253
Correspondence to: Dae Hwan Kim, Department of Surgery, School of Medicine, Medical Research Institute, Pusan National University Hospital, Ami-dong, Seo-gu, Busan 602-739, Korea. Tel: 051-240- 7238, Fax: 051-247-1365, E-mail: [email protected] Received October 20, 2009, Accepted November 24, 2009
Laparoscopic Resection of a 12 cm Sized Retroperitoneal Schwannoma Adjacent to Retroperitoneal Vital Vessels: Are Large Retroperitoneal
Schwannomas Not Suitable for the Laparoscopic Approach?
Departments of Surgery, 1Internal Medicine, 2Pathology and 3Radiology, School of Medicine, Medical Research Institute, Pusan National University, Busan, Korea
Young Hoon Cho, M.D., Dae Hwan Kim, M.D., Si Hak Lee, M.D., Gyung Mo Son, M.D., Sang Hyup Lee, M.D., Hae Young Kim, M.D.,
Gwang Ha Kim, M.D.
1, Do Yoon Park, M.D.
2, Suk Kim, M.D.
3There are a lot of advantages to laparoscopic surgery, including early recovery, less postoperative pain, better cosmesis, shorter hospital stay and an early return to normal activities because of its minimal invasiveness. So, most surgeons have agreed on these points and have accepted the various indications for laparoscopic surgery.
Despite these advantages and the recent advances in laparoscopic surgery, there are few cases using the laparoscopic approach for treating retroperitoneal schwannomas. Laparoscopic resection of a large retroperitoneal schwannoma has some difficulties for tumor retraction, dissecting around the large vessels, and removal of the resected tumor.
Sometimes these difficulties may cause complications and a lengthened hospital stay. However, if appropriate methods are used, long hospital stay and complication can be prevented while maintaining the advantages of laparoscopic surgery. (J Korean Surg Soc 2010;78:253-257)
Key Words: Schwannomas, Retroperitoneum, Laparoscopic resection
INTRODUCTION
Schwannomas are neurogenic tumors that originate from the schwann cells of peripheral nerve sheaths. Most of them occur in the head and neck, but they are rarely seen in the retroperitoneum. Retroperitoneal schwannomas are generally slow-growing and they can grow to a large size before producing symptoms. Because there are no patho- gnomic radiologic findings, making the definite preopera- tive diagnosis is difficult to do. The treatment of choice for these tumors is complete surgical resection. To date, a conventional open procedure has been used, but lapa- roscopic approaches are increasingly being applied as a
result of the recent advances in laparoscopic surgery. We recently experienced a case of a 12 cm sized retroperitoneal schwannoma that was located adjacent to large vessels. It was successfully treated by laparoscopic surgery without any postoperative complications or extended hospital stay, so we report here on this case along with a review of the relevant literature.
CASE REPORT 1) Patient
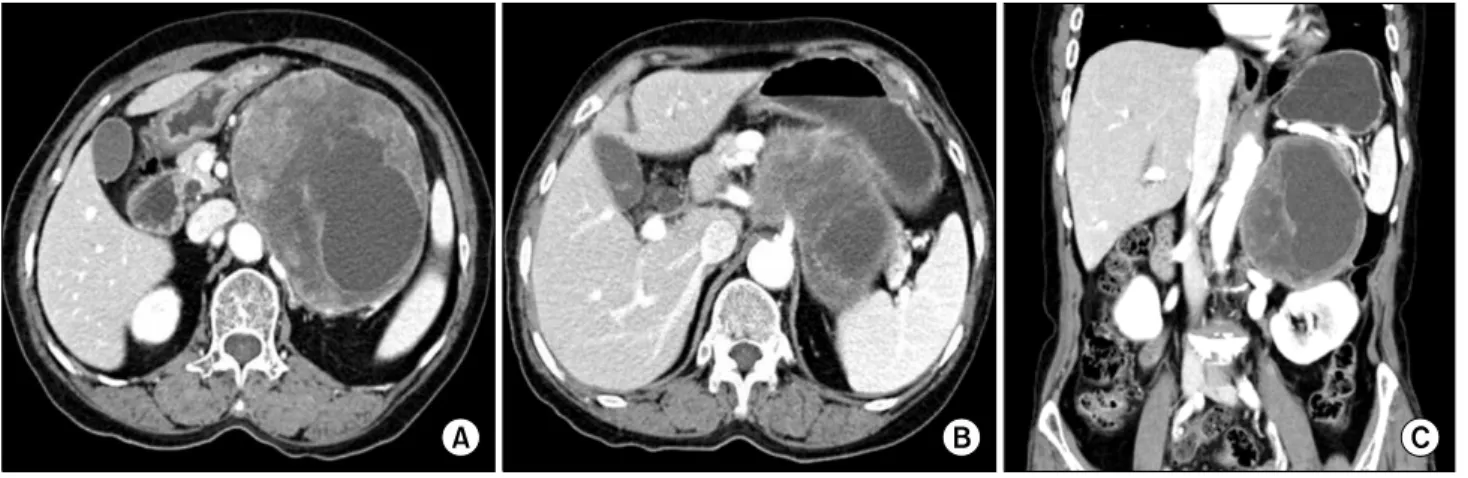
A 73-year-old female was referred to us with indigestion and early satiety. Her past history and family history were unremarkable. Her abdomen was soft on physical exami- nation, but a firm, non-tender mass was palpable in the left upper quadrant of the abdomen. The horizontal section of computed tomography demonstrated a 12×10 cm well- defined, encapsulated mass that had an internal cystic
