접수일: 2008년 8월 18일, 게재승인일: 2008년 9월 12일
책임저자: 정선근, 서울시 종로구 연건동 28번지
110-744, 서울대학교병원 재활의학과
Tel: 02-2072-5203, Fax: 02-743-7473 E-mail: suncg@snu.ac.kr
비-회전근개 견관절 질환에 대한 초음파 소견
서울대학교 의과대학 재활의학교실
정 선 근
Sonographic Fidings of Shoulders with Non-rotator Cuff Diseases
Sun-Gun Chung, M.D., Ph.D.
Department of Rehabilitation Medicine, Seoul National Univer- sity College of Medicine, Seoul, Korea
The development of high resolution ultrasonographic techni- que made it possible to investigate a variety of muscu- loskeletal diseases using ultrasound. Shoulder pain is one of the most frequently examined musculoskeletal disorders by ultrasonography. It is because sonography has a strong diagnostic power for rotator cuff tendon problems, which are very common causes of the shoulder pain. For this rea- son, many sonographers pay much attention to the rotator cuff tendon disorders, while the importance of the non-rota- tor cuff lesions in shoulder sonography is less appreciated.
However, it would be impossible to make an accurate diag- nosis of shoulder disorders if one does not have a compre- hensive and thorough knowledge and experience on both rotator cuff and non-rotator cuff lesions, because many cas- es of shoulder pain are caused by non-rotator cuff lesions and sometimes they are closely associated with rotator cuff lesions. This review includes pictorial descriptions of the so- nographic findings of non-rotator cuff pathologies. (J Korean Assoc Pain Med 2008;7:70-85)
Key Words: Sonography, Shoulder, Non-rotator cuff
서 론
전기-전자 기술의 발달로 천부 조직에 대한 고해상도의 초음파 영상의 획득이 가능해진 이래 근골격계 질환에 대 한 초음파의 임상적 이용은 급격히 늘어가고 있다. 근골격 계 초음파 진단이 가장 흔히 적용되는 구조물은 단연 견관 절을 꼽을 수 있는데 그 이유로는 빈도상으로나 기능적으
로나 견관절에 가장 중요한 질환인 회전근개 질환에 대해 초음파 검사의 진단적 가치가 매우 높기1) 때문으로 볼 수 있다. 이에 비해 비-회전근개 질환(non-rotator cuff dis- eases)에 대한 초음파의 진단력은 자기공명영상검사에 비 해 비교적 낮으며2) 따라서 임상적 적용 빈도도 낮은 것이 사실이다.3) 그러나 회전근개 질환과 비-회전근개 질환이 하나의 견관절속에서 동시에 발견되는 경우가 많고 하나의 병변이 시간이 흐름에 따라 다른 병변을 유발하기도 하는 이유로 견관절 초음파 검사때 회전근개 질환만 평가를 한 다는 것은 실제적으로 불가능한 일이다. 견관절의 3차원 해 부학을 숙지하고 검사하려는 견관절의 자세를 정확히 잡아 탐색자를 적절히 위치하여 검사하면 견관절 통증의 원인이 되는 비-회전근개 질환들의 소견에 차츰 익숙해진다. 이러 한 과정을 통하여 충분한 경험을 쌓으면 비-회전근개 질환 들에 대한 진단에 초음파를 매우 유용하게 사용할 수 있다.
중요한 것은 회전근개뿐만 아니라 비-회전근개 질환에 대 해서도 익숙해져야하고 초음파로 진단하기 어려운 견관절 질환까지 정확하게 파악하고 있어야만 견관절 통증이나 문 제가 있는 경우 자신있게 초음파 검사를 시행할 수 있다는 것이다. 본 고에서는 견관절의 비-회전근개 구조물로서 이 두박근장두건(long head of the biceps tendon), 회전근개간 격(rotator interval), 점액낭들(bursae), 관절낭(joint capsule), 관절순(labrum), 상완골두(humeral head), 상완관절(gleno- humeral joint), 견봉-쇄골관절(acromioclavicular joint) 등에 서 발생될 수 있는 여러 가지 질환의 초음파 소견에 대해 논한다.
비회전근개 구조물들의 병적 초음파 소견 1. 이두박근장두건(long head of the biceps tendon)
의 손상
대부분의 초음파 전문가들이 견관절 초음파 검사를 이두 박근장두건에 대한 횡단면상(transverse view)에 대한 관찰 로 시작한다. 이유는 이두구(bicipital groove)의 독특한 형 상 때문에 찾기가 쉽고 이를 기준으로 내측에는 견갑하근건 (subscapularis tendon)과 소결절(lesser tuberosity)이 있고 외측에는 극상근건(supraspinatus tendon)과 대결절(greater tuberosity)이 있어 견관절에 대한 전반적인 해부학적 방향
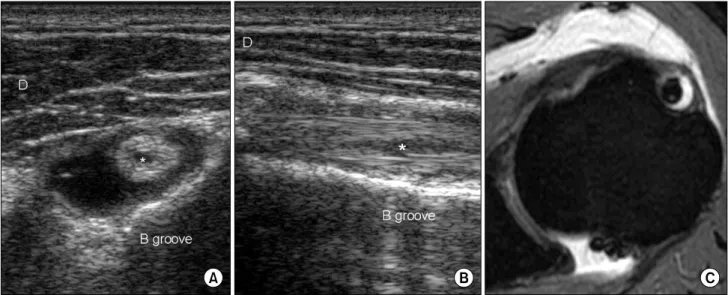
Fig. 2. A male patient (58 yo), who used to be a leather-tanner, with bilateral shoulder pain. A hypoechoic structure suggesting scar tissue is seen instead of a hyperechoic fibrillar biceps tendon in the transverse (A) and longitudinal (B) planes. The gross appearance (C) of his arm is quite typical. D: deltoid, B groove: bicipital groove, SCT: subscapularis tendon.
