대한소화기학회지 2008;52:310-314
접수: 2008년 9월 1일, 승인: 2008년 9월 27일
연락처: 박창근, 701-600, 대구광역시 동구 신암동 576-31 대구파티마병원 내과
Tel: (053) 940-7191, Fax: (053) 954-7417 E-mail: endoscope@medimail.co.kr
Correspondence to: Chang Keun Park, M.D.
Department of Internal Medicine, Daegu Fatima Hospital, 576-31, Sinam-dong, Dong-gu, Daegu 701-602, Korea Tel: +82-53-940-7191, Fax: +82-53-954-7417 E-mail: endoscope@medimail.co.kr
위 사구종양 1예
대구파티마병원 내과
박종필ㆍ박승찬ㆍ박창근
A Case of Gastric Glomus Tumor
Jong Pil Park, M.D., Seung Chan Park, M.D., and Chang Keun Park, M.D.
Department of Internal Medicine, Daegu Fatima Hospital, Daegu, Korea
Glomus tumor is a tumor arising from glomus body, a nodular form of arteriolovenular anastomosis that functions to regulate blood flow according to temperature. Gastrointestinal glomus tumors are rare and most frequently oc- cur in the stomach as a subepithelial tumor. A 46-year-old woman presented with an incidental finding of a sub- epithelial tumor in the stomach. Endoscopic ultrasonography (EUS) showed a 1.4×1 cm sized well circumscribed heterogeneous hypoechoic tumor with a few tubular structures in the fourth sonographic layer of the gastric wall.
Characteristically, more hypoechoic halo equal to the echogenecity of proper muscle layer enclosed the tumor.
Contrast enhanced abdominal computerized tomography (CT) revealed high enhancement of tumor up to the same level of portal vein in arterial phase and this enhancement persisted to portal phase. For histolgogic confirmation and treatment, endoscopic enucleation was attempted but failed due to fibrotic adhesion with the surrounding tissue. Histologic findings of biopsy specimen were compatible with glomus tumor. Although it is difficult to di- agnose glomus tumor preoperatively, these characteristic findings in EUS and CT seem to be useful in dis- tinguishing glomus tumor from other tumors arising from the fourth sonographic layer of gastric wall. (Korean J Gastroenterol 2008;52:310-314)
Key Words: Glomus tumor; Subepithelial tumor; Stomach; Endoscopic ultrasonography
서 론
사구종양은 온도 변화에 따라 혈류를 조절하는 신경근동 맥 수용체(neuromyoarterial receptor)인 사구(glomus body)의 변형된 평활근 세포인 사구세포(glomus cell)에서 발생하는 종양으로, 흔히 손톱, 발톱 아래에서 발생하지만, 연부 조직, 피부, 기도, 폐, 간, 췌장 등 우리 몸의 어디에서나 발생할 수 있으며, 위장관에서 드물게 발생한다. 위장관에서는 위, 식도, Vater 팽대부, 대장 등 다양한 보고가 있으나 이 중 위
에서 가장 흔하게 발생하며, 주로 상피하 종양(subepithelial tumor)의 형태로 발현된다.1 따라서 내시경초음파 검사가 진 단에 중요한 역할을 하며, 내시경초음파 검사에서 위벽의 4 번째 층(또는 3번째 층)에서 기원하는 저에코성 병변으로 관찰된다.2 사구종양은 드물게 원격 전이 등 악성화를 할 수 있는 종양이어서,1 다양한 예후를 보일 수 있는 위벽의 4번 째 층에서 발생하는 다른 종양들과의 감별 진단이 중요할 것으로 생각하나, 내시경초음파 소견만으로는 감별이 곤란 하다. 저자들은 내시경 검사에서 우연히 발견된 상피하 종
박종필 외 2인. 위 사구종양 1예 311
Fig. 2. Endosonographic find- ings. (A) It shows a 1.4×1 cm sized well circumscribed heteroge- neous hypoechoic tumor with a few tubular structures in the fourth sonographic layer of the gastric wall. Characteristically more hypoechoic halo equal to echoge- necity of the proper muscle layer encloses the tumor. (B) Tumor is easily deformed on compression by the balloon of echoendoscope.