Fig. 1. Abdominal CT findings. The image shows a 12×10 cm sized retroperitoneal tumor (A). The horizontal section view demonstrates a well-defined, encapsulated mass that has an internal cystic component. The mass is located adjacent to the superior mesenteric artery and celiac trunk (B). On the coronal section view, the mass was located adjacent to the splenic vein, left renal vein, and abdominal aorta (C).
the coronal section of computed tomography, the mass was located adjacent to the splenic vein, the left renal vein, and the abdominal aorta (Fig. 1C). Ultrasonography-guided fine-needle aspiration biopsy was done and the mass was diagnosed as a benign retroperitoneal schwannoma. Based on the preoperative pathologic finding the patient under- went laparoscopic excision and she discharged on the post- operative 4th day without any complication. A permanent histopathologic examination revealed the mass to be a benign schwannoma (Fig. 2).
2) Surgical technique
Under general anesthesia, the patient was placed in a supine position with the legs separated. The operator stood on the patient’s right, the first assistant stood on the patient’s left and the camera operator stood between the patient’s legs. A 10-mm trocar is inserted through a sub- umbilical incision with using an open technique and a pneumoperitoneum was established. Four other trocars (One 12-mm trocar and three 5-mm trocars) were placed.
The dissection began with omentectomy from the splenic flexure to the mid-transverse colon. After exposing the anterior surface of the mass, we dissect the tumor from the surrounding tissue along an avascular plane (Fig. 3A). The
the retraction easier (Fig. 3B). A careful dissection was performed during dissecting near the large vessels. Several feeding arteries from the aorta and drainage veins to the splenic vein were identified and these were securely ligated using laparoscopic endoclips. After complete resection and inserting the tumor into a retrieval bag, tumor removal was performed as described below. We extended the umbilical incision vertically about 3 cm in length (Fig. 3C), a wound protector was inserted and the abdominal skin was draped using a sterile tower. The tumor has a cystic portion, so fluid aspiration was performed to reduce the tumor’s size.
Then we divided the tumor into two fragments in a retrieval bag and then we removed them. After complete tumor removal, we exchanged all the surgical instruments.
One closed suction drain was placed into the surgical field through the 5 mm left lower trocar. The operation time was 205 minutes, and the blood loss was 75 ml.
DISCUSSION
Retroperitoneal schwannomas are rare and they account for 0.7% to 2.7% of all schwannomas.(1) These tumors are usually asymptomatic and discovered incidentally. But sometimes they can grow to a large size and produce
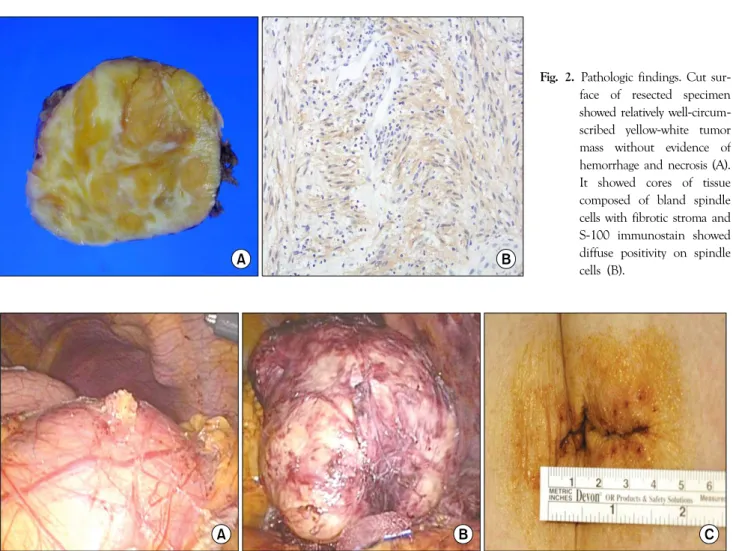
Fig. 2. Pathologic findings. Cut sur- face of resected specimen showed relatively well-circum- scribed yellow-white tumor mass without evidence of hemorrhage and necrosis (A).