Fig. 1. A left shoulder pain patient (M/59) shows a longitudinal tear (*) of the long biceps tendon in the transverse (A) and longitudinal (B) planes. The tear is not easily seen in his MR image (C). He had a concomitant full-thickness tear in his supraspinatus tendon.
D: deltoid, B groove: bicipital groove.
을 잡을 수 있기 때문이다. 회전근개와 마찬가지로 이두박 근장두건도 강한 외상이나 반복적 손상에 의해 파열이 올 수 있는데 작은 실질내 파열로부터 완전파열까지 다양한 정도의 손상을 볼 수 있다. 초음파 영상은 실제 구조물보다 확대하는 효과가 있으므로 작은 실질내 파열의 경우 자기 공명영상보다 더 예민하게 진단하는 경우도 많다(Fig. 1).
이두박근장두건의 완전 파열의 경우 이론적으로는 이두구
내에 힘줄이 없어져서 쉽게 진단할 수 있을 것 같으나 실제 로는 이두구속에 연부조직신호가 보이는 경우가 많아 경험 이 많지 않은 검사자는 힘줄이 있는 것으로 착각하기도 한 다. 이런 경우 탐색자를 여러 방향으로 움직여(rocking) 비 등방성 인공음영(anisotropic artifact)을 최소화하여 관찰하 고 종단면상(longitudinal view)에서도 건의 명확한 섬유형 (fibrilla pattern)이 보이지 않는 것으로 완전 파열을 진단할
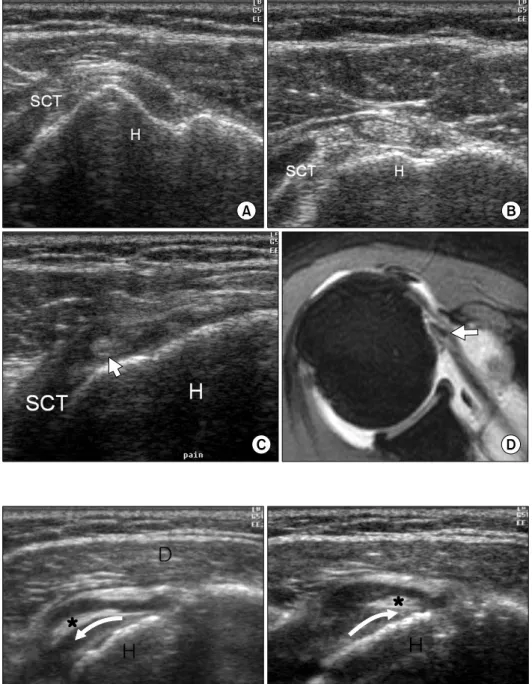
Fig. 3. No tendinous structure is seen in the bicipital groove of a 55 year old female (A). Her long bi- ceps tendon is visualized prox- imally on the subscapularis tendon (SCT) (B). Medial scanning re- veals the long biceps tendon (ar- row) lies deeper to the torn SCT in full thickness (C). The correspond- ing axial MR image is also shown (the arrow indicates the dislocated long biceps tendon) (D). H: hum- eral head.
Fig. 4. Medial and lateral move- ment of the long biceps tendon (*) can be observed when the shoulder is medially (A) and laterally (B) rotated while the long biceps ten- don is seen in its transverse plane.
D: deltoid, H: humeral head.
수 있다. 반대측과 비교해 보는 것도 좋은 방법이며 파열이 되었던 병력이나 이두박근 알통이 특징적으로 커지는 양상 (뽀빠이 형상, Popeye appearance)으로 추가적인 정보를 얻 는 것도 좋은 방법이다(Fig. 2).
2. 이두박근장두건(long head of the biceps tendon) 의 탈구
이두구에서 이두박근장두건이 발견되지 못하면 장두건 의 완전 파열로 진단하기 전에 장두건을 따라 근위부로 탐
색자를 옮겨 회전근개간격부위에서는 장두건이 관찰될 수 있는지 확인하는 것이 중요하다. 이러한 경우는 장두건의 완전 파열이 아니라 탈구일 가능성이 높다. 탐색자를 내측 으로 이동하여 견갑하근건쪽을 조사하면 탈구된 장두건을 발견할 수도 있다. 견갑하근건의 파열이 동반된 경우에는 탈구된 장두건이 견갑하근건보다 더 깊이에서 발견될 수도 있다(Fig. 3). 장두건이 이두구에서 완전히 탈구되지 않은 아탈구 상태에서는 견관절을 내, 외회전하면서 장두건이 움직이는 것을 관찰할 수도 있다(Fig. 4).
Fig. 6. Ultrasound findings (A) and anatomic drawing (B) of the rota- tor interval structures. SST: supra- spinatus tendon, SCT: subscapu- laris tendon, B: long biceps tendon, C: coracohumeral ligament, S: su- perior glenohumeral ligament.
Fig. 5. Modified Crass position for the examination of the rotator in- terval.
