.8%)
0.002 0.93 0.13 0.001 Source of bacteremia
Pneumonia Urinary tract
Vascular catheter-related Intra-abdomen Postoperative wound Unknown
28 (29.5%) 6 (6.3%) 24 (25.3%) 15 (15.8%) 8 (8.4%) 8 (8.4%)
17 (32.1%)
2 (3.8%) 12 (22.6%) 9 (17.0%) 6 (11.3%) 1 (1.9%)
11 (26.2%) 4 (9.5%) 12 (28.6%) 6 (14.3%) 2 (4.8%) 7 (16.7%)
0.65 0.25 0.51 0.72 0.25 0.02 CRAB, carbapenem-resistant Acinetobacter baumannii.
tients are shown in Table 1. The mean age of the patients was 58.4 ± 20.9 yr, and of the 95 patients, 53.7% were male. The mean length of stay before A. baumannii bacteremia was 30.2 ± 51.5 days. The presumed sources of bacteremia were respiratory tract (n = 28, 29.5%), vascular catheter (n = 24, 25.3%), intra-abdomen (n = 15, 15.8%), postoperative wounds (n = 8, 8.4%), urinary tract (n = 6, 6.3%), and other unknown sources (n = 8, 8.4%).
Fifty-three patients (55.8%) were infected with CRAB. Univar- iate analysis showed that the risk factors for acquisition of CRAB bacteremia were diabetes mellitus (OR 3.2, 95% CI 1.06-9.64;
P = 0.04), dialysis (OR 4.23, 95% CI 1.11-15.9; P = 0.03) as an un- derlying disease, use of foley catheter (OR 2.91, 95% CI 1.26-6.73;
P = 0.01), mechanical ventilation support (OR 4.6, 95% CI 1.66- 12.77; P = 0.003), and prior use of cephalosporin (OR 3.81, 95%
CI 1.62-8.96; P = 0.002) or carbapenem (OR 19.3, 95% CI 4.21- 87.9; P = 0.001). By multivariate analysis, diabetes mellitus as an underlying disease (OR 4.51, 95% CI 1.16-14.8; P = 0.03) and prior use of carbapenem (OR 14.8, 95% CI 2.76-79.5; P = 0.002) were independently associated with CRAB bacteremia (Table 2).
The overall infection-related 14-day mortality in patients with A. baumannii bacteremia was 31.6% (30/95); infection-related 14-day mortality was higher in patients receiving inappropriate antimicrobial therapy than in patients receiving appropriate therapy (59.5% [22/37] vs 13.8% [8/58], P < 0.05). The cumula- tive survival curves of the patients according to the appropriate- ness of antimicrobial therapy are shown in Fig. 1. Univariate anal- ysis showed that the risk factors for infection-related 14-day mor-
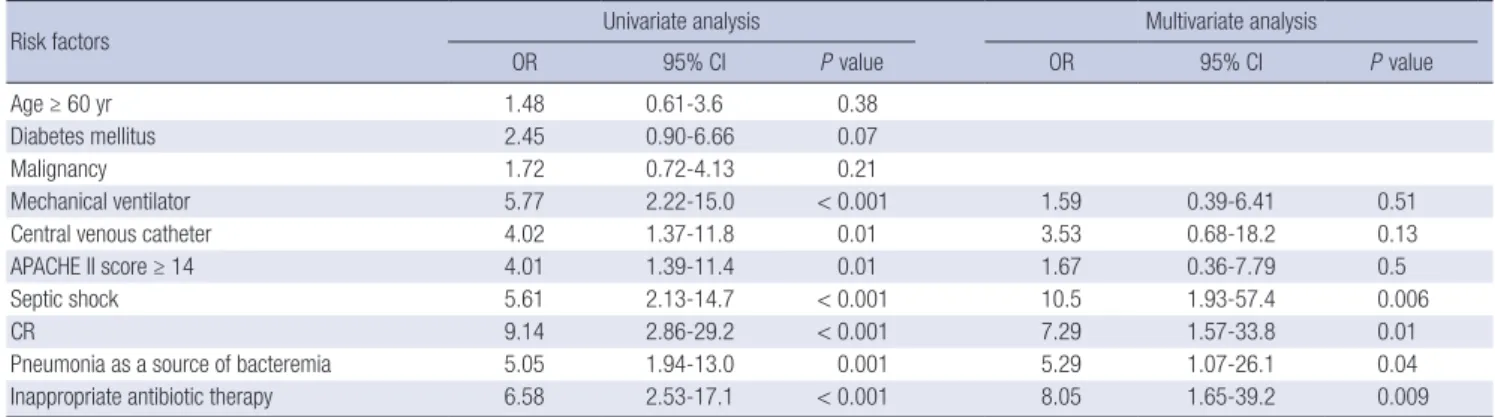