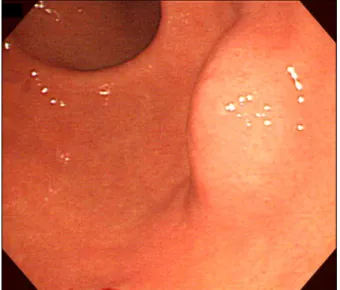
Fig. 1. Endoscopic finding shows a mucosal bulge suggestive of subepithelial tumor at posterior wall of antrum.
양을 주소로 내원한 환자에서 사구종양에 특징적인 소견으 로 보이는 내시경초음파, CT 및 조직 소견을 경험하여 보고 하고자 한다.
증 례
평소 건강하게 지내온 46세 여자 환자가 타 의료기관에서 건강 검진 목적으로 시행한 상부내시경 검사에서 위전정부 에 상피하 종양이 있어 추가 검사를 위해 내원하였다. 과거 력 및 가족력에서 특이 소견은 없었다. 내원 당시 혈압 110/70 mmHg, 맥박 68회/분, 호흡수 16회/분, 체온 36.5oC였 다. 전신 상태와 진찰 소견은 정상이었으며, 말초혈액 검사, 생화학 검사 및 소변 검사에서 특이 소견은 없었다.
상부내시경 검사에서 위전정부 후벽에서 상피하 종양이 관찰되었으며, 생검 겸자로 눌렀을 때 쿠션 징후는 없었다 (Fig. 1). 내시경초음파 검사에서 병변은 위벽의 4번째 층에
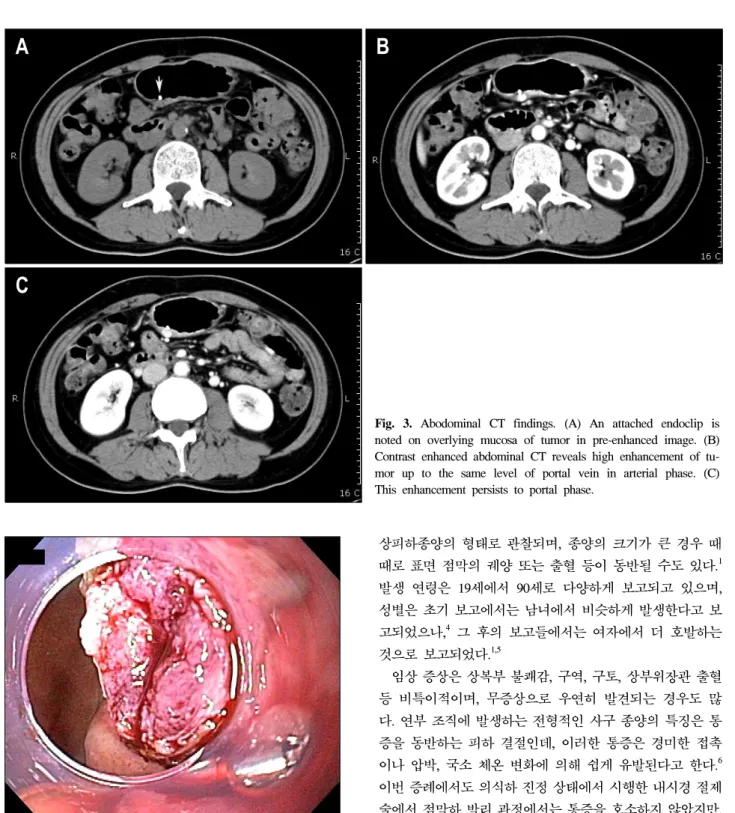
서 1.4×1.1 cm 크기의 비균질 저에코 종양으로 관찰되었고, 특징적으로 종양 주위로 종양보다 에코 수준이 더 낮은 저 에코 halo가 관찰되었다(Fig. 2A). 또한 내시경 선단의 풍선 으로 압박하였을 때 종양의 변형이 관찰되었다(Fig. 2B). 이 러한 소견들은 위장관 간질종양과 같이 통상적으로 4번째 층에서 기원하는 종양과는 다른 비전형적인 소견으로 생각 되어 종양 부위에 반복 생검을 시행하였으나 조직 검사 결 과는 진단적이지 못했다. 복부 CT에서 종양은 동맥기에 문 맥과 거의 유사한 조영 증강을 보여 위장관 간질종양 보다 훨씬 더 강하고 균질성으로 조영 증강이 되었으며, 이러한 조영 증강이 문맥기(portal phase)까지 지속되는 고혈관 종괴 로 관찰되었다(Fig. 3). 조직학적인 확진 및 치료 목적으로 점막하 박리술(submucosal dissection)을 이용한 내시경적 절 제술을 시도하였으나 종양과 주위 조직과의 유착으로 절제 할 수 없었으며, 일부 노출된 종양은 위장관 간질종양이나 평활근종에서 관찰되는 단단한 황백색 종괴가 아니라, 소고 기와 같은 적갈색 및 부드러운 경도를 보였고(Fig. 4), 특징 적으로 조직 생검에도 환자가 통증을 호소하였다. 