3. 회전근개간격(rotator interval)의 질환
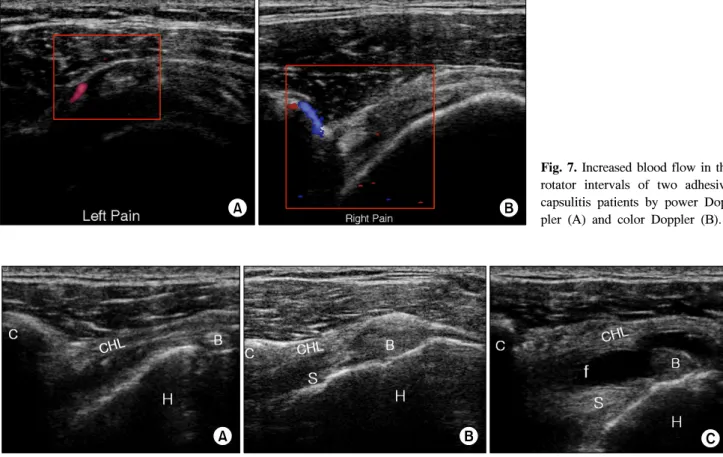
견관절의 하방을 제외하고는 4개의 회전근개건이 상완 골구를 단단히 감싸고 있으나 견갑하근건과 극상근건 사이 에는 이두박근장두건이 관절내로 들어가기 위한 공간이 있 다. 이 공간을 회전근개간격이라고 하는데 회전근개간격은 Fig. 5와 같은 변형크라스자세(modified Crass position)에 서 잘 관찰할 수 있다. 이 공간에는 오구상완인대(coraco- hemeral ligament)가 상부를 차지하고 이두박근장두근이 가운데 그 하부는 상상완관절인대(superior glenohumeral ligament)로 이루어진다(Fig. 6).4) 최근 회전근개간격의 중 요성에 대한 관심이 높아지고 있는데 이는 회전근개간격이 극상근건과 견갑하근건과의 밀접한 생역학적 관계가 있으 며5,6) 유착성관절낭염의 주된 병변부위로 주목을7-9) 받기 때문이다. 즉, Fig. 7, 8과 같이 유착성관절낭염이 있으면 회
전근개간격에서 도플러 소견상 혈류의 증가를 보이거나10) 오구상완인대의 비후를 관찰할 수 있다8-11)고 보고되었다.
그러나 상기 연구결과를 자세히 들여다보면 연구에 포함된 유착성관절낭염환자들 중 정상 소견을 보이는 경우가 상당 한 수에 이름을 알 수 있으며 실제 임상에서도 모든 유착성 관절낭염환자에서 상기 소견이 관찰되지 않는 것을 경험하 게 되어 진단적 가치가 아주 높은 소견은 아닌 것으로 보인 다. 아마도 초음파 소견을 관찰할때의 유착성관절낭염의 병기(stage)가 조금씩 달라서 발생되는 문제로 보인다.
4. 점액낭(bursae)의 질환
견관절내에는 수 개의 점액낭이 정상적으로 존재하는데 우리 몸에서 가장 큰 점액낭으로 알려진 견봉하삼각근하 점액낭(subacromial-subdeltoid bursa)과 견갑하 점액낭(sub- scapular bursa), 이두박근 점액낭(bicipital bursa), 오구하
Fig. 7. Increased blood flow in the rotator intervals of two adhesive capsulitis patients by power Dop- pler (A) and color Doppler (B).
Fig. 8. Coracohumeral ligaments (CHL) in the rotator intervals of the contra-lateral healthy shoulder of a 54 year old male with adhesive capsulitis (A), the adhesive capsulitis shoulder of a 62 year old female (B), and the adhesive capsulitis shoulder with fluid (f) infused in male patient (C). It is noted that the CHLs are thicker in the adhesive shoulders (B, C). The fluid infused in the shoulder joint (C) helps the visualization of the CHL and the hypertrophied synovial tissues (S). C: coracoid process, B: long biceps tendon, H: humeral head.
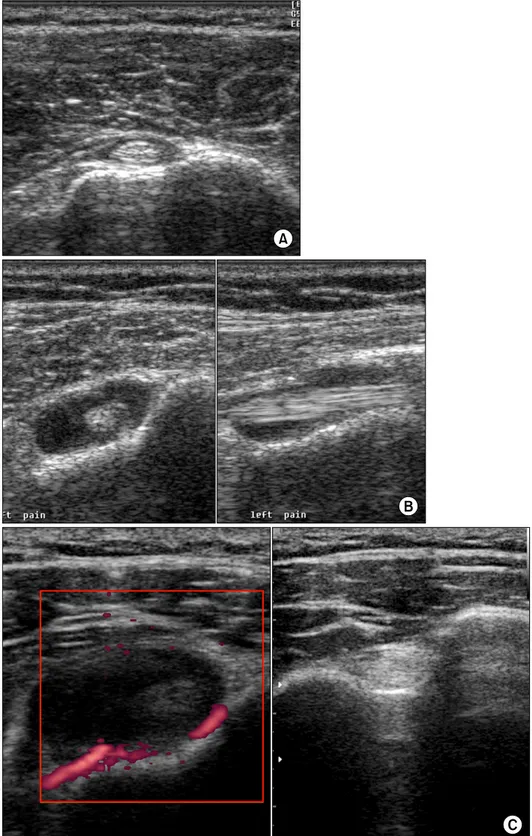
점액낭(subcoracoid bursa) 등이다. 이들 중 이두박근 점액 낭은 건초(tendon sheath)로 간주하여 이두박근 건초(bici- pital sheath)라고 불리기도 하며 견관절의 관절낭과 서로 소통되는 것으로 알려져 있다.3) 견관절내의 관절액이 증가 하면 이두박근 점액낭도 같이 종대가 되므로 세균성 혹은 비세균성 관절염이나 유착성 관절낭염, 회전근개 손상 등 의 질환에서 이두박근 점액낭의 종대를 쉽게 관찰할 수 있 다(Fig. 9). 따라서 이두박근 점액낭의 종대를 초음파로 관 찰하는 경우 이두박근 점액낭염(bicipital bursitis)이나 이두 박근 건염(bicipital tendonitis)이라고 진단하기 보다는 견관 절 자체의 질환의 가능성을 먼저 고려해야 한다.12)
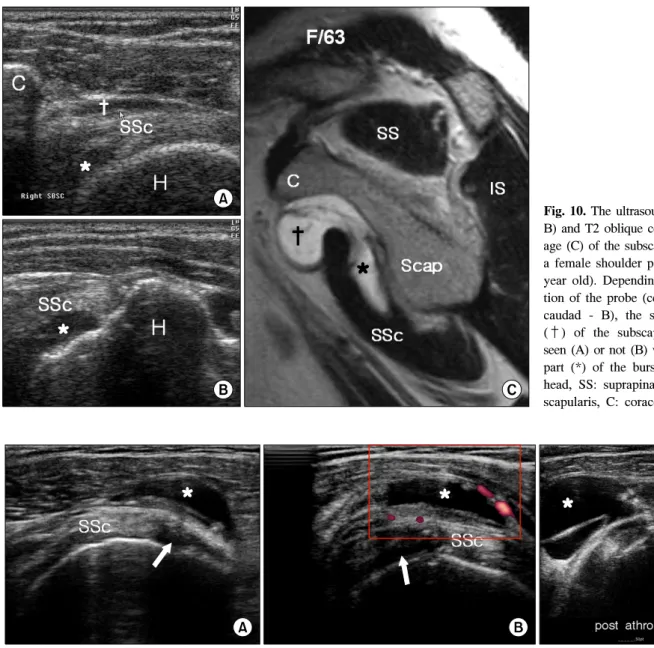