tality in patients with A. baumannii bacteremia were central venous catheter (OR 4.02, 95% CI 1.37-11.83; P = 0.01), mechan- ical ventilatoin (OR 5.77, 95% CI 2.22-15.02; P < 0.001), high APACHE II score (OR 4.01, 95% CI 1.39-11.4; P = 0.01), septic shock (OR 5.61, 95% CI 2.13-14.7; P < 0.001), carbapenem-resis- tance (OR 9.14, 95% CI 2.86-29.2; P < 0.001), pneumonia as a source of bacteremia (OR 5.05, 95% CI 1.94-13.0; P < 0.001), and inappropriate antibiotic therapy (OR 6.58, 95% CI 2.53-17.1; P <
0.001) (Table 3). Multivariate analysis showed that septic shock (OR 10.5, 95% CI 1.93-57.4; P = 0.006), carbapenem-resistance
Table 2. Risk factors for acquisition of carbapenem resistant Acinetobacter baumannii bacteremia
Risk factors Univariate analysis Multivariate analysis
OR 95% CI P value OR 95% CI P value
Age, mean ± SD 1.0 0.99-1.02 0.59
Male sex 2.2 0.96-5.02 0.06
Underlying disease Diabetes mellitus Hypertension Liver cirrhosis Transplant Malignancy Dialysis
Immunosuppression
3.2 1.79 1.44 5.23 1.01 4.23 1.53
1.06-9.64 0.65-4.95 0.39-5.31 0.61-45.3 0.45-2.29 1.11-15.9 0.57-4.10
0.04 0.3 0.56 0.12 0.95 0.03 0.40
4.51
1.48
1.16-14.8
0.27-7.7
0.03
0.66
Previous surgery within one month 1.01 0.45-2.29 0.96
Hospitalization in the preceding 90 days 1.19 0.52-2.69 0.68
Invasive procedure Central venous catheter Surgical drainage Foley catheter Tracheostomy Mechanical ventilation
1.74 1.14 2.91 1.94 4.6
0.74-4.10 0.48-2.73 1.26-6.73 0.54-6.81 1.66-12.77
0.21 0.76 0.01 0.31 0.003
2.51 2.75
0.89-7.59 0.77-9.62
0.08 0.12
The length of stay before bacteremia, mean ± SD 1 0.99-1.00 0.96
Prior antibiotics Cephalosporin Quinolone Aminoglycoside Carbapenem
3.81 1.05 3.44 19.3
1.62-8.96 0.29-3.74 0.63-18.7 4.21-87.9
0.002 0.93 0.15 0.001
1.85 14.8
0.61-5.61 2.76-79.5
0.27
0.002 CRAB, carbapenem-resistant Acinetobacter baumannii.
Fig. 1. Survival curve according to the appropriateness of antimicrobial therapy.
Cumulative survival
Days from onset of bacteremia
P < 0.05
Appropriate antimicrobial therapy Inappropriate antimicrobial therapy
0.00 2.00 4.00 6.00 8.00 10.00 12.00 14.00 1.0
0.8 0.6 0.4 0.2 0.0
(OR 7.29, 95% CI 1.57-33.8; P = 0.01), pneumonia as a source of bacteremia (OR 5.29, 95% CI 1.07-26.1; P = 0.04), and inappro- priate antimicrobial therapy (OR 8.05, 95% CI 1.65-39.2; P = 0.009) were the independent risk factors for 14-day mortality (Table 3).