동결절편 조직검사에서 유암종(carcinoid tumor)으로 진단되었으나, 추 후 시행한 H&E 염색에서 풍부한 혈관들 주위로 균일하게 작고 둥근 세포들이 충실성으로 배열되어 있으며, 개개의 종양 세포들은 균일하고 둥근 핵을 가지며, 세포질은 투명 하거나 경한 호산성을 띠었으며(Fig. 5A), 면역조직화학염색 에서 chromogranin A나 synaptophysin에는 염색이 되지 않았 고, smooth muscle actin에는 강하게 염색되어서 사구종양으 로 진단되었다(Fig. 5B). 세포 분열이나 핵의 이형성은 보이 지 않았다.
환자는 수술 치료를 원치 않고 정기적인 경과 관찰을 원 해 현재 외래에서 경과 관찰 중이다.
312 The Korean Journal of Gastroenterology: Vol. 52, No. 5, 2008
Fig. 4. Endoscopic finding. After partial unroofing of overlying mucosa, exposed tumor appeared fleshy reddish in color and soft in consistency.
고 찰
위에서 발생한 사구종양은 1948년 De Busscher 등이 처음 보고한 이래 비교적 드물게 보고되었으며,2 대개 단발성이 나 드물게 다발성으로 보일 수도 있으며,3 주로 전정부에서
상피하종양의 형태로 관찰되며, 종양의 크기가 큰 경우 때 때로 표면 점막의 궤양 또는 출혈 등이 동반될 수도 있다.1 발생 연령은 19세에서 90세로 다양하게 보고되고 있으며, 성별은 초기 보고에서는 남녀에서 비슷하게 발생한다고 보 고되었으나,4 그 후의 보고들에서는 여자에서 더 호발하는 것으로 보고되었다.1,5
임상 증상은 상복부 불쾌감, 구역, 구토, 상부위장관 출혈 등 비특이적이며, 무증상으로 우연히 발견되는 경우도 많 다. 연부 조직에 발생하는 전형적인 사구 종양의 특징은 통 증을 동반하는 피하 결절인데, 이러한 통증은 경미한 접촉 이나 압박, 국소 체온 변화에 의해 쉽게 유발된다고 한다.6 이번 증례에서도 의식하 진정 상태에서 시행한 내시경 절제 술에서 점막하 박리 과정에서는 통증을 호소하지 않았지만, 생검 겸자로 종양에 대한 조직 검사를 하였을 때 통증이 유 발되었으며, 이는 위장관에서 발생한 사구 종양에서도 내장 통증(visceral pain)과 다른 기전으로 통증이 유발될 수 있음 을 시사하는 소견이다.