견갑하 점액낭은 견갑하근보다 더 깊이 위치하여 견갑하 근과 견갑골 사이에 점액낭의 대부분이 존재하고 점액낭의 상부만 견갑하근 위로 돌출되어 오구아래에까지 이른다.13) 견갑하 점액낭에 삼출액이 차면 견갑하근 위로 돌출된 점 액낭의 상부가 잘 관찰될 수 있다(Fig. 10). 견갑하 점액낭 역시 견관절낭과 소통-주로 중상완인대와 하상완인대사이
에서-하는 것으로 알려져 견갑하 함요(subscapular recess) 라고 불리기도 한다. 그러나 최근 42개의 사체 견관절에 대 한 연구13)에 의하면 견갑하 점액낭과 견관절낭의 직접적인 소통은 관찰 되지 않았고 단지 회전근개간격부위에서 견갑 하 점액낭과 견관절 사이에 얇은 활액막으로 경계가 나눠 져 있음을 보고하였다. 아마도 견관절낭내 관절액이 증가 하거나 수액을 주입하는 경우 이 활액막 경계가 허물어지 면서 소통이 일어날 가능성이 있어 보이며 이는 3,368개의 통증있는 견관절에 관절조영술을 시행하여 67.7%에서 견 갑하 점액낭에 조영제가 침투함을 관찰한 결과14)와 일맥상 통하다고 볼 수 있다. 즉, 초음파로 관찰되는 견갑하 점액낭 의 종대도 점액낭의 염증이나 견갑하근건의 점액측 손상을 의미할 수도 있지만 견관절 자체의 다른 질환의 표현일 수 도 있음을 기억해야 한다.
오구하 점액낭(subcoracoid bursa)은 견갑하근보다 피부 쪽에 오구돌기보다 더 하방에 위치하는 점액낭으로 상기 언급된 Colas 등의 연구에서 28%의 사체에서 견갑하 점액
Fig. 9. Ultrasonographic findings of bicipital bursae of normal (A), adhesive capsulitis (B) and a side by side comparison of a male rheu- matoid arthritis patient (C) show- ing increased blood flow by Power Doppler technique.
낭과 통해 있었다고 보고되기는 하지만 관절낭과 직접적으 로 소통되는 견갑하 점액낭과는 구별되는 점액낭이다. 삼 출액의 증가로 오구하 점액낭이 확연히 보이는 경우는 석
회성 점액낭,15) 견갑하근건을 포함하는 회전근개 손상,16) 견관절 불안정성17) 등으로 초음파 견관절 진단에 많은 도 움을 준다(Fig. 11). 자기공명영상검사상 오구하 점액낭과
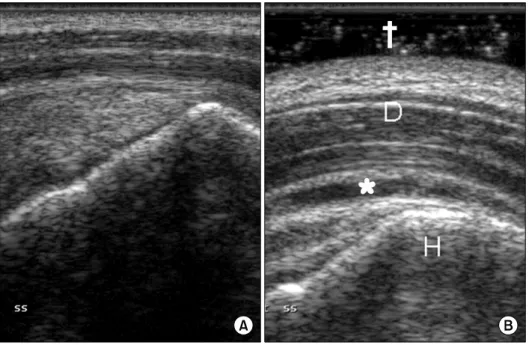
Fig. 11. A swollwen subcoracoid bursa (*) in a female patient with a high grade articular side partial thickness tear (arrow) of the subscapularis tendon. The longitudinal (A) and transverse (B) views of the subscapular (SSc) tendon are shown. The bursa swelling becomes much larger after intra-articular injection of 20 ml fluid (C), which confirms that the tear (arrow) of SSc is in full-thickness.
Fig. 10. The ultrasound images (A, B) and T2 oblique coronal MR im- age (C) of the subscapular bursa of a female shoulder pain patient (63 year old). Depending on the posi- tion of the probe (cephalad - A or caudad - B), the superficial part (†) of the subscapular bursa is seen (A) or not (B) with the deeper part (*) of the bursa. H: humeral head, SS: suprapinatus, SSc: sub- scapularis, C: coracoid process.
견봉하/삼각근하 점액낭이 소통한다는 보고15,18)가 있으나 사체연구13)에서는 소통이 없음이 확인되었다. 아마도 회전 근개전층 손상 후 견봉하/삼각근하 점액낭과 동시에 종대 가 되었거나 아니면 실제 점액낭 자체 보다 점액낭이 있는 잠재적 공간은 서로 소통하고 있어 아마도 이 공간에 삼출 액이 발생하면서 양쪽 점액낭 모두가 종대된 것으로 보였 을 가능성이 높다.