In sub-analysis of the CRAB group, patients receiving inappro- priate antimicrobial therapy showed a higher mortality than those receiving appropriate therapy (67.9% [19/28] vs 28.0% [7/
25], P = 0.004). In the non-CRAB group, 33 patients received appropriate therapy and 97% of the patients had survived for 14 days after the onset of bacteremia.
DISCUSSION
A. baumannii is usually a healthcare-associated pathogen and is emerging as a cause of numerous global outbreaks (1, 2). An- timicrobial resistance recently has emerged as an important problem. Carbapenem is widely used for the treatment of mul- tidrug-resistant A. baumannii infections, however, reports of CRAB are also increasing worldwide.
Previous studies have showed that factors associated with mor- tality in patients with A. baumannii infection are septic shock, age, severity of the underlying disease, and mechanical ventila- tion (16-18). Delay in receiving empirical antimicrobial therapy has an adverse effect on clinical outcomes, however, some stud- ies have shown that severity of illness is a more important factor for mortality than empirical therapy in hospital-acquired pneu- monia caused by A. baumannii (12, 19). Moreover, in Korea, use of broad spectrum antibiotics prior to the isolation of multidrug- resistant strains is limited.
Our study revealed that independent risk factors associated with 14-day mortality in patients with A. baumannii bacteremia included septic shock, carbapenem-resistance, pneumonia as a source of bacteremia and inappropriate antibiotic therapy. This study evaluated the clinical outcomes in patients with A. bau- mannii bacteremia according to the inappropriateness of anti- biotics (i.e., antibiotics that were not active in vitro and those that were administered as an improper dose or through an im-
proper route) after obtaining the blood culture results. Our data suggest that early administration of appropriate antimicrobial therapy showed improved outcomes in patients with CRAB bacteremia, although underlying status played an important role in clinical outcome.
Studies have shown that APACHE II score is useful for the es- timation of prognosis in Acinetobacter pneumonia (19, 20). In our study, a high APACHE II score was associated with mortali- ty by univariate analysis; however this was not identified as an independent risk factor by multivariate analysis. This may be because of several reasons. First, some information, such as that on sepsis and mechanical ventilation, was not included while determining this score. Second, we assessed the APACHE II score before the occurrence of bacteremia on the date of admission, in order to best reflect the patients’ baseline status. Our study also showed that septic shock at the time of bacteremia was an independent risk factor for mortality. This finding suggested that a combination of other parameters, including the APACHE II score, is necessary for the evaluation of morbidity in patients with bacteremia.
The effect of antibiotic resistance on mortality is controversial.
Some studies have reported that antibiotic resistance has an ad- verse impact on the mortality rates in patients with A. baumannii bacteremia (1, 21). One study reported that mortality in patients with multidrug-resistant A. baumannii infection in surgical in- tensive care units did not differ significantly from that in patients with non-multidrug-resistant A. baumannii infection. However, the study did not include patients who were simply bacteremic (6). Our results showed that carbapenem resistance was inde- pendently associated with mortality. However, patients with CRAB bacteremia had a higher APACHE II score (14.4 ± 7.7 vs 10.4 ± 6.1, P = 0.005) and received a more inappropriate antibi- otic treatment (52.8% [28/53] vs 21.4% [9/42], P = 0.002) than those with non-CRAB bacteremia. CRAB bacteremia usually occurs in patients with severe illness and in patients with a high probability of receiving inappropriate antimicrobial therapy, which then negatively affect the outcomes.