이 종양은 주로 상피하종양으로 나타나므로 내시경초음 파 검사가 진단 과정에서 중요한 역할을 하며, 내시경초음 파 소견은 4번째 층(일부 3번째 층)에서 기원하는 비균일 저에코 종양으로 나타나며, 내부에 고에코 반점, 불규칙한 윤곽 등 마치 악성을 시사하는 소견도 보고되었다.7 하지만 Fig. 3. Abodominal CT findings. (A) An attached endoclip is noted on overlying mucosa of tumor in pre-enhanced image. (B) Contrast enhanced abdominal CT reveals high enhancement of tu- mor up to the same level of portal vein in arterial phase. (C) This enhancement persists to portal phase.
Park JP, et al. A Case of Gastric Glomus Tumor 313
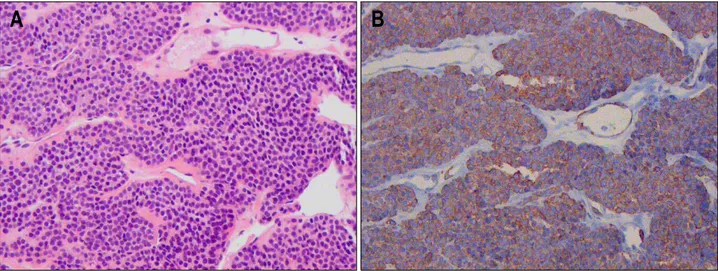
Fig. 5. Histologic findings. (A) The tumor is composed of sheets of uniform small round cells around abundant, variable sized dilated vessels. The tumor cells have round, regularly shaped nuclei and eosinophilic cytoplasms and show no mitosis or nuclear atypia (H&E stain, ×200). (B) On immunohistochemistry, tumor cells are positive for smooth muscle actin (Immunohistochemical stain, ×200).
내시경초음파 소견만으로 위장관 간질종양, 신경초종 (Schwannoma), 평활근종 등과 같은 위벽의 4번째 층에서 기 원하는 종양과의 감별은 불가능하다. 이번 증례에서는 특징 적으로 종양 주위로 종양보다 더 낮은 에코 수준을 보이는 halo가 관찰되었는데, 이전에 발표된 증례들의 내시경초음 파 사진에서도, 비록 저자들이 언급하지는 않았지만, 유사 한 소견들이 관찰되어 이러한 소견이 사구 종양의 특징적인 소견일 수 있을 것으로 보인다.8-10 이러한 저에코 halo는 주 위의 정상 고유근층과 연속되고, 또 비슷한 에코 수준을 보 여, 상대적으로 에코 수준이 높은 사구 종양을 비후된 고유 근층이 둘러싸서 생기는 소견으로 추정되며, 이러한 종양 주위 고유근층의 비후는 일부 보고에서도 지적되고 있다.1,10 하지만 위장관 간질 종양 및 신경초종의 일부에서도, 사구 종양에서만큼 뚜렷하지는 않지만, 종양 주위로 일부 저에코 성 halo가 관찰됨을 보고하고 있어11 이러한 소견이 사구 종 양에 특이적이지는 않음을 시사한다. 또한 내시경 선단의 풍선을 이용해서 종양을 압박하였을 때 종양의 변형이 관찰 되었는데 이는 종양이 어느 정도의 탄력성을 갖고 있음을 시사하며,12 다른 4번째 층의 종양에서 볼 수 없는 소견으로 생각된다.
