Korean Journal of HBP Surgery Vol. 6, No. 2, December, 2002
128
서 론투명 세포 간세포암은 헤마톡실린-에오신 염색에서 염색 되지 않는 투명한 세포질을 갖는 다수의 종양 세포로 구성 된 간세포암의 변형된 형태로 전체 간세포암의 약 8.7∼
25%를 차지한다.1-16) 이러한 특이한 세포학적 형태로 인해 그 특성에 대한 다양한 보고가 있어 왔고 adrenal nest tumor, hepatic hypernephroma, regenerative hepatic hyperplasia, he- patic adenoma로 불려 왔다.1-3) 그 예후에 대해서는 간 침범 범위가 넓은 경우에도 생존율이 양호하다는 보고가 있는2)
반면, 최근에는 생존율에 유의한 차이가 없다는 보고도 있 어3) 저자들은 간세포암에서 투명 세포군과 정형 세포군 의 임상병리학적 특성을 비교하여 투명 세포 간세포암의 특징을 이해하는 데 도움이 되고자 하였다.
1992년 1월부터 1997년 12월까지 서울대학교병원 외과에 서 간세포암으로 근치적 절제술을 시행 받은 환자 537명을 대상으로 정형 세포군과 투명 세포군 간의 임상병리학적 특성을 비교 분석하였다.
대상 및 방법
1992년 1월부터 1997년 12월까지 서울대학교 병원 외과 에서 근치적 간절제술을 시행 받은 537명 중 방추 세포군 2명을 제외한 535명을 대상으로 하였다. 의무기록을 분석 한 후향적 연구를 진행하였고 The Chi-square test, Student T-test, Kaplan-Meier test를 이용하여 통계 분석하였다. 임상
투명 세포 간세포암의 임상병리학적 고찰
서울대학교 의과대학 외과학교실
강민관․이혁준․장성환․최석호․서경석․이건욱
Clinicopathologic Study on Clear Cell Hepatocellular Carcinoma
Min Kwan Kang, M.D., Hyuk-Joon Lee, M.D., Sung-Hwan Chang, M.D., Seok Ho Choi, M.D., Kyung-Suk Suh, M.D., and Kuhn Uk Lee, M.D.
Department of Surgery, Seoul National University College of Medicine, Seoul, Korea
Background: Clear cell hepatocelluar carcinoma (CHCC) is
a well defined type of hepatocellular carcinoma (HCC) in which a large number of tumor cells have clear cytoplasm that is not stained by hematoxylin and eosin stain. It is generally reported that CHCC has a favorable prognosis compared with that of conventional non-CHCC.1 The reasons for the better prognosis are not clear. To date the clini- copathologic features of CHCC of the liver have not been fully elucidated. In the present study we compared the clinico- pathologic features of 56 cases of CHCC with those of 479 cases of non-CHCC and report here hoping to further under- standing of CHCC.Methods: 535 consecutive cases that were curatively
resected from Jan. 1992 to Dec. 1997 in Seoul NationalUniversity Hospital were reviewed. The cases were divided into clear cell HCC (56 cases) and non-clear cell HCC (479 cases). Clinical and pathological findings were compared between two groups.
Results: Clinically there is no significant difference in sex &
age, preoperative liver function, the association rate with liver cirrhosis, the extent of resection. Pathologically there is no significant difference in tumor size, capsule formation, portal vein invasion, the differentiation of tumor. Three- and five- year survival rates of clear cell HCC were 55.3%, 42.8%, respectively, lower than the finding of 68.4%, 54.4% for non-clear cell HCC. But there is no significant difference in prognosis between both groups (p=0.13). The multiplicity rate (tumor number≥2) of clear cell HCC was 3.8% (2/56), lower than the finding of 13.1% (62/479) for non-clear cell HCC.
(p<0.05)
Conclusion: It was concluded that clear cell HCC has no
significant difference in clinicopathologic features except tumor number. (Korean J HBP Surg 2002;6:128-131)ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Clear cell hepatocellular carcinoma, Hepato-
cellular carcinoma
중심 단어: 투명세포 간세포암, 간세포암
책임저자:서경석, 서울특별시 종로구 연건동 28
ꂕ 110-744, 서울대학교병원 외과
Tel: 02-760-3789, Fax: 02-745-2282
E-mail: [email protected]
강민관 외:투명 세포 간세포암의 임상병리학적 고찰 129 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
적 특징으로는 성별, 연령, 간염 및 간경변 동반 여부, 수술전 간기능(차일드 분류), 수술 방법의 차이를 비교 하였다.