견봉하삼각근하 점액낭은 정상적인 상태에서는 삼출액 이 관찰되지 않는 잠재적 공간으로15) 초음파상에서는 점액 낭주변에 음영이 증가된 지방만 보인다(Fig. 12). 소량의 삼
출액이 발생한 경우에는 탐색자에 젤을 많이 도포하여 압 박을 가하지 않거나(Fig. 13) 환자가 앉아서 검사를 받으면 견봉하삼각근하 점액낭의 가장 아래쪽인 대결절 바로 옆에 서 삼출액을 관찰해야만(Fig. 14) 점액낭의 종대를 확인할 수 있다.19) 다른 점액낭과 마찬가지로 세균성 혹은 석회성 점액낭염에 의해 심하게 종대될 수 있으며(Fig. 15) 회전근 개의 전층 파열 혹은 점액낭측 부분파열에 동반하여 삼출 액의 증가가 관찰될 수도 있다(Fig. 16).12) 류마치스성 관절 염이나 류마티스성 다발성 근육통(polymyalgia rheuma- tica)에서도 특징적으로 견봉하삼각근하 점액낭의 종대가
Fig. 12. A nomral subacromial-subdeltoid bursa of a young healthy male shown in the longitudinal view of the supraspinatus tendon (SST). The hyperechoic band denoted by the black straight arrows is the bursa, which is not shown in this image but the peribursal fat tissues. Novice sonographers are easy to be confused by the low echo band of deltoid (D) muscle tissues just superficial to the bursal fat (curved white arrow). H: hum- eral head.
Fig. 14. Anather way to visualize a small collection of fluid (*) in the subacromial-subdeltoid bursa is to put the probe caudal to the supraspinatus tendon (SST) to see the most dependent part of the bursa when the patient is in a sitting position. H: humeral head, D: deloid.
Fig. 13. A 29 year old female pa- tient with chronic shoulder pain.
Her subacromial-subdeltoid bursal swelling (*) was so small that it was not visible (A) before the pres- sure of the probe was minimized (B) (see †, showing thick gel be- tween the skin and probe).
확찰된다.20)
5. 관절순(labrum) 손상
관절순은 회전근개보다 더 심부에 위치하여 회전근개보 다 관찰이 어려울 뿐만 아니라 전방과 상방의 관절순은 오 구돌기와 견봉에 의해 초음파의 투과가 차단되므로 관찰이
더욱 어렵다. 따라서 관절순의 손상이나 병변을 보기 위해 가장 좋은 영상학적 검사는 자기공명영상이며 관절순 손상 에 대한 초음파 검사의 진단적 가치는 제한적이다. 초음파 로 관절순 손상을 잘 관찰할 수 있는 경우는 후방관절순의 손상이 있는 경우이다. 후방관절순은 극하근건에 대한 종 축영상을 얻기 위한 위치에서 잘 보이는데 관절와(bony glenoid)와 관절순 사이에 저에코 음영을 관찰되거나(Fig.
17), 팔을 움직임에 따라 관절순이 움직이거나, 퇴행되고
Fig. 16. Fluid collection (f) in the subacromial-subdeltoid bursa is shown in longitudinal (A) and transverse (B) views. It was found out that the bursa swelling was as- sociated with the full-thickness tear of the supraspinatus tendon (C and D).
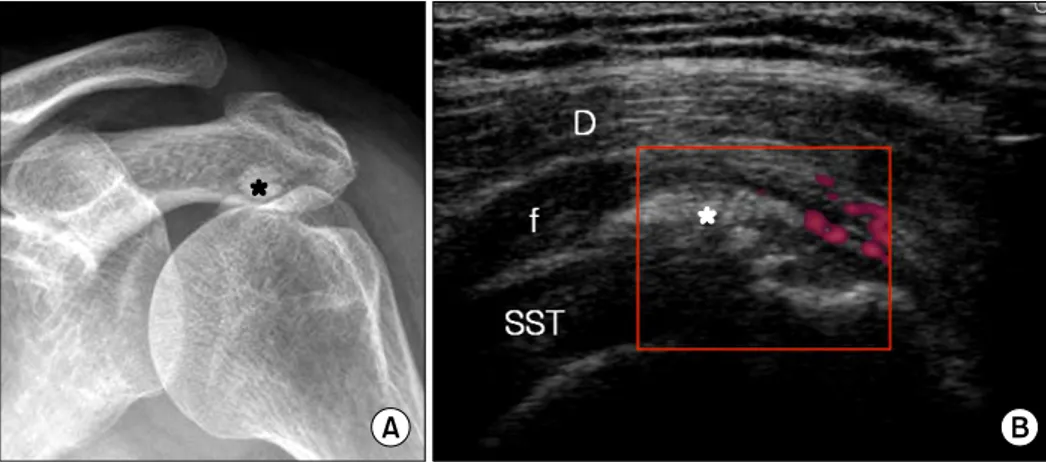
Fig. 15. X ray (A) and sonographic (B) images of a soft calcific nodule (*) in the bursal surface of the supraspinatus tendon of a 50 year old femal dermatomyositis patient. The subacromial-sub- deltoid bursa is irritated by the calcium material that results in calcific bursitis with fluid collec- tion (f) and increase of blood flow (by Power Doppler). The patient had a very serious pain on her left shoulder that she could not sleep for several days. SST: supraspinatus tendon, D: deltoid.