It showed cores of tissue composed of bland spindle cells with fibrotic stroma and S-100 immunostain showed diffuse positivity on spindle cells (B).
Fig. 3. Operative findings of laparoscopic resection. After performing omentectomy from the splenic flexure to the mid-transverse colon, the anterior surface of the tumor was exposed (A). The operative findings after completed resection of the tumor from the surrounding tissue (B). After complete resection, we vertically extended the umbilical incision about 3 cm in length to remove the resected tumor (C).
symptoms due to a mass effect.
Because of the pathologic variations of this tumor and the lack of pathognomic radiologic findings, making a definite preoperative diagnosis of retroperitoneal schwannoma is difficult.(2) But sometimes a preoperative pathological diagnosis can be made by ultrasonography or computed tomography guided needle biopsy. In addition, radiological imaging is helpful for treatment planning because it pro- vides information about a tumor’s size and location and its anatomical relationship with the retroperitoneal large vessels, and the possible tumor invasion to other struc- tures.(3)
The treatment of choice for retroperitoneal schwannomas is complete surgical excision.(4) A conventional open pro-
cedure has been traditionally used for resection of retro- peritoneal schwannomas, but the laparoscopic approaches are increasingly being applied. This is due to the many advantages of laparoscopic surgery, including early recovery, less pain, good cosmesis, a short hospital stay and an early return to normal activities because of its minimal inva- siveness. However, there have been discouraging opinions about using the laparoscopic approach to treat large retroperitoneal schwannomas such as the extended hospital stay and the technical difficulty.(5)
To the best of our knowledge, 15 cases of retroperitoneal schwannomas treated by laparoscopic surgery have been reported in the English medical literature.(5-19) For these cases, the tumor mean size was 4.8 cm (range: 2∼8 cm)
was 6.8 days (range: 1∼18 days). When comparing the duration of the hospital stay according to tumor size, the mean hospital stay was 8.9 days when the tumor size was over 5 cm and it was 3.3 days when the tumor size was less than 5 cm. Thus, the hospital stay was significantly longer when the tumor size was over 5 cm (P=0.0048). For this reason, some investigators have suggested that large retroperitoneal schwannomas are not suitable for the laparoscopic approach. They suggest that a large retro- peritoneal schwannomas may be managed effectively by conventional open surgery in terms of a reasonable post- operative hospital stay, and a shorter hospital stay was also noted in a recent report on a large retroperitoneal schw- annoma that was treated by the open approach.(5,19) Technically, laparoscopic resection of a large retro- peritoneal schwannomas has some difficulty for tumor retraction, dissecting around large vessels, and removing the resected tumor. However, retroperitoneal schwannomas are well circumscribed, they rarely invade to adjacent organs and large vessels, and they enveloped by dense connective tissue which makes retraction easier.(18) So, if great care is taken during dissecting near the large vessels, the laparo- scopic approach for a large retroperitoneal schwannomas can be performed safely.
When a large retroperitoneal schwannoma is resected via laparoscopic surgery, extending an incision is necessary for removing the tumor. However, the extension of the inci- sion reduces the advantages of laparoscopic surgery and it also makes the hospital stay longer. Considering that there were no postoperative complications in all the previous reported cases, we can presume that extension of the incision was one causes of the longer hospital stay for the patients whose tumor was 5 cm or larger. However, if proper methods are used (protect the wound and the skin to prevent seeding of tumor cells, divide the tumor into two pieces in the lap-bag before remove it, and change all the surgical instruments after the extraction), then exce- ssively extending the incision can be avoided and conse- quently, a long hospital stay can be prevented while
peritoneal schwannoma that was located adjacent to the great vessels, and this was successfully treated by laparo- scopic surgery without any postoperative complications or an extended hospital stay. This case suggests the indications for laparoscopic surgery can be widened to include treating large retroperitoneal schwannomas.