병리학적 특징으로는 종양의 크기, 개수, 피막 형성 여부, 문맥 침범 여부, 분화도의 차이를 비교하였다.
결 과
1. 임상적 특징(Table 1)
1) 성별 및 연령: 평균 연령은 정형 세포군이 52.6±9.6세, 투명 세포군이 51.0±11.2세였다. 남녀의 비는 정형 세포군 이 4.9:1, 투명 세포군이 4.6:1이었다. 성별과 연령에 있어 서 두 군 간의 유의한 차이를 보이지 않았다.
2) 간염 및 간경변 동반 여부: 병리 조직 검사상 절제된 정상 간 조직이 경변성 변화를 가진 경우가 정형 세포군에 서는 284/479 (59.3%), 투명 세포군은 20/56 (50.0%)로 유의 한 차이를 보이지 않았다.
B형 간염이 동반된 경우가 정형 세포군은 361/479 (75.4%), 투명 세포군이 43/56 (76.8%)였고 C형 간염이 동반된 경우 는 정형 세포군이 61/479 (12.7%), 투명 세포군이 6/56 (10.9%)로 간염 동반 여부에 있어 두 군간의 유의한 차이는 없었다.
3) 수술 전 간기능: 수술 전 간기능으로 차일드 분류에 따라 분류하였다. Child A, B, C인 경우가 정형 세포군은 각각 334 (69.7%), 121 (25.3%), 24 (5%), 투명 세포군은 각각 42 (75%), 12 (23.2%), 1 (1.8%)로 수술 전 간기능에 있어서 도 두 군간의 유의한 차이는 없었다.
4) 수술 방법: 엽절제술 이상의 수술을 한 경우가 정형 세포군이 61/479 (12.7%), 투명 세포군이 9/56 (16.1%)로 수
술 방법의 차이는 없었다.
2. 병리학적 특징(Table 2)
1) 크기: 종양의 평균 크기는 정형 세포군이 4.48±2.94 (cm), 투명 세포군이 4.41±2.30 (cm)으로 두 군간의 유의한 차이는 보이지 않았다.
2) 개수: 종양이 두 개 이상인 경우가 정형 세포군이 62/479 (13.1%), 투명 세포군이 2/56 (3.8%)로 투명 세포군이 한 개의 종양만 형성하는 경우가 유의하게 많았다(p<0.05).
3) 피막 형성: 종양이 피막을 형성하는 경우가 정형 세포 군이 127/479 (26.5%), 투명 세포군이 14/56 (25.0%)로 두 군 간의 유의한 차이가 없었다.
4) 문맥 침범: 수술 소견 및 병리 검사 결과 문맥 침범이 있었던 경우가 정형 세포군이 48/479 (10.1%), 투명 세포군 이 4/56 (7.7%)로 두 군간의 유의한 차이가 없었다.
5) 분화도: 종양 세포의 분화도는 고, 중등도, 저분화도로 구분하였는데 정형 세포군이 각각 31 (8.3%): 236 (62.9%):
108 (28.8%), 투명 세포군이 각각 5 (9.1%): 28 (50.9%): 22 40.0%)로 두 군 모두 중등도의 분화도를 나타내는 경우가 가장 많았다.