위축된 관절순, 진공현상(vacuum phenomenon)-관절와와 관절순 사이에 기체가 관찰되는 현상-등이 관찰될 때 관절 순 손상을 진단할 수 있다.21,22) 그러나 정상적으로 관절와 (bony glenoid)와 관절순사이에 2 mm 정도의 저에코 음영 은 관찰될 수 있으므로19) 2 mm 이상의 저음영을 진단 기준 으로 삼는 경우가 많다. 때로 해부학위치에서는 관절와와
관절순사이의 간격이 거의 없어 정상으로 보이지만 탐색자 를 견관절의 후방에 위치하고 견관절을 내회전(internal ro- tation)-체간횡단내전(crossbody adduction) 시키면서 관찰 하면 관절순이 관절와로부터 떨어져 나오는 양상을 관찰할 수 있으므로 관절순 손상이 의심이 되는 경우 동적 검사를 시행하는 것이 필요하다(Fig. 18).21)
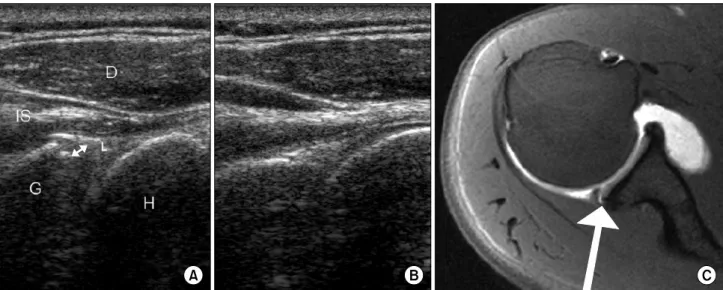
Fig. 17. Torn posterior labrum of a 42 year old male with a SLAP lesion in his right painful shoulder (A). Note the wider hypoechoic zone (arrow) at the base of his labrum (L) compared with that of his left shoulder (B). His torn superior labrum (arrow) is visualized in a MR arthrographic image (C).
Fig. 18. A male patient who had chronic severe left shoulder pain shows an apparently normal posterior labrum (A) in the routine sonography. However, a significant gap between the bony glenoid and labrum (hypoechoic space marked with *) is found when his arm is moved across his trunk (B). The arrow denotes the direction of the humeral head rotation. The posterior labral tear was con- firmed by MR arthrography (C).
6. 관절낭(joint capsule)
유착성관절낭염(adhesive capsulitis)은 관절낭의 염증과
섬유화7,23-25)가 보고되어 있으며 자기공명영상에서 이에 합
당한 소견을 관찰할 수 있다고 알려져 있으나8,26) 초음파 소 견상 관절낭의 비후를 관찰한 보고는 흔치 않고 주로 회전 근개간격의 이상소견이 관찰되는 것으로 보고되고 있다.9) 이는 아마도 관절낭의 두께가 1 mm 정도로 얇고 회전근개 건이 관절낭에 부착되어 있어5,6) 확연한 구분이 쉽지 않은
이유27)로 생각된다.
7. 상완골두(humeral head)의 질환
초음파로 발견할 수 있는 상완골두의 문제는 골절, 골미 란(bony erosion), 골수염(osteomyelitis), 골종양 등이다. 골 절을 보기 위해서는 단순 방사선 촬영을 하는 것이 원칙이 겠으나 때로는 작은 골절이나 견봉 등에 의해 가려진 부분 의 골절은 단순방사선 촬영보다 초음파 검사에서 발견되는 경우도 있다. 초음파 검사상의 골절은 고신호 강도의
Fig. 19. A 66-year-old woman with greater tuberosity fracture. Transverse sonogram (A) shows mildly displaced fracture of the greater tuberosity (arrows) that was not revealed on routine plain X rays (B) but the caudal tilt view (C). D: deltoid, H: humeral head, SST:
supraspinatus tendon.
Fig. 20. A side to side comparison of a patient (M/31) with an os- teochondral compression fracture (Hill-Sachs lesion, arrow). He had a history of falling on his left shoulder. MR arthrography of his left shoulder reveals 1 cm sized shallow bony defect in the postero- lateral aspect of the humeral head (A, straight arrow) corresponding the Hill-Sach lesion and globular enlarged anteroinferior labrum (B, curved arrow) suggesting an old Bankart lesion.
Fig. 21. The sonographic (A) and simple X ray (B) findings of a rotator cuff arthropathy shoulder. In the ultrasound image, there is no supraspinatus tendon between the acromion
“A” and humeral head “H”. The irregular sur- face of the humeral head is noted. Slight supe- rior migration of the humeral head with mild erosion of the superior glenoid is seen in the true AP view, which suggests early changes of rotator cuff arthropathy.
Fig. 22. Normal versus swollen acromio-clav- icular joint (A versus B). The clavicle “C” is normally higher than the acromion “A”. The joint space can be widened when it is sprained (C and D) or be narrowed in a degenerative condition (E and F).
골피질선이 끊어지거나 끊어지면서 층이 지는 양상을 보이 게 된다(Fig. 19). 골미란은 초음파로 발견할 수 있는 확률
이 단순 방사선에 비해 7배 이상 높다.28) 특히, 대결절에서 발견되는 골미란은 회전근개 손상과 관계가 깊은 것으로
Fig. 23. Normal coraco-acromial and coraco-clavicular ligaments are shown with arrows (A and B, re- spectively). The coraco-acromial (C, D) and coraco-clavicular (E, F) ligaments are not visualized in the affected shoulder of a male patient who had a severe shoulder injury in a traffic accident. Normal liga- ments (arrows) are seen in his con- tral-lateral healthy shoulder. C: co- racoid process, A: acromion, clav:
clavicle.