Table 3. Risk factors associated with 14-day mortality in patients with Acinetobacter baumannii bacteremia
Risk factors Univariate analysis Multivariate analysis
OR 95% CI P value OR 95% CI P value
Age ≥ 60 yr 1.48 0.61-3.6 0.38
Diabetes mellitus 2.45 0.90-6.66 0.07
Malignancy 1.72 0.72-4.13 0.21
Mechanical ventilator 5.77 2.22-15.0 < 0.001 1.59 0.39-6.41 0.51
Central venous catheter 4.02 1.37-11.8 0.01 3.53 0.68-18.2 0.13
APACHE II score ≥ 14 4.01 1.39-11.4 0.01 1.67 0.36-7.79 0.5
Septic shock 5.61 2.13-14.7 < 0.001 10.5 1.93-57.4 0.006
CR 9.14 2.86-29.2 < 0.001 7.29 1.57-33.8 0.01
Pneumonia as a source of bacteremia 5.05 1.94-13.0 0.001 5.29 1.07-26.1 0.04
Inappropriate antibiotic therapy 6.58 2.53-17.1 < 0.001 8.05 1.65-39.2 0.009
OR, odds ratio; CI, confidential interval; CR, carbapenem-resistance.
Results from the present study also showed that factors for acquisition of CRAB included diabetes mellitus as an underlying disease and a prior exposure to carbapenem. Some studies have reported that prior use of carbapenem, third-generation cepha- losporins and fluoroquinolones are independent risk factors for the acquisition of multidrug resistant A. baumannii (22, 23).
Selective pressure exerted by use of broad spectrum antibiotics, such as carbapenem, leads to the emergence of multidrug-resis- tant A. baumannii. Therefore, we consider multidrug resistance in patients with A. baumannii bacteremia who showed particu- larly severe illness, and who had recently received carbapenem.
In order to decrease acquisition of CRAB, judicious use of car- bapenem is important.
Our study had some limitations, including the retrospective design, which was not randomized. A small number of patients were enrolled from a single center. Furthermore, we could not judge the appropriateness of the empirical antibiotic treatment in this study. It was rare that patients with CRAB bacteremia re- ceived colistin empirically, because of insurance or restriction of broad spectrum antibiotics for policy of antibiotics control.
However, our study should encourage clinicians not to delay definite antimicrobial treatment in patients with A. baumannii bacteremia.
In conclusion, patients with A. baumannii bacteremia receiv- ing early and appropriate antimicrobial therapy are expected to show favorable outcomes, although the status of underlying dis- ease also plays an important role in the clinical outcomes.
REFERENCES
1. Perez F, Hujer AM, Hujer KM, Decker BK, Rather PN, Bonomo RA.
Global challenge of multidrug-resistant Acinetobacter baumannii. Anti- microb Agents Chemother 2007; 51: 3471-84.
2. Dijkshoorn L, Nemec A, Seifert H. An increasing threat in hospitals: mul- tidrug-resistant Acinetobacter baumannii. Nat Rev Microbiol 2007; 5:
939-51.
3. Ayan M, Durmaz R, Aktas E, Durmaz B. Bacteriological, clinical and ep- idemiological characteristics of hospital-acquired Acinetobacter bau- mannii infection in a teaching hospital. J Hosp Infect 2003; 54: 39-45.
4. Paul M, Weinberger M, Siegman-Igra Y, Lazarovitch T, Ostfeld I, Boldur I, Samra Z, Shula H, Carmeli Y, Rubinovitch B, et al. Acinetobacter bau- mannii: emergence and spread in Israeli hospitals 1997-2002. J Hosp In- fect 2005; 60: 256-60.
5. Navon-Venezia S, Ben-Ami R, Carmeli Y. Update on Pseudomonas ae- ruginosa and Acinetobacter baumannii infections in the healthcare set- ting. Curr Opin Infect Dis 2005; 18: 306-13.
6. Daniels TL, Deppen S, Arbogast PG, Griffin MR, Schaffner W, Talbot TR. Mortality rates associated with multidrug-resistant Acinetobacter baumannii infection in surgical intensive care units. Infect Control Hosp Epidemiol 2008; 29: 1080-3.
7. Park YK, Peck KR, Cheong HS, Chung DR, Song JH, Ko KS. Extreme drug resistance in Acinetobacter baumannii infections in intensive care units, South Korea. Emerg Infect Dis 2009; 15: 1325-7.