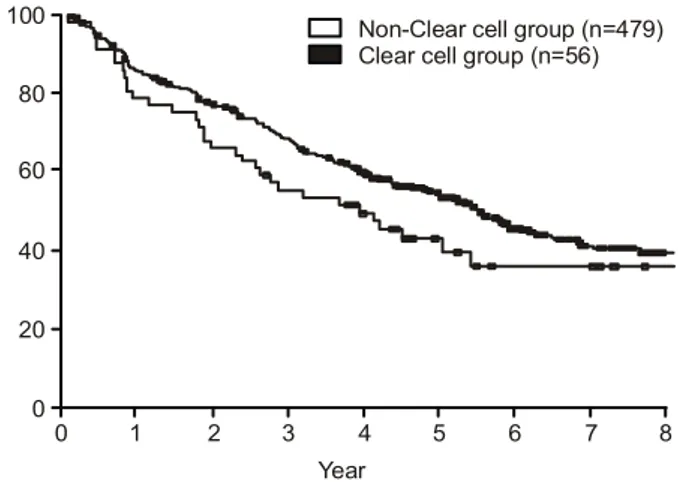
3. 생존율(Fig 1, 2)
전체 생존율은 정형 세포군이 평균 67.5±2.3개월이었고 3, 5년 생존율은 각각 68.4%, 54.4%였다. 투명 세포군은 평 균 56.8±5.8개월이었고 3, 5년 생존율은 각각 55.3%, 42.8%였다.
무병 생존율은 정형 세포군이 평균 58.5±1.9개월이었고 3, 5년 무병 생존율이 각각 68.9%, 49.6%였다. 투명 세포군 은 평균 50.7±5.1개월이었고 3, 5년 무병 생존율은 각각 55.3%, 38.3%였다.
투명 세포군이 정형 세포군에 비해 무병 생존율과 생존율 에 있어 보다 불량한 예후를 보이는 경향이 있으나 이는 통계학적으로 유의한 차이를 보이지 않았다.
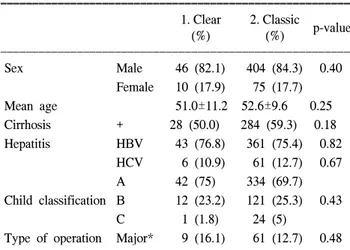
Table 1. Comparison of clinical characteristics between clear cell HCC and Classic HCC
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ 1. Clear 2. Classic
p-value
(%) (%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Sex Male 46 (82.1) 404 (84.3) 0.40
Female 10 (17.9) 75 (17.7)
Mean age 51.0±11.2 52.6±9.6 0.25
Cirrhosis + 28 (50.0) 284 (59.3) 0.18
Hepatitis HBV 43 (76.8) 361 (75.4) 0.82
HCV 6 (10.9) 61 (12.7) 0.67
A 42 (75) 334 (69.7)
Child classification B 12 (23.2) 121 (25.3) 0.43 C 1 (1.8) 24 (5)
Type of operation Major* 9 (16.1) 61 (12.7) 0.48 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*Major operation = left lateral sectionectomy, left (or right) hemi- hepatectomy, left (or right) trisectionectomy 1. Clear cell hepato- cellular carcinoma; 2. Classic hepatocellular carcinoma
Table 2. Comparison of pathologic characteristics between clear cell HCC and classic HCC
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ 1. Clear (%) 2. Classic (%) p-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Mean size (cm) 4.41±2.30 4.48±2.94 0.86
Number ≥2 2 (3.8) 62 (13.1) <0.05
Capsule + 12 (27.5) 127 (26.5) 0.83
PV* invasion + 4 (7.7) 48 (10.1) 0.58 Well 5 (9.1) 31 (8.3)
Differentiation Mod. 28 (50.9) 236 (62.9) 0.21 Poor 22 (40.0) 108 (28.8)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*PV = portal vein. 1. Clear cell hepatocellular carcinoma; 2. Clas-
sic hepatocellular carcinoma
130 한국간담췌외과학회지:제 6 권 제 2 호 2002
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
고 찰