CT 소견은 위장관 간질종양은 근육과 같거나 약간 강한 조영 증강을 보이는데 비해 사구 종양은 동맥기에는 거의 문맥과 비슷한 정도로 강한 조영 증강을 보이며, 이러한 조 영 증강이 문맥기 및 지연기까지 지속되는 것이 특징이
다.13-15 따라서 상피하종양에 대한 내시경초음파 검사에서 4
번째 층에서 저에코 종양으로 보이나 주위로 종양보다 더 낮은 에코 수준의 뚜렷한 halo로 둘러싸여 있고, 내시경 선 단의 풍선을 이용한 압박 시 종양의 변형이 관찰된다면 추
가로 역동적 복부 CT를 촬영함으로써 위벽의 4번째 층에서 기원하는 다른 종양과 사구종양을 감별하는 데 도움이 될 것으로 보인다.
내시경초음파 유도하 미세침흡인세포검사(endoscopic ultra- sound guided fine-needle aspiraion cytology, EUS-FNA)로 종 양에 대한 조직학적인 진단을 시도할 수 있으나 유암종으로 오진하기 쉬우며, 추가로 면역조직화학염색을 통해야만 사 구 종양을 확진할 수가 있다.5,16 이번 증례에서도 동결절편 조직검사에서는 유암종으로 진단되었으나, H&E 염색 및 면 역조직화학염색을 통해 사구 종양으로 진단되었다. 그 외 상피세포양 위장관 간질종양, 림프종, 평활근종 등과의 감 별이 필요하다.17
사구 종양은 대개의 경우 양성의 임상 경과를 보이나 드 물게는 악성화하여 원격 전이를 일으킬 수 있으며,1 악성을 시사하는 인자로 종양의 위치, 크기, 세포 분열수, 혈관 침 윤, 방추 세포(spindle cell)로의 변형 및 형성이상의 동반 등 이 제시되고 있으나,18 위장관의 사구 종양에 대해서는 아직 연구가 이루어지지 않았다.
치료는 복강경을 이용한 쐐기절제술과 같은 국소 절제술 로 충분하며, 한 연구에서 내시경 절제술을 시도하였으나 이번 증례에서처럼 주위 조직과의 유착으로 종양이 분리되 지 않아 완전 절제를 하지 못했다.19 사구종양은 불완전 절 제 시 국소 재발이 비교적 흔하며, 주로 4번째 층에 위치하 고 주변 조직과 유착되어 천공의 위험이 높다는 점, 이번 증 례에서처럼 시술 중 환자에게 통증을 유발할 수 있다는 점 등으로 내시경 절제술은 부적절할 것으로 생각된다. 추적 관찰도 한 방법일 수 있지만 이러한 경우 환자에게 충분한 설명 및 정기적인 추적 검사가 반드시 필요하다.20
314 대한소화기학회지: 제52권 제5호, 2008
이제까지 발표된 대부분의 사구종양은 수술 후 조직 소견 으로 진단되었으나, 수술 전에 임상 소견만으로 정확한 진 단이 이루어진다면 불필요하게 확장된 수술을 줄일 수 있을 것으로 보인다. 저자들은 이번 증례를 통해서, 종양을 둘러 싸는 뚜렷한 저에코 halo, 압박에 의해 유발되는 종양의 변 형, 종양의 육안, 조직 소견 및 조영 증강 CT에서 문맥과 유 사한 정도의 강한 조영 증강 및 이러한 조영 증강이 문맥기 까지 지속되는 점 등이 위벽의 4번째 층에서 발생하는 다른 간엽 기원 종양들과 구별되는 사구종양의 특징적인 임상 소 견일 것으로 생각되며 여기에 대해서는 향후 추가 연구가 필요할 것으로 생각한다. 또한 사구종양이 의심되는 상피하 종양에서 조직학적인 확진을 고려하다면 반복적인 생검(bite on bite biopsy)이나 내시경초음파 유도하 미세침흡인세포검 사를 고려해 볼 수 있으며, 세포검사의 경우 병리의사에게 충분한 임상 정보를 주어야만 면역조직화학염색과 같은 추 가 검사를 통해 유사한 세포진 소견을 보이는 다른 질환을 감별하는 데 도움이 될 것으로 보인다.
