An inflammatory myofibroblastic tumor (IMT), or in- flammatory pseudotumor, is a relatively rare quasineo- plastic lesion consisting of inflammatory cells and my- ofibroblastic spindle cells. The exact etiology of an IMT is unknown and whether an IMT represents a reactive or neoplastic process remains unclear. An IMT was ini- tially described in the lung, but it has subsequently been found to potentially involve nearly all areas of the body (1-3). An IMT usually presents as a single mass within a single organ or sometimes as multifocal lesions within a single anatomic region. An IMT involving noncontigu- ous multi-organs is extremely rare (4, 5).
We present a case of an aggressive IMT that involves multiple organs within different anatomic regions.
Case Report
A 68-year-old man presented with a one-week history of right lower extremity weakness and lower back pain.
The patient had no trauma history. The laboratory data revealed only a mild elevation of ESR (18 mm/hr) and a minor degree of thrombocytosis with a platelet count of 525,000 platelets/μl. MR imaging showed irregular bony destructive soft tissue masses involving the body and right pedicle of the L2 vertebra, with expansion to the epidural space and the ipsilateral neural foramen (Fig.
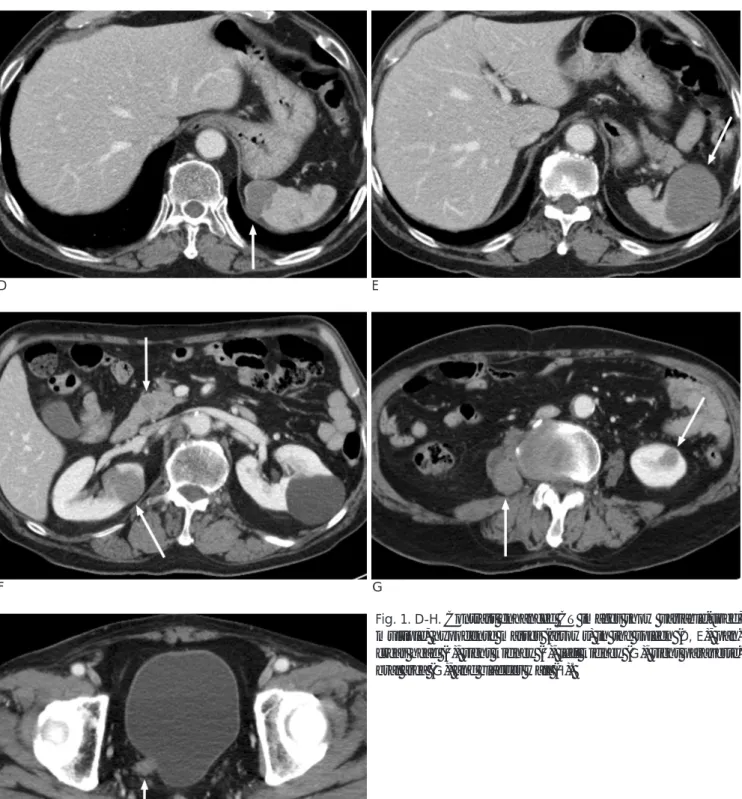
1A-C). Since the lesion was considered a metastasis, we performed a diagnostic work-up to find the primary ma- lignancy. A contrast-enhanced abdominopelvic CT scan demonstrated the presence of multiple nodules in the spleen, both kidneys, pancreas, right paravertebral, and bladder wall (Fig. 1D-H). From brain MR imaging, a 1.5 cm, well enhanced mass was noted that extended from the hypothalamus to the pituitary stalk.
Non-contiguous Multi-organ Involvement of an Inflammatory Myofibroblastic Tumor: A Case Report1
Jae-Wook Lee, M.D., Ki Whang Kim, M.D. , Kyung-Mi Paek, M.D., Mi-Suk Park, M.D., Jae-Yeon Seok, M.D.2, Sungjun Kim, M.D.3, Myeong-Jin Kim, M.D.
1Department of Diagnostic Radiology, Yonsei University College of Medicine, Research Institute of Radiological Science, Yonsei University College of Medicine
2Department of Pathology, Yonsei University College of Medicine
3Department of Diagnostic Radiology, Hanyang University Medical Center
Received April 12, 2006 ; Accepted August 2, 2006
Address reprint requests to : Ki Whang Kim, M.D., Department of Diagnostic Radiology, Severance Hospital, Seodaemun-gu, Shinchon- dong 134, Seoul 120-752, Republic of Korea
Tel. 82-2-2228-7400 Fax. 82-2-393-3035 E-mail: [email protected]
An inflammatory myofibroblastic tumor (IMT) is relatively rare quasineoplastic le- sion. An IMT usually presents as a single mass within a single organ or sometimes as multifocal lesions within a single anatomic region. An IMT involving noncontiguous multi-organs within different anatomic regions is extremely rare. We present a case of an aggressive IMT that involved the musculoskeletal system and multiple abdominal visceral organs.