투명 세포 간세포암은 헤마톡실린-에오신 염색에서 염색 되지 않는 투명한 세포질을 갖는 다량의 세포로 구성된 간 세포암의 한 형태를 말한다.1-16) 이 투명 세포 간세포암의 임상병리학적 특징에 대한 다양한 연구가 있었으나 아직까 지 그 특성이 명확히 밝혀지지 않은 상태이다. 이 세포의 세포질은 다량의 글라이코겐과 지질을 함유하고 있어 일반 염색에서 염색되지 않는 것으로 알려져 있고 그 예후에 대 해서는 서로 다른 결과를 보고하고 있다.1-16) Edmonson은 투 명 세포 간세포암은 원격 전이를 하지 않고 양호한 예후를 보인다고 처음으로 보고했다.2)
이후 Buchannan 등은 투명 세포 간세포암은 전체 간세포 암의 8.7%를 차지하며, 남녀의 비는 1.6:1로 여자에 비교 적 많고 다른 형태의 간세포암에 비해 예후에 있어 차이가 없음을 보고 했다.3)
Lai 등은 투명 세포 간세포암을 미만형(diffuse pattern)- 전체 세포 중 50% 이상을 차지하는 경우, 국소형(focal pattern)-전체 세포 중 약 30%를 차지하는 경우로 구분하였 고, 이는 각각 전체 간세포암의 12.5%, 25%를 차지한다고 보고했다.1) 그리고 전체 세포 중 투명 세포 간세포암은 광 범위한 침범이 있더라도 양호한 예후를 보이고, 전체 세포 중 차지하는 비율이 높을수록 보다 양호한 예후를 보인다 고 보고했다.1) Yang 등은 투명 세포 간세포암은 대부분 중 등도 분화도를 보이며, 남녀의 비는 2.3:1로 상대적으로 여자에 많고 예후에 있어서는 다른 형태의 간세포암과 차 이가 없음을 보고했다. 여자에서 많은 경향에 대해서는 아 마 성호르몬이 관여할 것으로 생각했고 이는 세포의 형태 학적 변화에도 관계가 있을 것으로 해석했다.5) 본 연구에서 는 투명 세포 간세포암은 전체의 10.4%를 차지했는데, 이는 Buchannan과 Lai의 보고와 차이가 없었다. 남녀의 비는 4.9:1로 정형 세포군의 4.6:1과 유의한 차이가 없었다. 이
는 여자에서 많은 비율을 보인다는 Buchannan과 Yang의 보 고와는 다른 결과이다. Yang 등은 간경변과 동반되는 비율 이 높다고 보고했으나5) 본 연구에서는 간염 및 간경변 동반 여부는 정형 세포군과 차이가 없었다. 수술 전 간기능 및 수술 방법에 있어서도 차이를 보이지 않았다. 병리학적 특 성에 있어서도 크기, 문맥 침범, 분화도의 차이도 보이지 않 았다. 다른 연구에서와 같이 중등도의 분화도의 비율이 50.9%로 가장 많은 비율을 차지했다. 투명 세포 간세포암이 한 개의 종양을 형성하는 경우가 많았다. 무병 생존율과 전 체 생존율은 투명 세포 간세포암에서 오히려 불량한 예후 를 보이는 경향을 나타냈으나 유의한 차이는 없었다. 이상 의 결과를 볼 때 투명 세포 간세포암은 종양의 개수가 적은 것 이외에는 특이한 임상병리학적 특성을 보이지 않았다.
전체 56명의 투명 세포 간세포암 환자 중 두 개 이상의 종양 이 있었던 경우가 단 2명뿐으로 이는 정형 세포 간암에 비 해 유의하게 개수가 적은 결과를 나타냈으나 연구 대상이 56명과 479명으로 큰 차이가 있어 유의한 차이로 보기는 어 려울 듯하다. 투명 세포 간세포암은 그 특이한 세포학적 특 징으로 인해 다양한 연구가 진행되어 왔으나, 본 연구에서 는 단지 세포학적 한 형태일 뿐 임상적으로나 예후에 있어 서 어떠한 영향을 미치지 않는 것으로 나타났다. 그러나 다 수의 연구들이 투명 세포의 비율에 따라 미만형과 국소형 으로 구분하여 비교한 반면,1) 본 연구는 이를 통합하여 하 나의 투명 세포 간세포암으로 구분하였다. 따라서 전체 세 포 중 투명 세포가 차지하는 비율에 따른 임상 병리적 특징 을 구분하지는 못 하였다. 앞으로 보다 많은 증례와 자세한 세포 병리학적 검사를 통한 투명 세포 간세포암의 특성과 예후를 밝혀야 할 것이다.
Fig. 1. Overall survival rate curve. Fig. 2. Disease free survival rate curve.
0 100
8 Year
0
Clear cell group (n=56) Non-Clear cell group (n=479)
6 5 4 3 2 1 80 60 40 20
7
강민관 외:투명 세포 간세포암의 임상병리학적 고찰 131 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
참 고 문 헌