REFERENCES
1) Tortorelli AP, Papa V, Rosa F, Pacelli F, Doglietto GB. Image of the month--retroperitoneal schwannoma. Arch Surg 2006;
141:1259-61.
2) Sharma SK, Koleski FC, Husain AN, Albala DM, Turk TM.
Retroperitoneal schwannoma mimicking an adrenal lesion.
World J Urol 2002;20:232-3.
3) Tortorelli AP, Rosa F, Papa V, Rotondi F, Sanchez AM, Bossola M, et al. Retroperitoneal schwannomas: diagnostic and thera- peutic implications. Tumori 2007;93:312-5.
4) Nah YW, Suh JH, Choi DH, Ko BK, Nam CW, Kim GY, et al. Benign retroperitoneal schwannoma: surgical consideration.
Hepatogastroenterology 2005;52:1681-4.
5) Kang CM, Kim DH, Seok JY, Lee WJ. Laparoscopic resection of retroperitoneal benign schwannoma. J Laparoendosc Adv Surg Tech A 2008;18:411-6.
6) Melvin WS. Laparoscopic resection of a pelvic schwannoma.
Surg Laparosc Endosc 1996;6:489-91.
7) Nishio A, Adachi W, Igarashi J, Koide N, Kajikawa S, Amano J. Laparoscopic resection of a retroperitoneal schwannoma. Surg Laparosc Endosc Percutan Tech 1999;9:306-9.
8) Ohigashi T, Nonaka S, Nakanoma T, Ueno M, Deguchi N.
Laparoscopic treatment of retroperitoneal benign schwannoma.
Int J Urol 1999;6:100-3.
9) Behrend M, Kaaden S, Von Wasielewski R, Frericks B. Benign retroperitoneal schwannoma mimicking an adrenal mass. Surg Laparosc Endosc Percutan Tech 2003;13:133-8.
10) Descazeaud A, Coggia M, Bourriez A, Goeau-Brissonniere O.
Laparoscopic resection of a retroperitoneal schwannoma. Surg Endosc 2003;17:520.
11) Morrison KB, McAuley IW, Kinahan JF. Laparoscopic resection of a juxta-adrenal schwannoma. Can J Urol 2004;11:2309-11.
12) Funamizu N, Sasaki A, Matsumoto T, Inomata M, Shiraishi N, Kitano S. Laparoscopic resection of a retroperitoneal schwan- noma behind the lesser omental sac. Surg Laparosc Endosc Percutan Tech 2004;14:175-7.
13) Singh V, Kapoor R. Atypical presentations of benign retro- peritoneal schwannoma: report of three cases with review of literature. Int Urol Nephrol 2005;37:547-9.
14) Konstantinidis K, Theodoropoulos GE, Sambalis G, Georgiou M, Vorias M, Anastassakou K, et al. Laparoscopic resection of presacral schwannomas. Surg Laparosc Endosc Percutan Tech 2005;15:302-4.
15) Hori T, Yamagiwa K, Yagi S, Iida T, Taniguchi K, Yamamoto C, et al. Noradrenalin-secreting retroperitoneal schwannoma resected by hand-assisted laparoscopic surgery: report of a case.
Surg Today 2006;36:1108-13.
16) Inokuchi T, Takiuchi H, Moriwaki Y, Ka T, Takahashi S, Tsutsumi Z, et al. Retroperitoneal ancient schwannoma presen- ting as an adrenal incidentaloma: CT and MR findings. Magn
Reson Imaging 2006;24:1389-93.
17) Pinto D, Kaidar-Person O, Cho M, Zundel N, Szomstein S, Rosenthal RJ. Laparoscopic resection of a retroperitoneal degenerative schwannoma: a case report and review of the literature. Surg Laparosc Endosc Percutan Tech 2008;18:121-3.
18) Rao W, Wang G, Xiu D. Laparoscopic resection of a retro- peritoneal schwannoma adherent to vital vessels. Surg Laparosc Endosc Percutan Tech 2009;19:e21-3.
19) Daneshmand S, Youssefzadeh D, Chamie K, Boswell W, Wu N, Stein JP, et al. Benign retroperitoneal schwannoma: a case series and review of the literature. Urology 2003;62:993-7.