Index words :Computed tomography (CT)
Magnetic resonance (MR), image display Abdomen, CT
Spine, MR
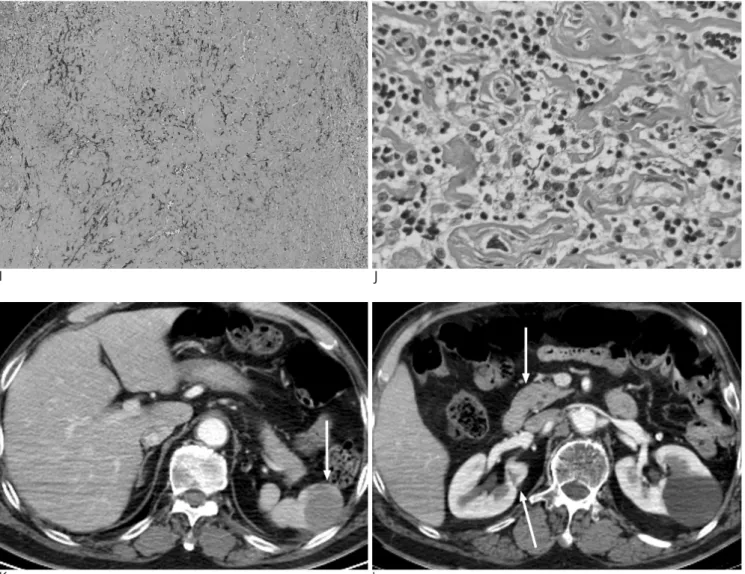
The patient underwent an excisional biopsy for the le- sion in the L2 vertebra. An microscopic examination re- vealed diffuse dense collagenous fibrosis admixed with intervening, mature looking lymphoid cells and plasma cells, which is consistent with an IMT (Fig. 1I, J). An ad- ditional ultrasound-guided biopsy of the splenic mass re- vealed the same microscopic findings as the L2 vertebral lesion, therefore enabling the conclusion of the same di- agnosis of an IMT. Thirteen months after discharge, the patient received a follow-up abdominopelvic CT and brain MRI. A contrast enhanced CT scan showed a de- crease in the size of the nodules in the spleen, and no residual masses were noted in the kidneys and pancreas (Fig. 1K, L). From the brain MRI, no mass was demon- strable in the hypothalamic area.
Discussion
An inflammatory myofibroblastic tumor, also known
as an inflammatory pseudotumor, is defined as “a tumor composed of differentiated myofibroblastic spindle cells usually accompanied by numerous plasma cells and/or lymphocytes” by the 1994 WHO Classification of Soft Tissue Tumors (6). Coffin et al. (1) subdivided this rare tumor type into three histological subtypes: myxoid-vas- cular, hypocellular fibrous, and the compact spindle cell type. The tumor mainly affects young patients and most often involves the lung and the orbit, but may occur in virtually any anatomic location and at any age.
Whereas the exact etiology of an IMT is unknown, an IMT has been thought to result from inflammation fol- lowing trauma, surgery, or acute infection. Other inves- tigators argue that an IMT is a true neoplastic lesion.
Some IMT cases with malignant transformation or metastasis to distant organs have been demonstrated in the literature (2). There are only sporadic descriptions of the radiological findings for IMT in the medical litera- ture and the reported findings are variable depending on
A B
Fig. 1. A-C. MR imaging demonstrates the mass destroying the L2 vertebral body and the right pedicle, and expanding to the epidural space and the neural foramen. The mass shows hetero- geneous hypo- and hyperintensity on the axial T2-weighted im- age (A) and isointensity on the T1-weighted image (B). The post- contrast T1-weighted image (C) reveals a well-enhanced lesion.
the involved organ, histological subtype, and are even inconsistent within the same organ (3, 4).
IMT bone involvement is extremely rare, and the gen- eral imaging features of this involvement have not been well described (7, 8). In our case, a bony lesion demon-
strated heterogeneous signal intensity on T2WI, homo- geneous iso-signal intensity on T1WI, and heteroge- neously well-enhanced intensity on gadolinium-en- hanced T1WI with expansion to the epidural space and the neural foramen. These findings cannot be differenti-
D E
F G
H
Fig. 1. D-H. Contrast enhanced CT images show variable-sized, multiple, hypodense masses (arrows) in the spleen (D, E), pan- creas head (F), right kidney (F), left kidney (G), right paraverte- bral area (G), and bladder wall (H).
ated from a metastasis or other primary bone tumors.