8. Robenshtok E, Paul M, Leibovici L, Fraser A, Pitlik S, Ostfeld I, Samra Z, Perez S, Lev B, Weinberger M. The significance of Acinetobacter bauman- nii bacteraemia compared with Klebsiella pneumoniae bacteraemia:
risk factors and outcomes. J Hosp Infect 2006; 64: 282-7.
9. Jerassy Z, Yinnon AM, Mazouz-Cohen S, Benenson S, Schlesinger Y, Rudensky B, Raveh D. Prospective hospital-wide studies of 505 patients with nosocomial bacteraemia in 1997 and 2002. J Hosp Infect 2006; 62:
230-6.
10. Grupper M, Sprecher H, Mashiach T, Finkelstein R. Attributable mor- tality of nosocomial Acinetobacter bacteremia. Infect Control Hosp Epi- demiol 2007; 28: 293-8.
11. Harbarth S, Garbino J, Pugin J, Romand JA, Lew D, Pittet D. Inappropri- ate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med 2003;
115: 529-35.
12. Erbay A, Idil A, Gözel MG, Mumcuoˇglu I, Balaban N. Impact of early ap- propriate antimicrobial therapy on survival in Acinetobacter bauman- nii bloodstream infections. Int J Antimicrob Agents 2009; 34: 575-9.
13. Lim SK, Lee SO, Choi SH, Choi JP, Kim SH, Jeong JY, Choi SH, Woo JH, Kim YS. The outcomes of using colistin for treating multidrug resistant Acinetobacter species bloodstream infections. J Korean Med Sci 2011; 26:
325-31.
14. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions for nosocomial infections, 1988. Am J Infect Control 1988; 16: 128-40.
15. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing Informational Supplement M100- S16. Wayne: Clinical and Laboratory Standards Institute, 2008.
16. Choi JY, Park YS, Kim CO, Yoon HJ, Shin SY, Kim YA, Song YG, Yong D, Lee K, Kim JM. Mortality risk factors of Acinetobacter baumannii bacte- raemia. Intern Med J 2005; 35: 599-603.
17. Tilley PA, Roberts FJ. Bacteremia with Acinetobacter species: risk fac- tors and prognosis in different clinical settings. Clin Infect Dis 1994; 18:
896-900.
18. Chen HP, Chen TL, Lai CH, Fung CP, Wong WW, Yu KW, Liu CY. Predic- tors of mortality in Acinetobacter baumannii bacteremia. J Microbiol Immunol Infect 2005; 38: 127-36.
19. Joung MK, Kwon KT, Kang CI, Cheong HS, Rhee JY, Jung DS, Chung SM, Lee JA, Moon SY, Ko KS, et al. Impact of inappropriate antimicrobi- al therapy on outcome in patients with hospital-acquired pneumonia caused by Acinetobacter baumannii. J Infect 2010; 61: 212-8.
20. Garnacho-Montero J, Ortiz-Leyba C, Fernández-Hinojosa E, Aldabó- Pallás T, Cayuela A, Marquez-Vácaro JA, Garcia-Curiel A, Jiménez-Jimé- nez FJ. Acinetobacter baumannii ventilator-associated pneumonia: epi- demiological and clinical findings. Intensive Care Med 2005; 31: 649-55.
21. Kwon KT, Oh WS, Song JH, Chang HH, Jung SI, Kim SW, Ryu SY, Heo ST, Jung DS, Rhee JY, et al. Impact of imipenem resistance on mortality in patients with Acinetobacter bacteraemia. J Antimicrob Chemother 2007;
59: 525-30.
22. Ye JJ, Huang CT, Shie SS, Huang PY, Su LH, Chiu CH, Leu HS, Chiang PC.
Multidrug resistant Acinetobacter baumannii: risk factors for appear- ance of imipenem resistant strains on patients formerly with susceptible strains. PLoS One 2010; 5: e9947.
23. Falagas ME, Kopterides P. Risk factors for the isolation of multi-drug- resistant Acinetobacter baumannii and Pseudomonas aeruginosa: a systematic review of the literature. J Hosp Infect 2006; 64: 7-15.