알려져 있다.29) 골수염이나 골종양이 있을 때는 골피질이 나 골막의 변화를 초음파로 관찰할 수도 있다.30)
견관절 전방 탈구 후 발생되는 Hill-Sachs 병변도 초음파 로 쉽게 관찰할 수 있는데 이는 상완골두의 후방-외측에 위 치하는 골-연골 압박골절로 나타난다. 이는 극하근건이 대
결절에 삽입하는 부위 근처에서 고신호 강도의 상완골에 얕은 쇄기 모양의 결손의 형태로 보이는데 문제는 회전근 개 손상 때 발생하는 골미란과 감별이 쉽지 않다는 것이다 (Fig. 20).19) 회전근개 손상 때 발생하는 골미란은 Hill- Sachs 병변에 비해 크기가 작고 좀 더 얕으며 상완골두의
Fig. 24. Asymptomatic (A, B) and symptomatic (C, D) ganglions. A 74 year old male patient had an asymptomatic ganglion (*) super- ficial to the long biceps tendon (A, B). A 48 year old female patient complained a vague posterior shoulder pain without any motor weakness. A ganglion cyst (*) un- der the infraspinatus (IS) was found and subsequent aspiration of the cyst relieved her symptom immediately. H: humeral head, S:
scapular, D: deltoid.
해부학적 경부보다 약간 더 미측(caudal)에 위치하는 경향 이 있으나 이 기준 만으로는 명확하게 구분할 수는 없고 견관절 탈구 혹은 불안정성에 대한 병력, 진찰 소견 등을 모두 종합하여 판단하여야 한다. 견관절 불안정성의 10%
이하에서 발생하는 후방 탈구에서는 Trough 골절이나 McLaughlin 골절이 견갑하근건 아래의 상완골두에서 발견 될 수 있다.
8. 상완관절(glenohumeral joint)의 질환
상완관절 자체의 질환이나 병변은 관절면의 위치적 특성 상 초음파검사보다는 자기공명영상이 더 정확한 영상학적 소견을 제공하고 심한 경우에는 단순방사선 검사만으로도 확연한 소견을 보일 때가 많다. 초음파 영상에서 보이는 소 견은 관절면과 피질의 불규칙한 형태를 보이고 회전근개관 절증(rotator cuff arthropathy)의 경우 회전근개건의 광범위 한 파열로 회전근개건을 관찰할 수 없는 소견을 같이 관찰 하게 된다(Fig. 21).
9. 견봉-쇄골관절(acromioclavicular joint)
견봉-쇄골관절은 일회성 충격 혹은 반복적 손상의 축적 에 의한 퇴행성 변화에 의해 통증을 유발할 수 있다. 초음파 소견에서는 전자의 경우 관절강의 확장을 보이며 후자의
경우 관절강이 협소해지고 골극이 관찰된다(Fig. 22). 관절 강의 넓이를 평가하기 위해서는 정상 견봉-쇄골관절의 후 방의 관절강이 좁고 전방은 넓어지는 해부학적 구조를 보 인다는 사실을 기억하는 것이 중요하다. 견봉-쇄골관절의 손상이나 퇴행에서는 관절내 삼출물의 증가로 관절낭의 팽 창도 관찰될 수 있다(Fig. 22). 그러나, 초음파 영상에서 관 찰되는 관절의 퇴행성 변화가 반드시 통증의 원인이 되는 것은 아니므로 견봉-쇄골관절에 대한 압통이나 견관절의 수평-내전에 의해 통증이 유발되는지를 확인하는 것이 필 요하다.31) 견봉-쇄골관절에 외상이 있는 경우 오구-쇄골인 대(coraco-clavicular ligament)와 오구-견봉인대(coraco-ac- romial ligament)의 손상이 동반되는 경우가 많으므로 이를 초음파로 확인해야 한다(Fig. 23). 환자가 관절을 움직이면 서 구조물을 관찰할 수 있는 초음파 검사의 장점을 이용하 여 최근 견봉-쇄골관절의 염좌에 대한 진단율을 높이기 위 한 동적 초음파 검사를 시행한 보고도 있다.32)
10. 낭종
다른 관절과 마찬가지로 견관절에도 결절종 등의 낭종이 발견되는 경우가 드물지 않다. 낭종은 주변과 확연히 구분 이 되는 저음영으로 나타나므로 쉽게 진단할 수 있는데 무 증상인 경우가 많지만 크기가 크거나 신경을 누르는 경우
통증의 원인이 될 수도 있다. 이런 경우는 초음파 유도하 흡인술로 쉽게 해결되는 경우가 많다(Fig. 24).
결 론
견관절 질환에 대한 정확한 진단을 위해서는 회전근개건 뿐만 아니라 비회전근개 구조물들의 병적 소견을 정확히 파악하는 것이 매우 중요하다. 회전근개 질환과 비회전근 개 질환가 동시에 존재하는 경우도 많고 비회전근개 질환 만으로도 견관절 통증의 원인이 되는 경우도 흔하기 때문 이다 따라서 회전근개 질환과 비회전근개 질환 그리고 초 음파를 이용하여 정확히 진단하기 어려운 질환들에 대해서 도 충분한 지식과 경험이 있어야만 견관절에 대한 정확한 초음파 진단이 가능할 것이다.
감사의 글
본 종설에 실린 모든 초음파 영상(Fig. 24의 C, D 제외) 은 주식회사 메디슨의 Sononace 8800과 Accuvix V10 장비 로 획득된 것으로 주식회사 메디슨의 지원에 감사의 뜻을 표하는 바이다.
참 고 문 헌
1. Dinnes J, Loveman E, McIntyre L, Waugh N. The effec- tiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review.
Health Technol Assess 2003;7:1-166.
2. Ardic F, Kahraman Y, Kacar M, Kahraman MC, Findikoglu G, Yorgancioglu ZR. Shoulder impingement syndrome: re- lationships between clinical, functional, and radiologic findings. Am J Phys Med Rehabil 2006;85:53-60.
3. Papatheodorou A, Ellinas P, Takis F, Tsanis A, Maris I, Batakis N. US of the shoulder: rotator cuff and non-rotator cuff disorders. Radiographics 2006;26:e23.
4. Plancher KD, Johnston JC, Peterson RK, Hawkins RJ. The dimensions of the rotator interval. J Shoulder Elbow Surg 2005;14:620-5.