The MR findings of IMT may be low to intermediate sig- nal intensity on T1- and variable signal intensity on T2- weighted images and possible strong enhancement with gadopentetate dimeglumine (3). Han et al. (9) suggested that the T2 hypointensity of a soft-tissue lesion might be explained by a relative lack of both free water and mo- bile protons within the fibrotic lesions. Hoger et al. (4) reported a case of synchronous IMTs with different sub-
An IMT has been reported in various sites within the abdomen, including the liver, spleen, pancreas, adrenal gland, kidney, retroperitoneum, diaphragm, mesentery, and the alimentary and urinary tracts. An IMT has a variable CT appearance. On un-enhanced scans, the mass may be hypoattenuated or isoattenuated relative to the muscle, with or without calcification. Enhancement with contrast material administration frequently occurs and is not pronounced and a variety of patterns has
I J
K L
Fig. 1. I, J. Diffuse, dense collagenous fibrosis admixed with intervening, mature looking lymphoid cells and plasma cells, which are consistent with IMT histology (H & E staining, I: ×40, J: ×400).
K, L. Follow-up contrast enhanced CT images show a decrease in the size of the masses (arrows) in the spleen (K), left kidney (L), and pancreas (L).
we assume that the IMT also involved the kidneys, pan- creas, paravertebral area, bladder wall, and brain. In ad- dition, all of the lesions involving the intra-abdominal organs were homogeneous iso- or hypo-attenuated masses relative to the muscle on contrast-enhanced CT.
The density and enhancement patterns of this case were similar to those described in previous reports. However, the radiological findings in this case were nonspecific and the lesions could not be differentiated from a lym- phoma, melanoma, or other metastatic or multi-organ involved lesions.
In conclusion, this case certifies that this rare entity may demonstrate non-contiguous, multi-organ involve- ment, aggressive growth patterns, and variable signal in- tensities. In addition, this case shows inconsistent en- hancement with MR and CT imaging. Therefore, when dealing with such cases, an IMT should be included as a potential differential diagnosis, even though these cases are very rare.
References
1. Coffin CM, Watterson J, Priest JR, Dehner LP. Extrapulmonary in- flammatory myofibroblastic tumor (inflammatory pseudotumor).
A clinicopathologic and immunohistochemical study of 84 cases.
Am J Surg Pathol 1995;19:859-872
2. Dehner LP. The enigmatic inflammatory pseudotumours: the cur- rent state of our understanding, or misunderstanding. J Pathol 2000;192:277-279
3. Narla LD, Newman B, Spottswood SS, Narla S, Kolli R.
Inflammatory pseudotumor. Radiographics 2003;23:719-729 4. Horger M, Pfannenberg C, Bitzer M, Wehrmann M, Claussen CD.
Synchronous gastrointestinal and musculoskeletal manifestations of different subtypes of inflammatory myofibroblastic tumor: CT, MRI and pathological features. Eur Radiol 2005;15:1713-1716 5. Di Vita G, Soresi M, Patti R, Carroccio A, Leo P, Franco V, et al.
Concomitant inflammatory pseudotumor of the liver and spleen.
Liver 2001;21:217-222
6. Weiss SW. Histological Typing of Soft Tissue Tumours. 2nd ed. Berlin:
Springer-Verlag, 1994
7. Sciot R, Dal Cin P, Fletcher CD, Hernandez JM, Garcia JL, Samson I, et al. Inflammatory myofibroblastic tumor of bone: report of two cases with evidence of clonal chromosomal changes. Am J Surg Pathol 1997;21:1166-1172
8. Allanore Y, Pham XV, Clerc DA, Menkes CJ, Kahan A. Sacral in- flammatory pseudotumor revealed by paraneoplastic syndrome.
Rheumatol Int 2004;24:166-168
9. Han MH, Chi JG, Kim MS, Chang KH, Kim KH, Yeon KM, et al.
Fibrosing inflammatory pseudotumors involving the skull base:
MR and CT manifestations with histopathologic comparison.
AJNR Am J Neuroradiol 1996;17:515-521
대한영상의학회지 2007;57:265-269
비연속적으로 다수의 장기에 발생한 염증성 근섬유모세포성 종양:
증례 보고1
1연세대학교 의과대학 영상의학과
2연세대학교 의과대학 병리학교실
3한양대학교 의과대학 영상의학과
이재욱・김기황・백경미・박미숙・석재연2・김성준3・김명진
염증성 근섬유모세포성 종양(inflammatory myofibroblastic tumor)은 상대적으로 드문 유사신생물로 일반적으로 단일 장기에 단일 병변, 또는 가끔 단일 해부학 영역에서 다수 병변으로 발견된다. 하지만, 다른 해부학적 영역에서 비연속적으로 다수의 장기에서 발생하는 경우는 매우 드물다. 이에 저자들은 근골격계와 다수의 복강 내 장기에 발 생한 염증성 근섬유모세포성 종양의 증례를 보고한다.