참고문헌
1. Miettinen M, Paal E, Lasota J, Sobin LH. Gastrointestinal glomus tumor: a clinicopathologic, immuohistochemical, and molecular genetic study of 32 cases. Am J Surg Pathol 2002;
26:301-311.
2. Imamura A, Tochihara M, Natsui K, et al. Glomus tumor of the stomach: endoscopic ultrasonographic findings. Am J Gas- troenterol 1994;89:271-272.
3. Haque S, Modlin IM, West AB. Multiple glomus tumors of the stomach with intravascular spread. Am J Surg Pathol 1992;16:291-299.
4. Kanwar YS, Manaligod JR. Glomus tumor of the stomach.
An ultrastructural study. Arch Pathol 1975;99:392-397.
5. Lee HW, Lee JJ, Yang DH, Lee BH. A clinicopathologic study of glomus tumor of the stomach. J Clin Gastroenterol 2006;40:717-720.
6. Freier DT, Lindenauer SM. Subcutaneous gomus tumor. Am J Surg 1970;120:359-362.
7. Debol SM, Stanley MW, Mallery S, Sawinski E, Bardales RH. Glomus tumor of the stomach:cytologic diagnosis by en- doscopic ultrasound-guided fine-needle aspiration. Diagn Cyto-
pathol 2003;28:316-321.
8. Shin HM, Ryu DY, Lee D, et al. A case of glomus tumor of the stomach:role of endoscopic ultrasonography. Korean J Gastrointest Endosc 2000;21:855-858.
9. Lee DS, Han SR, Kim WS, et al. A case of glomus tumor arising in the stomach. Korean J Gastrointest Endosc 2000;21:
559-562.
10. Agawa H, Matsushita M, Nishio A, Takakuwa H. Gastric glo- mus tumor. Gastrointest Endosc 2002;56:903.
11. Okai T, Minamoto T, Ohtsubo K, et al. Endosonographic evaluation of c-kit-positive gastrointestinal stromal tumor.
Abdom Imaging 2003;28:301-307.
12. Harig BM, Rosen Y, Dallemand S, Farman J. The radiology corner:glomus tumor of the stomach. Am J Gastroenterol 1975;63:423-428.
13. Kim JK, Won JH, Cho YK, Kim MW, Joo HJ, Suh JH.
Glomus tumor of the stomach: CT findings. Abdom Imaging 2001;26:303-305.
14. Cha SH, Cho SB, Kim YW, Park CM. Helical CT appear- ance of glomus tumor of the stomach. Eur Radiol 2000;10:
671-673.
15. Hu XY, Hu CH, Fang XM, Zhang TH. Glomus tumor of the gastric body: helical CT findings. Chin Med J 2007;120:
1289-1291.
16. Lorber J, Kalish J, Farraye FA, Cerda S, Babineau TJ.
Glomus tumor of the stomach:case report. Curr Surg 2005;62:
436-438.
17. Kapur U, Hobbs CM, McDermott E, Mooney EE. Gastric glomus tumor. Ann Diagn Pathol 2004;8:32-35.
18. Folpe AL, Fanburg-Smith JC, Miettinen M, Weiss SW.
Atypical and malignant glomus tumors: analysis of 52 cases, with a proposal for the reclassification of glomus tumors. Am J Surg Pathol 2001;25:1-12.
19. Park YS, Park SW, Kim TI, et al. Endoscopic enucleation of upper-GI submucosal tumors by using an insulated-tip electro- surgical knife. Gastrointest Endosc 2004;59:409-415.
20. American Gastroenterological Association Institute. American Gastroenterological Association Institute medical position statement on the management of gastric subepithelial masses.
Gastroenterology 2006;130:2215-2216.