5. Clark J, Sidles JA, Matsen FA. The relationship of the gle- nohumeral joint capsule to the rotator cuff. Clin Orthop Relat Res 1990;254:29-34.
6. Clark JM, Harryman DT, 2nd. Tendons, ligaments, and cap- sule of the rotator cuff. Gross and microscopic anatomy. J Bone Joint Surg Am 1992;74:713-25.
7. Bunker TD, Anthony PP. The pathology of frozen shoulder.
A Dupuytren-like disease. J Bone Joint Surg Br 1995;
77:677-83.
8. Mengiardi B, Pfirrmann CW, Gerber C, Hodler J, Zanetti M. Frozen shoulder: MR arthrographic findings. Radiology 2004;233:486-92.
9. Homsi C, Bordalo-Rodrigues M, da Silva JJ, Stump XM.
Ultrasound in adhesive capsulitis of the shoulder: is assess- ment of the coracohumeral ligament a valuable diagnostic tool? Skeletal Radiol 2006;35:673-8.
10. Lee JC, Sykes C, Saifuddin A, Connell D. Adhesive capsu- litis: sonographic changes in the rotator cuff interval with arthroscopic correlation. Skeletal Radiol 2005;34:522-7.
11. Lee JC, Guy S, Connell D, Saifuddin A, Lambert S. MRI of the rotator interval of the shoulder. Clin Radiol 2007;
62:416-23.
12. Arslan G, Apaydin A, Kabaalioglu A, Sindel T, Luleci E.
Sonographically detected subacromial/subdeltoid bursal ef- fusion and biceps tendon sheath fluid: reliable signs of rota- tor cuff tear? J Clin Ultrasound 1999;27:335-9.
13. Colas F, Nevoux J, Gagey O. The subscapular and sub- coracoid bursae: descriptive and functional anatomy. J Shoulder Elbow Surg 2004;13:454-8.
14. Nobuhara K, Supapo AR, Hino T. Effects of joint dis- tention in shoulder diseases. Clin Orthop Relat Res 1994;
304:25-9.
15. Bureau NJ, Dussault RG, Keats TE. Imaging of bursae around the shoulder joint. Skeletal Radiol 1996;25:513-7.
16. Tung GA, Yoo DC, Levine SM, Brody JM, Green A.
Subscapularis tendon tear: primary and associated signs on MRI. J Comput Assist Tomogr 2001;25:417-24.
17. Hirano M, Ide J, Takagi K. Acromial shapes and extension of rotator cuff tears: magnetic resonance imaging evalua- tion. J Shoulder Elbow Surg 2002;11:576-8.
18. Grainger AJ, Tirman PF, Elliott JM, Kingzett-Taylor A, Steinbach LS, Genant HK. MR anatomy of the subcoracoid bursa and the association of subcoracoid effusion with tears of the anterior rotator cuff and the rotator interval. AJR Am J Roentgenol 2000;174:1377-80.
19. Martinoli C, Bianchi S, Prato N, Pugliese F, Zamorani MP, Valle M, et al. US of the shoulder: non-rotator cuff disorders. Radiographics 2003;23:381-401.
20. Soubrier M, Dubost JJ, Ristori JM. Polymyalgia rheuma- tica: diagnosis and treatment. Joint Bone Spine 2006;73:
599-605.
21. Hammar MV, Wintzell GB, Astrom KGO, Larsson S, Elvin A. Role of US in the preoperative evaluation of patients with anterior shoulder instability. Radiology 2001;219:
29-34.
22. Magnusson L, Kalebo P, Baranto A, Lundin O, Wiger P, Kartus J, et al. The value of ultrasonography in the pre- operative diagnostic evaluation of patients with recurrent anterior shoulder dislocation: a prospective study of 44
patients. Knee Surg Sports Traumatol Arthrosc 2007;15:
649-53.
23. Hannafin JA, Chiaia TA. Adhesive capsulitis. A treatment approach. Clin Orthop Relat Res 2000;372:95-109.
24. Hand GC, Athanasou NA, Matthews T, Carr AJ. The path- ology of frozen shoulder. J Bone Joint Surg Br 2007;89:
928-32.
25. Uhthoff HK, Boileau P. Primary frozen shoulder: global capsular stiffness versus localized contracture. Clin Orthop Relat Res 2007;456:79-84.
26. Connell D, Padmanabhan R, Buchbinder R. Adhesive cap- sulitis: role of MR imaging in differential diagnosis. Eur Radiol 2002;12:2100-6.
27. Rozin AP. Differentiating subscapular tendon and gleno- humeral joint on anterior shoulder sonography. Med Sci Monit 2008;14:CS92-5.
28. Wakefield RJ, Gibbon WW, Conaghan PG, O'Connor P, McGonagle D, Pease C, et al. The value of sonography in
the detection of bone erosions in patients with rheumatoid arthritis: a comparison with conventional radiography.
Arthritis Rheum 2000;43:2762-70.
29. Wohlwend JR, van Holsbeeck M, Craig J, Shirazi K, Habra G, Jacobsen G, et al. The association between irregular greater tuberosities and rotator cuff tears: a sonographic study. Am J Roentgenol 1998;171:229-33.
30. Kane D, Grassi W, Sturrock R, Balint PV. Musculoskeletal ultrasound--a state of the art review in rheumatology. Part 2: Clinical indications for musculoskeletal ultrasound in rheumatology. Rheumatology (Oxford) 2004;43:829-38.
31. Walton J, Mahajan S, Paxinos A, Marshall J, Bryant C, Shnier R, et al. Diagnostic values of tests for acromiocla- vicular joint pain. J Bone Joint Surg Am 2004;86-A:
807-12.
32. Philippe Peetrons JPBa. Acromioclavicular joint injury: en- hanced technique of examination with dynamic maneuver.
J Clin Ultrasound 2007;35:262-7.